Tags
Alex Tabarrok, CDC, Chicago, Co-Morbidities, Covid-19, Emma Woodhouse, Essential Workers, Historical Inequities, Infection Fatality Rate, Long-Term Care, Megan McArdle, Super-Spreaders, Transmission, Vaccinations, Vaccine Allocation, Vaccine Passports
There are currently two vaccines in limited distribution across the U.S. from Pfizer and Moderna, but the number and variety of different vaccines will grow as we move through the winter. For now, the vaccine is in short supply, but that’s even more a matter of administering doses in a timely way as it is the quantity on hand. There are competing theories about how best to allocate the available doses, which is the subject of this post. I won’t debate the merits of refusing to take a vaccine except to say that I support anyone’s right to refuse it without coercion by public authorities. I also note that certain forms of discrimination on that basis are not necessarily unreasonable.
The vaccines in play all seem to be highly effective (> 90%, which is incredible by existing standards). There have been a few reports of side effects — certainly not in large numbers — but it remains to be seen whether the vaccines will have any long-term side effects. I’m optimistic, but I won’t dismiss the possibility.
Despite competing doctrines about how the available supplies of vaccine should be allocated, there is widespread acceptance that health care workers should go first. I have some reservations about this because, like Emma Woodhouse, I believe staff and residents at long-term care facilities should have at least equal priority. Yet they do not in the City of Chicago and probably in other areas. I have to wonder whether unionized health care workers there are the beneficiaries of political favoritism.
Beyond that question, we have the following competing priorities: 1) the vulnerable in care homes and other elderly individuals (75+, while younger individuals with co-morbidities come later); 2) “essential” workers of all ages (from police to grocery store clerks — decidedly arbitrary); and 3) basically the same as #2 with priority given to groups who have suffered historical inequities.
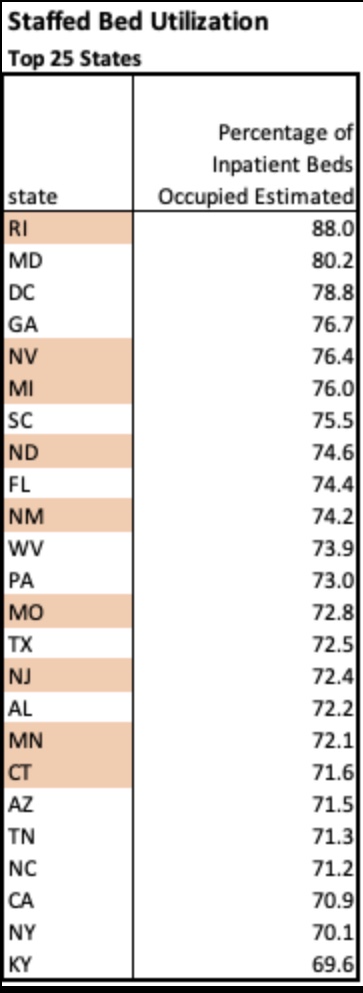
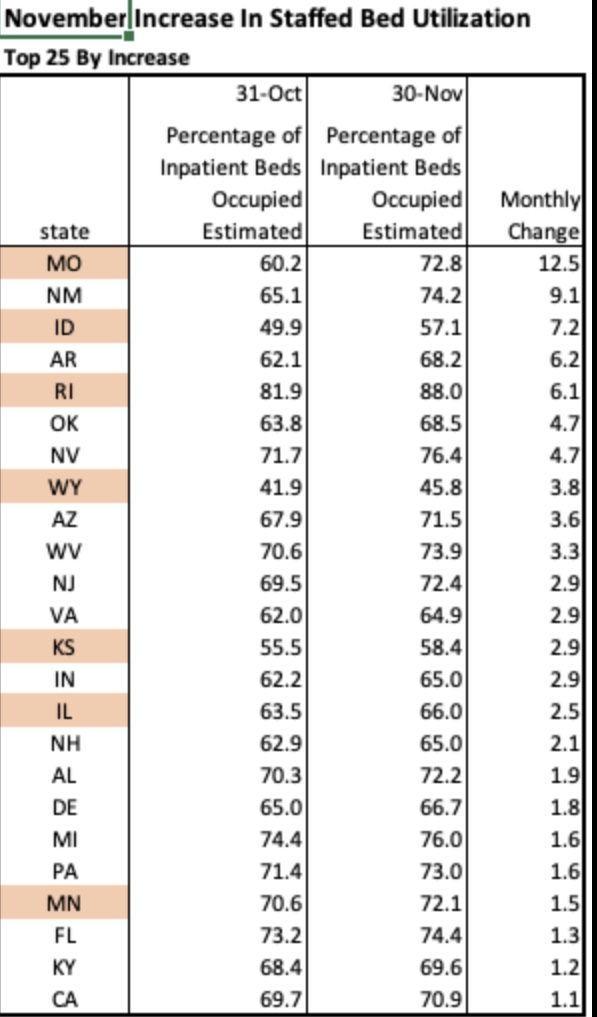
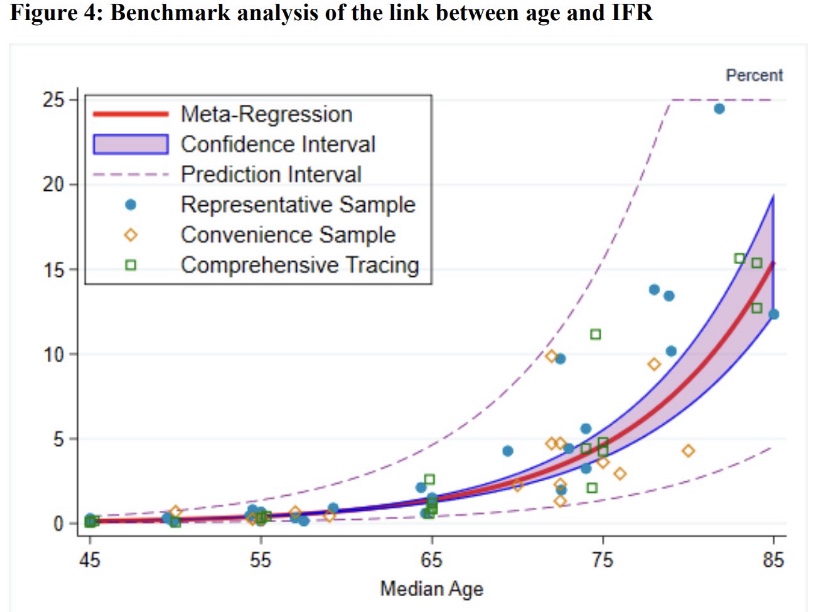
#1 is clearly the way to save the most lives, at least in the short-run. Over 40% of the deaths in the U.S. have been in elder-care settings, and COVID infection fatality rates mount exponentially with age:
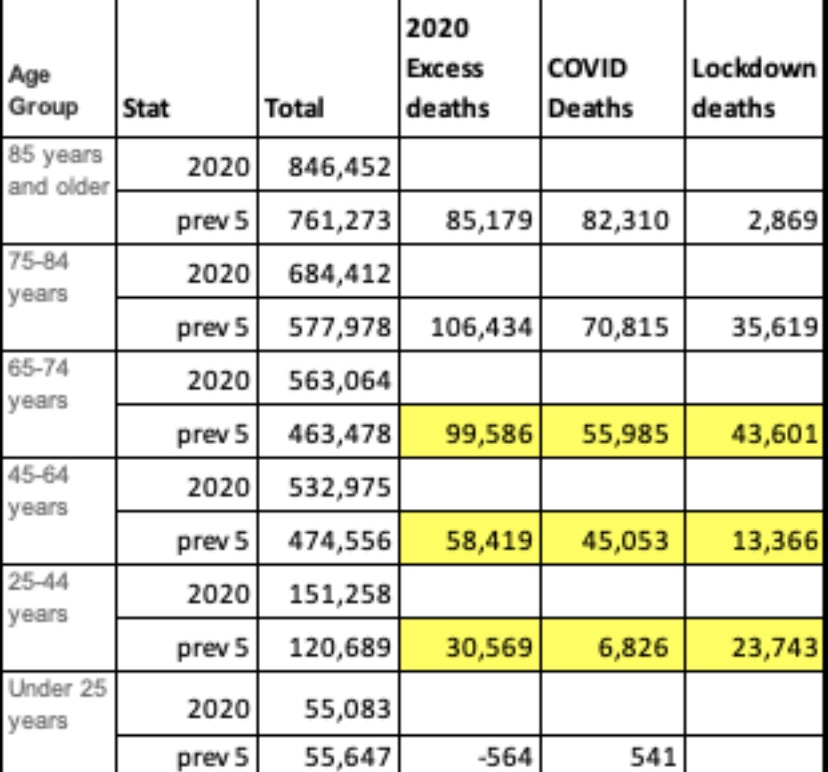
To derive the implications of #1 and #2, it’s more convenient to look at the share of deaths within each age cohort, since it incorporates the differences in infection rates and fatality rates across age groups (the number of “other” deaths is much larger than COVID deaths, of course, despite similar death shares):
