
Tags
Acquired Immunity, Aerosols, Alpha Variant, Antibodies, Base Rate Bias, Breakthrough Infections, Covid-19, Delta Variant, Immunity, Issues & Insights, Kappa Variant, Kelly Brown, Lambda Variant, Larry Brilliant, Mayo Clinic, Our World In Data, PCR Tests, Phil Kerpen, T-Cell Immunity, Vaccinations, WHO

Listen very carefully: immunity does NOT mean you won’t get COVID, though an infection is less likely. Immunity simply means your immune system will be capable of dealing with an infection successfully. This is true whether the immunity is a product of vaccination or a prior infection. Immunity means you are unlikely to have worse than mild symptoms, and you are very unlikely to be hospitalized. (My disclaimer: I am opposed to vaccine mandates, but vaccination is a good idea if you’ve never been infected.)
I emphasize this because the recent growth in case numbers has prompted all sorts of nonsensical reactions. People say, “See? The vaccines don’t work!” That is a brazenly stupid response to the facts. Even more dimwitted are claims that the vaccines are killing everyone! Yes, there are usually side effects, and the jabs carry a risk of serious complications, but it is minuscule.
Vaccine Efficacy
Right out of the gate, we must recognize that our PCR testing protocol is far too sensitive to viral remnants, so the current surge in cases is probably exaggerated by false positives, as was true last year. Second, if a large share of the population is vaccinated, then vaccinated individuals will almost certainly account for a large share of infected individuals even if they have a lower likelihood of being infected. It’s simple math, as this explanation of base rate bias shows. In fact, according to the article at the link:
“… vaccination confers an eightfold reduction in the risk of getting infected in the first place; a 25-fold reduction in risk of getting hospitalized; and a 25-fold reduction in the risk for death.”
The upshot is that if you are vaccinated, or if you have acquired immunity from previous exposure, or if you have pre-existing immunity from contact with an earlier COVID strain, you can still “catch” the virus AND you can still spread it. Both are less likely, and you don’t have as much to worry about for your own health as those having no immunity.
