Tags
All-Cause Mortality, American Academy of Pediatrics, American Association of Sciences, Asian Flu, Covid-19, David Zaruk, Engineering and Medicine, Hydroxychloraquine, Infection Fatality Rate, Mollie Hemingway, Precautionary Principle, Spanish Flu, The Risk Monger, Tyler Cowen, Wired

Perhaps life in a prosperous society has sapped our ability and willingness to face risks. This tendency undermines that very prosperity, however. If we ever needed an illustration, the hysteria surrounding COVID-19 surely provides it. Do we really know how to exist in a world with risk anymore? During this episode, the media, public officials, and much of the public have completely lost their bearings with respect to the evaluation of risk, acting as if they are entitled to a zero-risk existence. Of course, COVID-19 is highly transmissible and dangerous for certain segments of the population, but it is rather benign for most people.
Perspective On C19 Risks
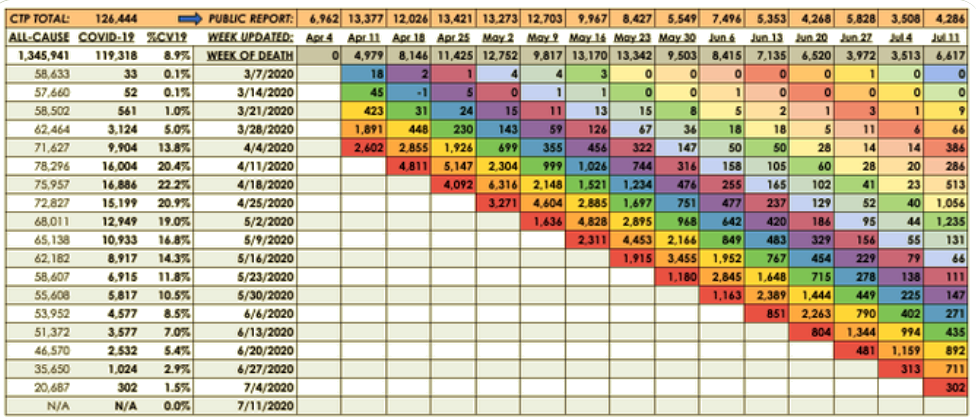
Just for starters, the table at the top of this post (admittedly not particularly well organized) shows calculations of odds from the CDC. These odds might well overstate the risks of both C19 and the flu, as they probably don’t account well for the huge number of asymptomatic cases of both viruses.
Another glimpse of reality is offered by a recent Swiss study showing the C19 infection mortality rate (IFR) by age, shown below. You can find a number of other charts on-line that show the same pattern: If you’re less than 50 years old, your risk of death from C19 is quite slim. Even those 50-64 years of age don’t face a substantial mortality risk, though it’s obviously higher for individuals having co-morbidities. These IFRs are lower than all-cause mortality for younger cohorts, but higher for older cohorts.

And here are a few other facts to put the risks of C19 in perspective:
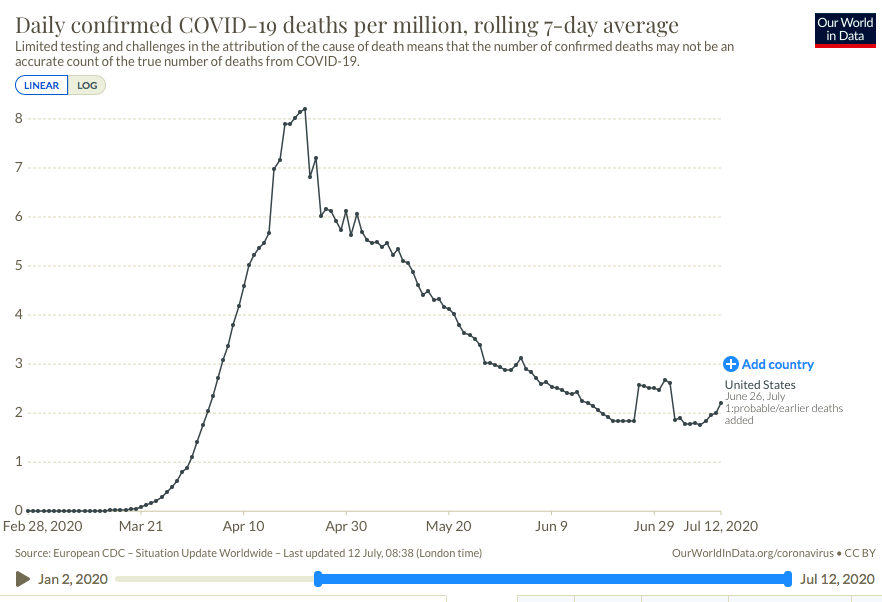
- The current pandemic is relatively benign: thus far, the U.S. has suffered a total of about 145,000 deaths, or 440 per million of population;
- the Asian Flu of 1957-58 took 116,000, according to the CDC, or 674 per million;
- the Spanish Flu of 1917-18 took 675,000 U.S lives, or 6,553 per million.