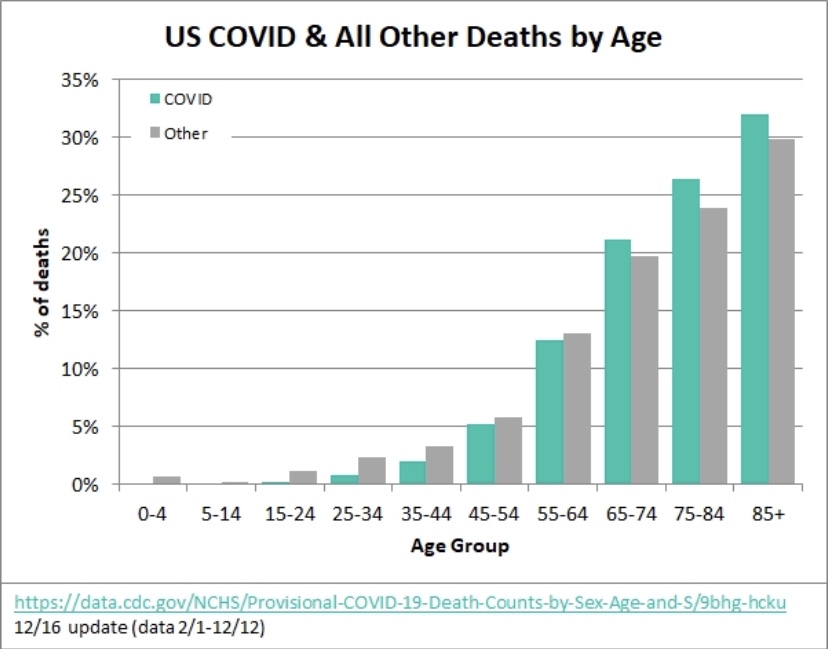
The 75+ age group has accounted for about 58% of all COVID deaths in the U.S., and ages 25 – 64 accounted for about 20% (an approximate age range for essential workers). This implies that nearly three times as many lives can be saved by prioritizing the elderly, at least if deaths among so-called essential workers mimic deaths in the 25 – 64 age cohorts. However, the gap would be smaller and perhaps reversed in terms of life-years saved.
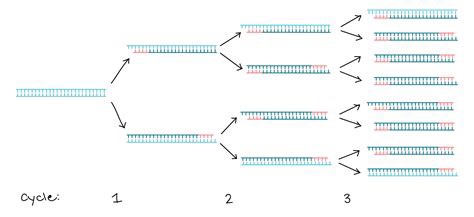
Furthermore, this is a short-run calculation. Over a longer time frame, if essential workers are responsible for more transmission across all ages than the elderly, then it might throw the advantage to prioritizing essential workers over the elderly, but it would take a number of transmission cycles for the differential to play out. Yes, essential workers are more likely to be “super-spreaders” than work-at-home, corporate employees, or even the unemployed, but identifying true super-spreaders would require considerable luck. Moreover, care homes generally house a substantial number of elderly individuals and staff in a confined environment, where spread is likely to be rampant. So the transmission argument for #2 over #1 is questionable.
