Tags
Alex Tabarrok, Drug Prices, Evergreen Patents, FDA, Food and Drug Administration, Generic Drug Prices, Import Quotas, Insulin Pricing, Michael Mandell, National Bureau of Economic Research, Out-of-Pocket Costs, Prescription Drug Escalator, Progressive Policy Institute, Utilization
Ask anyone on the street about prescription drug prices, or ask anyone in the press, and you’ll probably hear they are out of control. That contention is false. The conventional wisdom is typified by this exaggerated BS about insulin pricing … actually, you can find a vial of the kind I used for many years for about $25 without much difficulty.
Individual experience differs, of course. Yes, there are new drugs on the market that are exorbitant; there are older drugs still under patent that are pricey too. Those represent a fairly small part of the total market, however, and one on which policymakers should tread lightly if they hope to foster the development of new, life-saving drugs. Newer insulin varieties are not in that class, and those varieties don’t always incorporate meaningful improvements for patients.
Getting Old Is Hell
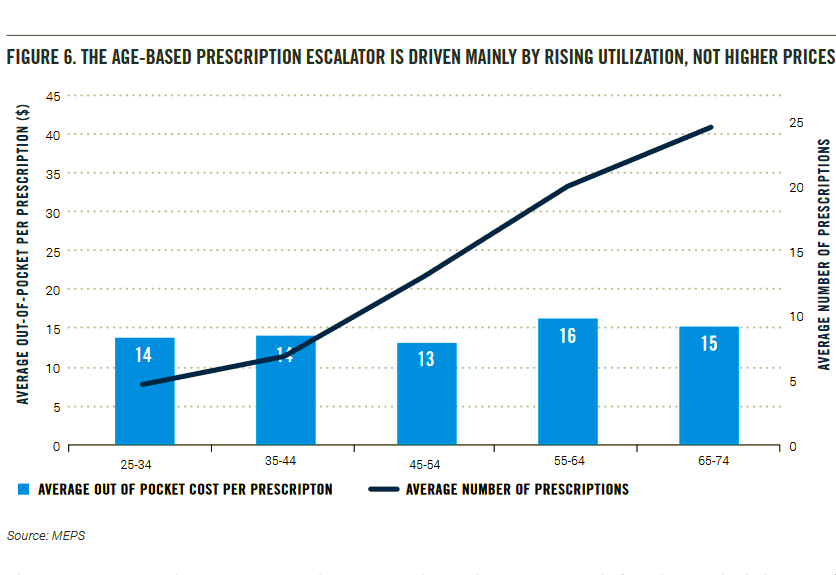
In fact, prescription drug prices have been declining for a number of years. The real problem is we’re always getting older! In a report from the Progressive Policy Institute, Michael Mandel describes what he calls the prescription drug escalator. Alex Tabarrok has a good summary of the article. The chart at the top of this post, from Mandel, shows that the number of drugs prescribed rises steadily with one’s age. The total bill rises along with age, which may create the perception that you’re paying higher prices. Unsurprisingly, more of each health-care dollar spent out-of-pocket (OOP) goes to prescribed medications as you age, and more goes to prescription drugs as health declines. As Mandell says, the increases experienced by individuals are a matter of utilization as opposed to pricing..
Generic Dominance
Tabarrok notes that generic drugs account for somewhere between 80-90% of all prescriptions, and generic costs have been falling for some time. He links to one of his earlier posts on generics and to this study by the National Bureau of Economic Research, which states:
“… direct-out-of-pocket CPI for generic prescription drugs decline[d] by about 50% between 2007 and 2016 …”
Average OOP prescription costs peaked in 2006, according to Mandel’s data. Tabarrok quotes Mandell:
“May 2019 research report from the Agency for Healthcare Research and Quality reported that average out-of-pocket spending for prescribed medications, among persons who obtained at least one prescribed medication, declined from $327 in 2009 to $238 by 2016, a decrease of 27 percent. Data from the Bureau of Labor Statistics Consumer Expenditure Survey shows that average household spending on prescription drugs fell by 11% between 2013 and 2018.
Moreover, OECD data shows that average out-of-pocket spending on prescribed medicines in the United States ($143 per capita in 2017) is actually lower than countries such as Canada ($144), Korea ($156), Norway ($178), and Switzerland ($215).”
The declines in OOP drug costs came despite a shift in health-care payment responsibilities from insurers to consumers in recent years — OOP costs would have declined much more had the shift not occurred, according to Mandel. As he says, consumers now have more “skin in the game”, and apparently they act on it.
Another basis of the misperception about escalating drug prices has to do with the way they are reported. Mandel says:
“List prices are the published prices that manufacturers charge to wholesalers. Net prices reflect the revenues that drug manufacturers receive, net of rebates and discounts to prescription benefit managers, insurance companies, and hospitals.
Studies of list prices invariably show very strong growth. For example the IQVIA Institute for Human Data Science found that the list price of the average brand rose from $364.92 to $657.08 since 2014, an 80% increase. Similarly, a widely cited recent study based on list prices found that from 2008–16, the costs of oral and injectable brand-name drugs increased annually by 9.2 percent and 15.1 percent, respectively. … By contrast, net prices and net pharma revenue have been growing much more slowly, once rebates and discounts are accounted for.”
The Pricey Segment
There are a variety of circumstances that bear on the pricing of individual drugs. Clearly, non-generic drugs are subject to more upward price pressure and give rise to anecdotes that feed misperceptions about the overall trajectory of drug prices. These are either new drugs or older ones sold under extended patents, which are sometimes granted for even minor changes in a drug’s chemical makeup.
Some new drugs are life-saving breakthroughs targeting rare diseases. The unfortunate truth is that drug development is a very costly enterprise, often stretching well over a decade in the U.S. under the FDA’s approval process. Moreover, U.S. consumers actually subsidize the cost of drugs for European consumers, where drugs are typically subject to price ceilings or are directly negotiated by government. By the time drugs go to market, development is treated as a fixed cost; even the low prices in Europe cover the marginal cost of production, so pharmaceutical manufacturers don’t mind selling there as long as their development overhead is paid by someone. That’s the rub.
Drug development costs are heavily influenced by public policy, often to the detriment of consumers. The FDA’s drug approval process is in dire need of reform, and patent extensions should be severely curtailed. As an advocate of free trade, I also favor a lifting of restrictions on imports of drugs to the U.S.
Conclusion
You’re likely to see more physicians as you age, they’re likely to prescribe more drugs, and you’re likely to pay more for prescriptions OOP. That’s the escalator in action. You can minimize the slope of your personal prescription escalator by taking good care of yourself and using generics when possible, but the slope is often beyond a person’s control. Nevertheless, over the past 13 years in the U.S., most of those experiencing higher OOP costs have this escalator, i.e., aging, to thank… it’s drug utilization, not pricing.
A relatively small but important share of the market has experienced price escalation. Newer, highly specialized drugs can carry high price tags. Patents give drug manufacturers considerably more pricing power, and drug companies have sought to maintain “evergreen” patents by manipulating their formulations. U.S. import quotas and restrictive pricing abroad have left consumers in the U.S. holding the bag for a large share of drug development costs. These shortcomings can be addressed via streamlined drug approval, patent reform, and lifting import restrictions.
A critical policy prescription is to liberate market forces and foster competition in the pharmaceuticals industry. Price controls in the U.S. would eliminate all incentives for new breakthroughs, leading progress in many areas of treatment to a stand-still. Price controls merely substitute the arbitrary decisions of politicians and bureaucrats for the market’s ability to balance dynamic consumer needs, medical expertise, and the costs faced by sellers.