It should be obvious that these risks, while new and elevated for some, are not of such outrageous magnitude that they can’t be managed without bringing life to a grinding halt. That’s especially true when so-called safety measures entail substantial health risks of their own, as I have emphasized elsewhere (and here).
The Schools
Nothing illustrates our inability to assess risks better than the debate over reopening schools. This article in Wired is well-balanced on the safety issue. It emphasizes that there is little risk to teachers, students, or their families from opening schools if reasonable safety measures are taken.
Children of pre-school and elementary school age do not contract the virus readily, do not transmit the virus readily, and do not readily succumb to its effects. This German study on elementary schools demonstrates the safety of reopening. It is similar to the experience of other EU countries that have reopened schools. This article reinforces that point, but it emphasizes measures to limit any flare-ups that might arise. And while it singles out Israel as an example of poor execution, it fails to offer any evidence on the severity of infections.
Furthermore, we should not overlook the destructive effects of denying in-classroom learning to children. They simply don’t learn as well on-line, especially students who struggle. There are also the devastating social-psychological effects of the isolation experienced by many elementary school children during extended school closures. This is of a piece with the significant risks of lockdowns to well being. Perhaps not well known is that schooling is positively correlated with life expectancy: this study found that a one-year reduction in years of schooling is associated with a reduction in life expectancy of 0.6 years!
It’s true that children older than 10 might pose somewhat greater risks for C19 contagion, but those risks are manageable via hygiene, distancing, and other mitigations including hydroxychloraquine or other prophylaxes against infection for teachers who desire it. Capacity limitations might well require a temporary mix of online and in-school learning, but at least part-time attendance at brick-and-mortar schools should remain the centerpiece.
As Tyler Cowen points out, teenagers are less likely to remain isolated from others during school closures, so their behavior might be more difficult to manage. It’s quite possible they could be more heavily exposed outside of school, hanging out with friends, than in the classroom. This illustrates how our readiness to demure from absolute risk often ignores the pertinent question of relative risk.
Judging by reactions on social media, people are so frightened out of their wits that they cannot put these manageable risks in perspective. But here is a statement from the American Academy of Pediatrics. And here is a statement from the American Association of Sciences, Engineering and Medicine. They speak for themselves.
Excessive Precautionary Putzery
Our reaction to C19 amounts to a misapplication of the precautionary principle (PP), which states, quite reasonably, that precautionary measures must be invoked when faced with a risk that is not well understood. Risk must be managed! But what are those precautions and on what basis should benefits we forego via mitigation be balanced against quantifiable risks. That was one theme of my post “Precaution Forbids Your Rewards” several years back. Ralph B. Alexander discusses the PP, noting that the construct is vulnerable to political manipulation. It is, unfortunately, a wonderful devise for opportunistic interest groups and interventionist politicians. See something you don’t like? Identify a risk you can use to frighten the public. Use any anecdotal evidence you can scrape together. Start a movement and put a stop to it!
That really doesn’t help us deal with risk in a productive way. Do we understand that well being generally is enhanced by our willingness to incur and manage risks? As David Zaruk, aka, the Risk Monger, says, “our reliance of the precautionary principle has ruined our ability to manage risk.”:
“Two decades of the precautionary principle as the key policy tool for managing uncertainties has neutered risk management capacities by offering, as the only approach, the systematic removal of any exposure to any hazard. As the risk-averse precautionary mindset cements itself, more and more of us have become passive docilians waiting to be nannied. We no longer trust and are no longer trusted with risk-benefit choices as we are channelled down over-engineered preventative paths. While it is important to reduce exposure to risks, our excessively-protective risk managers have, in their zeal, removed our capacity to manage risks ourselves. Precaution over information, safety over autonomy, dictation over accountability.”
To quote Mollie Hemingway, in the case of the coronavirus, Americans are “reacting like a bunch of hysterics“.