The over-riding problem is that of available supply. Suppose enough vaccine is available for all elderly individuals within a particular time frame. That’s about 6.6% of the total U.S. population. The same supply would cover only about 13% of the younger age group identified above. Essential workers are a subset of that group, but the same supply would fall far short of vaccinating all of them; lives saved under #2 would then fall far short of the lives saved under #1. Quantities of the vaccine are likely to increase over the course of a few months, but limited supplies at the outset force us to focus the allocation decision on the short-term, making #1 the clear winner.
Now let’s talk about #3, minority populations, historical inequities, and the logic of allocating vaccine on that basis. Minority populations have suffered disproportionately from COVID, so this is really a matter of objective risk, not historical inequities… unless the idea is to treat vaccine allocations as a form of reparation. Don’t laugh — that might not be far from the intent, and it won’t count as a credit toward the next demand for “justice”.
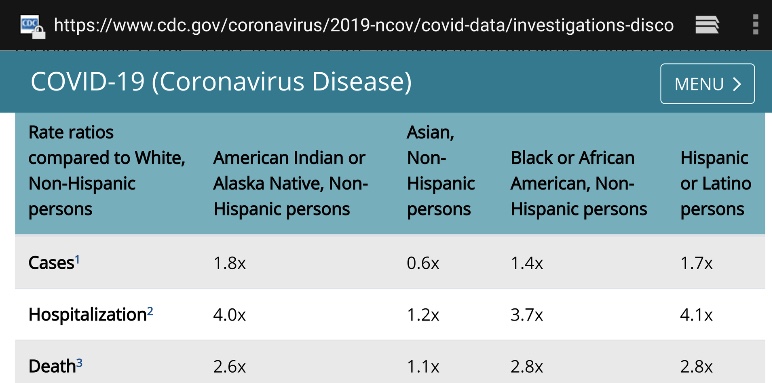
For the sake of argument, let’s assume that minorities have 3x the fatality rate of whites from COVID (a little high). Roughly 40% of the U.S. population is non-white or Hispanic. That’s more than six times the size of the full 75+ population. If all of the available doses were delivered to essential workers in that group, it would cover less than half of them and save perhaps 30% of minority COVID deaths over a few months. In contrast, minorities might account for up to two-thirds of the deaths among the elderly. Therefore, vaccinating all of the elderly would save 58% of elderly COVID deaths and about 39% of minority deaths overall!
The COVID mortality risk to the average white individual in the elderly population is far greater than that faced by the average minority individual in the working age population. Therefore, no part of #3 is sensible from a purely mathematical perspective. Race/ethnicity overlaps significantly with various co-morbidities and the number of co-morbidities with which individuals are afflicted. Further analysis might reveal whether there is more to be gained by prioritizing by co-morbidities rather than race/ethnicity.
Megan McArdle has an interesting column on the CDC’s vaccination guidelines issued in November, which emphasized equity, like #3 above. But the CDC walked back that decision in December. The initial November decision was merely the latest of the the agency’s fumbles on COVID policy. In her column, McArdle notes that the public has understood that the priority was to save lives since the very start of the pandemic. Ideally, if objective measures show that identifiable characteristics are associated with greater vulnerability, then those should be considered in prioritizing individuals who desire vaccinations. This includes age, co-morbidities, race/ethnicity, and elements of occupational risk. But lesser associations with risk should not take precedence over greater associations with risk unless an advantage can be demonstrated in terms of lives saved, historical inequities or otherwise.
The priorities for the early rounds of vaccinations may differ by state or jurisdiction, but they are all heavily influenced by the CDC’s guidelines. Some states pay lip service to equity considerations (if they simply said race/ethnicity, they’d be forced to operationalize it), while others might actually prioritize doses by race/ethnicity to some degree. Once the initial phase of vaccinations is complete, there are likely to be more granular prioritizations based on different co-morbidities, for example, as well as race/ethnicity. Thankfully, the most severe risk gradient, advanced age, will have been addressed by then.
One last point: the Pfizer and Moderna vaccines both require two doses. Alex Tabarrok points out that first doses appear to be highly effective on their own. In his opinion, while supplies are short, the second dose should be delayed until all groups at substantially elevated risk can be vaccinated…. doubling the supply of initial doses! The idea has merit, but it is unlikely to receive much consideration in the U.S. except to the extent that supply chain problems make it unavoidable, and they might.