Tags
Contagion, Coronavirus, Covid-19, Fat-Tailed Distribution, Heart Disease, Herd Immunity, John Cochrane, President Trump, Prophylaxis, Public Park Closures, Reproduction Rate, Restart Economy, Right Skew, Shelter In Place, Stay-at-Home, Suicide, Super-Spreaders, The Federalist, Transmission Rate

People talk about the transmission rate or reproduction rate (R0) of Covid-19 as if it’s a single number that applies to the entire population. John Cochrane emphasizes the huge implications of this misperception for how best to prevent the spread of the virus, and at lower cost, and for how best to “restart” the economy.
First, however, lets dispense with the absolutist position that there can be no compromise on virus mitigation in favor of economic activity. I am not opposed to the “lockdown” we are now living, but it will have significant and unnecessary costs if it goes on too long: the lost output is a huge blow not only to our current lifestyles but to our ability to grow in the future, or even to afford better health care in the future. Beyond that, the lockdown has immediate negative impacts of its own on public health: economic stress leads to all kinds of terrible health outcomes like heart disease and even suicide. About the latter, the President is absolutely correct: if you need research to prove it, see here, here, here, and here, all respected journals (the links all courtesy of The Federalist.) Economic stress and isolation is quite likely to promote poor dietary habits, lethargy, and possibly family dysfunction as well. Don’t pretend there aren’t real tradeoffs between the economy, virus interventions, and public health. The trick is to improve those tradeoffs. A balance can and must be struck, and depending on policy actions, the tradeoff can be made better or worse.
Back to the virus reproduction rate: the R0 values we see quoted are estimates of the average number of other people infected by each infected person. A value of three means that each person infected with the virus passes it on to three others, on average. If R0 is greater than one, an epidemic grows. If R0 is less than one, a contagion recedes. It becomes a “non-epidemic” if R0 remains less than one. It does not have to be zero (and probably cannot be zero).
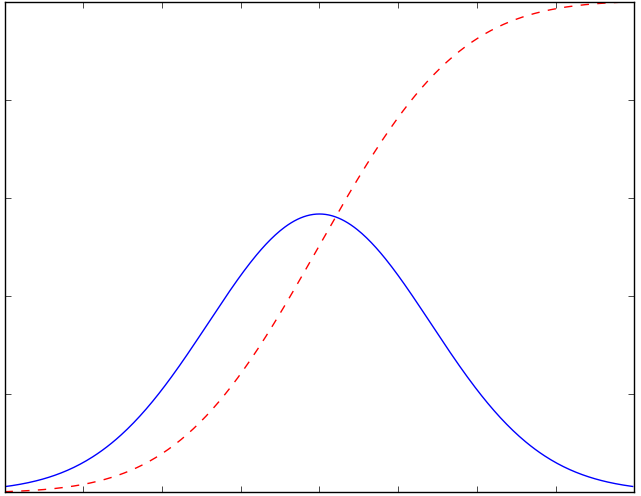
But not everyone is the same: my R0 is different from your R0 if only because we have different occupational exposure to others and different levels of social engagement. We also differ physiologically, which probably leads to differences in our “personal” R0 values. And an individual’s R0 will differ by time and place, depending on random circumstances like which way the wind is blowing. But here is where it gets interesting. Cochrane describes an extreme version of the skewed distribution shown at the top of this post:
“Suppose there are 100 people with a 0.5 reproduction rate, and 1 super-spreader with a 100 replication rate. The average reproduction rate is 1.5. Clearly, locking everyone down is wildly inefficient. It’s much more important to find the 1 super-spreader and lock him or her down, or change the business or behavior that’s causing the super-spreading.
This is exaggerated, but not far off the mark. I have not seen numbers on the distribution of reproduction rates across people, but it is a fair bet that it has an extremely fat tail. Most of us are washing our hands, social distancing, work in businesses that are shut down or are taking great steps to limit contact. And a few people and activities contribute to most of the spread.
This wide and fat-tailed dispersion is ignored in a lot of simulations I’ve seen. They take the average reproduction rate as the same for everyone. That’s a big mistake.
The danger: we waste a huge amount of time and money moving you and me from a 0.5 reproduction rate to an 0.4 reproduction rate. … The opportunity: focus on the super-spreaders, and the super-spreading activities, and you bring down the reproduction rate at much lower cost. “
There are many ways to reduce R0. Cochrane gets a little more specific about this and the policy implications of the skewed R0 distribution across individuals:
“All we need is to get the transmission rate under one. Activities with possible but very low transmission rates, and high economic benefits should go on. Don’t separate to ‘essential’ and ‘non-essential.’ Separate into ‘high likelihood of transmission’ and ‘low likelihood of transmission.’
Why are we not using masks everywhere? Sure, they’re not perfect. Sure, an old hankerchief might only cut the chance of transmission by half. We’re not all surgeons. Cutting by half is enough to stop the virus.
Conversely, why did they close the state parks? Really? Just how dangerous is it to drive the dog to a hiking trail and stay 6 feet away from other people? Parks, ski areas, golf courses, all sorts of businesses that surely can be run with a reproduction rate far less than one are just shut down. I met a realtor on our dog walk yesterday. They’re totally shut down. Just how hard is it to run a realty business with a 0.5 reproduction rate? One family in the house at a time, don’t touch anything, an hour between showings, stay 6 feet from the realtor… But instead the whole business is just shut down.”
The beginning of that last paragraph echoes a point I made in my last post about public park closures and the health benefits of getting outside generally.
Cochrane goes on to discuss several other policy options, including the potential benefits of simple kinds of testing and the overemphasis on false negatives and positives in policy discussions. Imperfect tests should not be discouraged by these concerns. If you’re worried about that, you shouldn’t use a thermometer either!
“Stay-at-home” or “shelter-in-place” orders will increasingly be tested by private parties if they remain in effect too long. That will be encouraged by the seemingly arbitrary distinctions some orders make between “essential” and “non-essential” activities. If workers or small businessmen judge themselves to be at low risk, they will take matters into their own hands to the extent they can. I believe that’s already happening where the specifics of “lockdown” orders have gone too far. Workers at the low end of the income spectrum are especially hard hit by these orders. One can hardly blame them for trying to earn what they can if they believe, and their customers believe, their activities and interactions are of low risk.
Ultimately, the entire distribution of R0s will slide to the left. That will occur even at low levels of “herd immunity” and anything that offers at least weak prophylaxis. Broadly speaking, the latter includes maintaining distance, refusing admittance to venues with a fever, avoiding handshakes, wearing masks, and potentially chloroquine, which is already in widespread use by physicians treating coronavirus patients. Ultimately, a vaccine will slide the distribution far to the left, but the economy need not be held hostage until that time. To paraphrase Cochrane, we can get the transmission rate below one and keep it there without stopping the world permanently. There are many options, and now is the time for business and government to start planning for that.