
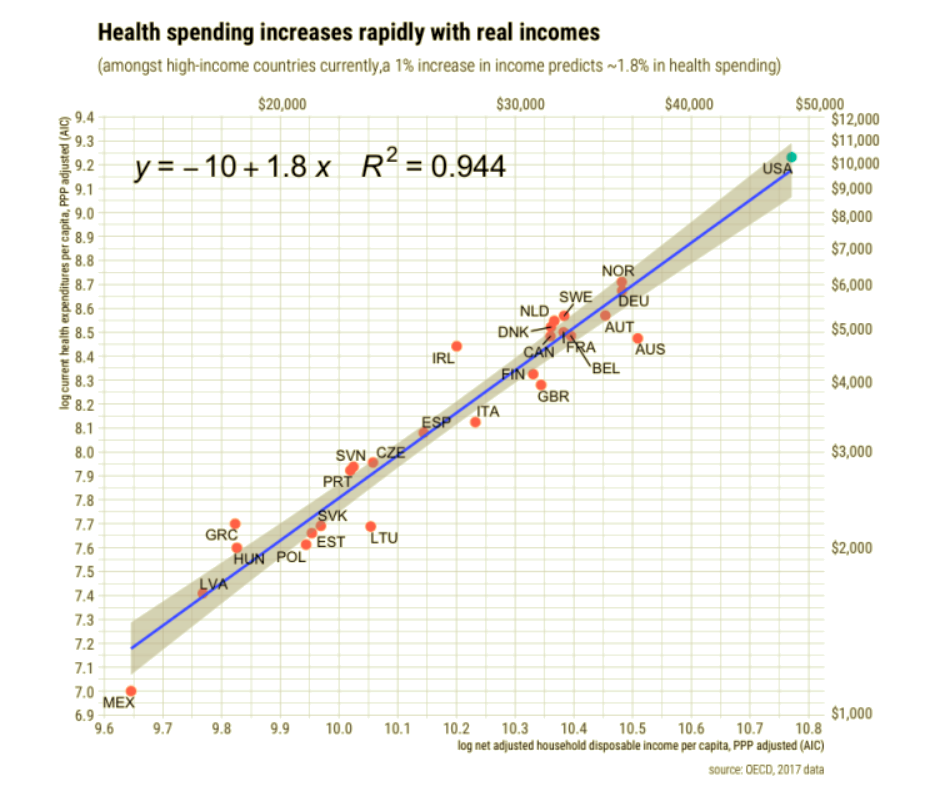
U.S. health care spending is not out-of-line internationally, despite whatever shortfalls our health care system might embody. By that, I mean that health care spending is almost exactly what U.S. income levels would predict based on cross-country statistical evidence. Other countries are certain to spend more as their own incomes grow. Take another look at the relationship shown in the chart above: it predicts that health care spending per capita grows 1.8% for every 1% increase in household income. In fact, the share of consumption devoted to health care rises as income rises. Quite simply, the slope of that curve means that health care qualifies as a luxury good.
The chart and conclusions above come from an exhaustive analysis at the Random Critical Analysis (RCA) blog, which is also summarized nicely by Alex Tabarrok at Marginal Revolution (to whom I owe a debt of gratitude for several great topics of late). The analysis goes further in asserting that income causes health care spending.
“When real income changes, health spending responds in a manner that is consistent with cross-sectional results…. It takes 3-4 years for payers and for providers to completely respond through reimbursement policy, premiums, services offered, and so on. Still, the strength of the long-run relationship is nonetheless readily apparent in the US time series. … Comparable results are obtained in OECD data with similar household income measures.”
So we spend more on health care because we can and, in a strong sense, because we want to. And here is an interesting wrinkle: we actually consume more health care services, we don’t just pay higher prices. Health care prices do increase with income, but at a slower rate than income. This implies that higher quantities of health care are delivered in high-income countries. As the post at RCA notes, health care prices in the U.S. are not “inexplicably high”.
If you visit the post at RCA, note that it’s very easy to browse between sub-topics from the list of sub-links on the right. The analysis covers many other nuances. I’ll mention one more very important one, which is emphasized by Tabarrok: our high level of health care consumption does not involve a loss of goods consumed from other sectors. In fact, quite the opposite. The prices of most goods and services have declined relative to income over the years:
“The typical American household is much better fed today than in prior generations despite spending a much smaller share of their income on groceries and working fewer hours. I submit this is primarily a direct result of productivity. We can produce food so much more efficiently that we don’t need to prioritize it as we once did. The food productivity dividend, as it were, has been and is being spent on higher-order wants and needs like cutting edge healthcare, higher amenity education, and leisure activities. … Similar patterns have doubtless been playing out in other essential consumption categories.
… these trends indicate that the rising health share is robustly linked with a generally constant long-term of increasing in real consumption across essentially all other major consumption categories.”
The share of income dedicated to health care in the U.S. is not a dysfunction in the health care sector, nor is it reflective of any dysfunction. That doesn’t mean there are no dysfunctions, however: our health insurance system severs the economic link between consumers and providers, nullifying the price incentives that normally yield effective market outcomes. price transparency is a casualty of the system as well; flaws in the Affordable Care Act create incentives for consolidation in health care delivery, undermining competitive forces; and tax deductibility of employer-provided coverage is a subsidy to those best able to pay for medical expenses and health care coverage.
There is no doubt that these peculiarities lead to suboptimal combinations of services and outcomes. I have written about that in several posts, including “Hospital Price Insanity” in December of 2019. Certain services are vastly overpriced; utilization levels suggest that expensive technology is unnecessarily duplicated; resources are over-allocated to medical tests as well as emergency rooms; and certain markets are underserved. As for outcomes, comparisons are difficult given the lifestyle issues that feed demand for health care in the U.S., such as obesity and smoking. This point too is treated in the long post at Random Critical Analysis.
Other health care systems certainly have their own dysfunctions (see my post “Single Payer: Queue Up and Die Already“, from January). There are undoubtedly wasteful misallocations of resources and lost opportunities for improvements in care in all these systems. But in terms of the share of resources we dedicate to health care, our system places us at a point along the same locus toward which other developed nations converge: health care spending is reliably related to income. There are problems, but that is not one of them.
