
Tags
Aerosols, BMI-Years, Body Mass Index, Body Positivity, Covid-19, David A. Edwards, Exhaled Particles, Mucus, Obestity, SARS Virus, Super-Spreading, Vaccination, Vaccine Passport, Weight Loss
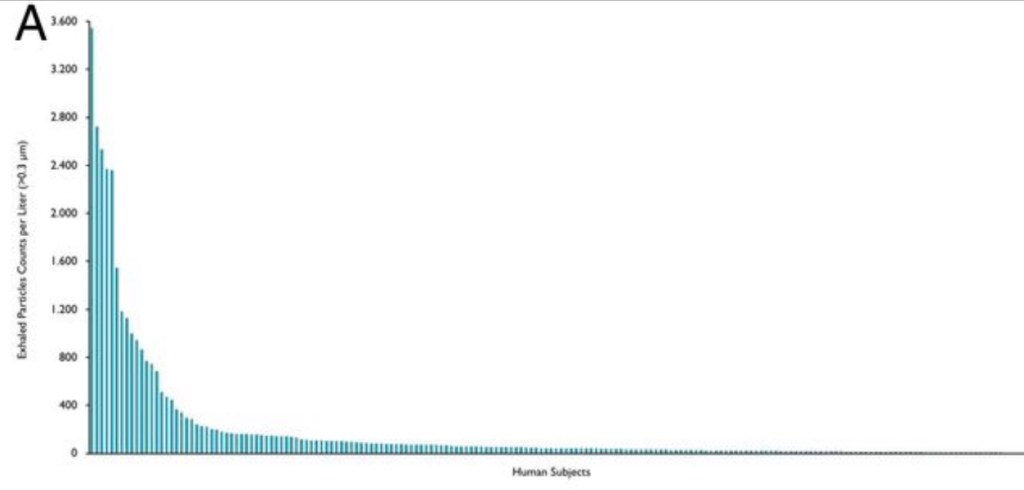
Super-spreading events are gatherings at which one or more attendees are already harboring an infection and manage to transmit it to a number of others. These people, in turn, spread it to their close contacts, possibly at the same event. Super-spreading has dominated the transmission of COVID-19. These transmissions have almost always taken place indoors in spaces with limited ventilation, and they have usually involved close or prolonged contact. In addition, super-spreading originates with a small subset of infected individuals. That’s essentially what the chart above shows. It ranks individual subjects by their exhaled quantity of aerosolized particles per liter of air.
For more than a year, we’ve also known that obesity and age are associated with more severe COVID infections. Now, it’s startling to learn that obese and/or older, infected individuals are more prone to transmitting virus: this study found that a high body mass index (BMI) is associated with significantly greater quantities of exhaled aerosol, and that age has a similarly strong association. So called BMI-years, or age x BMI, has an extremely powerful association with the exhalation of aerosol-borne particles. The authors, David A. Edwards, et al, believe this is a consequence of the properties of mucus produced by different individuals in response to infections and how their lungs and airways handle it. The authors say:
“Our findings indicate that the capacity of airway lining mucus to resist breakup on breathing varies significantly between individuals, with a trend to increasing with the advance of COVID-19 infection and body mass index multiplied by age (i.e., BMI-years). Understanding the source and variance of respiratory droplet generation, and controlling it via the stabilization of airway lining mucus surfaces, may lead to effective approaches to reducing COVID-19 infection and transmission. … ”
“Surfactant and mucin compositional and structural changes, driven, in part, by physiological alterations of the human condition—including diet (10), aging (11), and COVID-19 infection itself (12)—may therefore be anticipated to alter droplet generation and droplet size (7) during acts of breathing.”
So there is substantial variation in the exhalation of aerosol-borne particles across individuals. In the study, less than 20% of healthy subjects produced more than 156 particles per liter of air, accounting for 80% of the exhaled particles. This defined their so-called “super-spreader” cohort. The association of BMI-years and exhaled particles was less pronounced but still positive within the “low-spreader” cohort.
Edwards, et al speculate that these fine droplets might help explain the greater severity of COVID infections among the elderly and obese. Not only does the breakup of mucus into tiny droplets cause these individuals to exhale aerosols more profusely, it probably also leads to deep penetration into their lung tissue.
This knowledge might be broadly applicable to infectious diseases, and SARS viruses in particular. The elderly know they are vulnerable. It’s not clear that the obese have viewed themselves as vulnerable, but they should, even in the age of “body positivity“. And not only are they vulnerable: they appear to pose an elevated hazard to others. I came across a couple of sardonic comments that got right to the apparent elephant in the room: “Instead of a mask mandate, how about a push-up mandate?”; and “Instead of a vaccine passport, how about a BMI passport?”
The debate about how to care for the most vulnerable is ongoing, but the mere mention of regularities like those identified by the study might lead to proposals for coercive policies. But first, a few practical points to bear in mind: 1) while the study identifies a major risk factor for transmission, it must be replicated by others, and there must be research into the underlying reasons for the phenomenon; 2) while the obese and seniors may be more likely to super-spread, not all of them are super-spreaders; and 3) as a matter of policy, how would “super-spreaders” be defined? What would be the cutoff BMIs at various ages? No matter what was decided, restrictive policies predicated on mere statistical associations would involve gross injustices to a large number of individuals.
With the degree of acquired immunity already in the population and fairly widespread voluntary vaccination (since alarmists have scared the bejeezus out of everyone), the whole issue might seem moot. It’s not, however, because COVID-19 is likely to become endemic, the immunities of some individuals might erode more quickly than expected, new and more dangerous variants might arise, and new SARS viruses are likely to emerge with time.
In a pandemic, however, and even without knowing who is infected, it is ethically barbaric to probabilistically isolate classes of individuals, whether based on age, BMI, or anything other than contagious status. The social cost is simply unacceptable. Instead, public health authorities should provide information to those at high risk, facilitate vaccination for those who desire it, and promote rapid, at-home tests. This is essentially a deregulatory agenda relative to the mindless lockdown approaches favored by so many public health experts.
Everyone must balance their own personal risks and rewards. Based on the study of exhaled particles discussed above, some might shun the obese and seniors until the threat has passed. Some of the obese and elderly might shun each other. That might be another regrettable dimension of the costs of a pandemic. On the other hand, perhaps more of us will respond to the unquestionably positive incentives for weight loss, of which we’re almost all aware.

Pingback: I argue with Bill Maher (about COVID issues) – Life of an old goat
Pingback: CDC Makes a Bum Lead Steer: Alternate Reality vs. The Herd | Sacred Cow Chips