As for overall vaccine efficacy in preventing death, here are numbers from the UK, courtesy of Phil Kerpen:
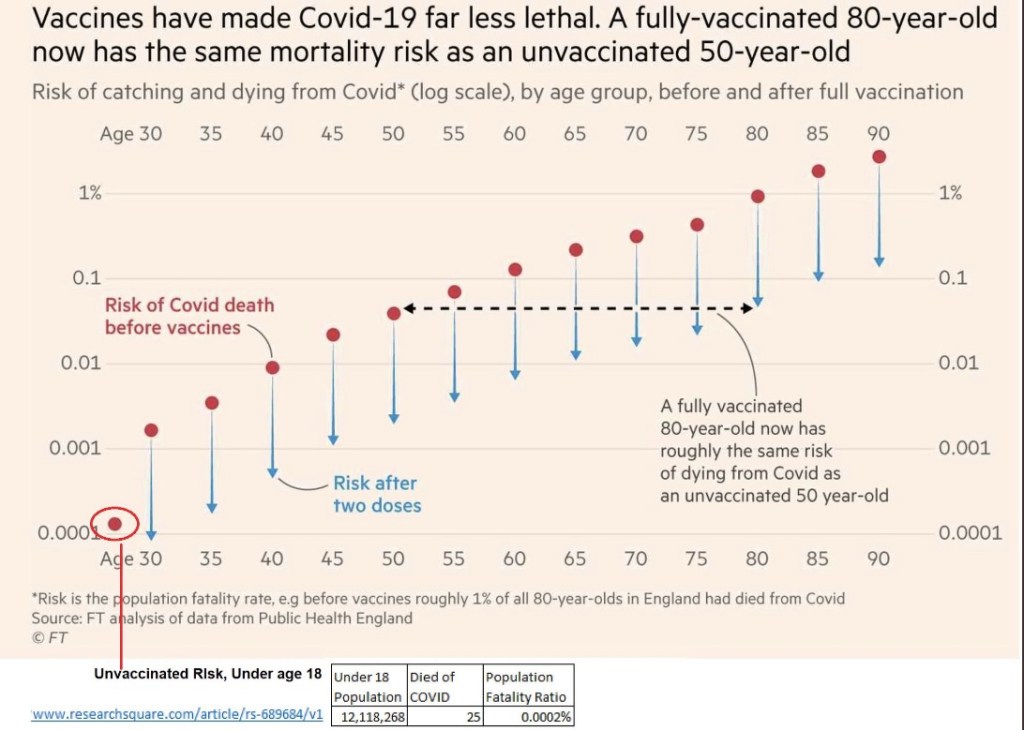
The vertical axis is a log scale, so each successive gridline is a fatality rate 100x as large as the one below it. Obviously, as the chart title asserts, the “vaccines have made COVID-19 far less lethal.” Also, at the bottom, see the information on fatality among children under age 18: it is almost zero! This reveals the absurdity of claims that children must be masked for schools to reopen! In any case, masks offer little protection to anyone against a virus that spreads via fine aerosols. Nevertheless, many school officials are pushing unnecessary but politically expedient masking policies
Delta
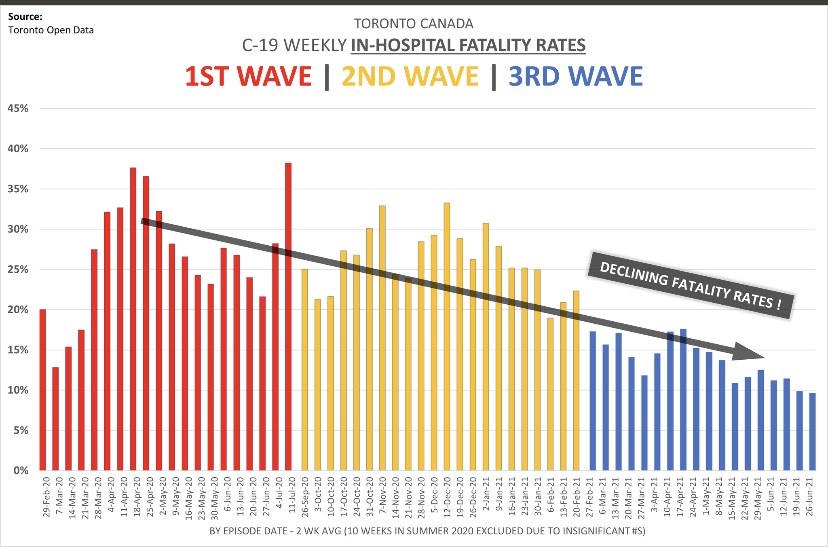
Ah, but we have the so-called Delta variant, which is now dominant and said to be far more transmissible than earlier variants. Yet the Delta variant is not as dangerous as earlier strains, as this UK report demonstrates. Delta had a case fatality rate among unvaccinated individuals that was at least 40% less than the so-called Alpha variant. This is a typical pattern of virus mutation: the virus becomes less dangerous because it wants to survive, and it can only survive in the long run by NOT killing its hosts! The decline in lethality is roughly demonstrated by Kelly Brown with data on in-hospital fatality rates from Toronto, Canada:
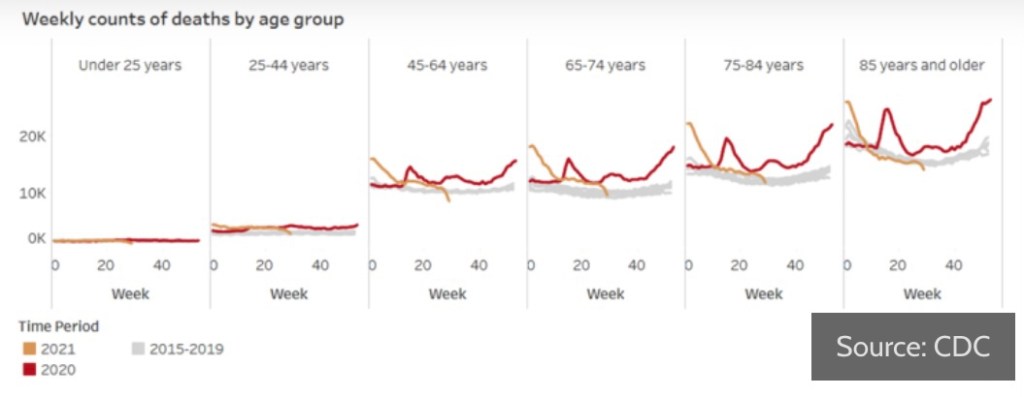
The case numbers in the U.S. have been climbing over the past few weeks, but as epidemiologist Larry Brilliant of WHO said recently, Delta spreads so fast it essentially “runs out of candidates.” In other words, the current surge is likely to end quickly. This article in Issues & Insights shows the more benign nature of recent infections. I think a few of their charts contain biases, but the one below on all-cause mortality by age group is convincing:
The next chart from Our World In Data shows the infection fatality rate continuing its decline in the U.S. The great majority of recent infections have been of the Delta variant, which also was much less virulent in the UK than earlier variants.

Furthermore, it turns out that the vaccines are roughly as effective against Delta and other new variants as against earlier strains. And the newest “scary” variants, Kappa and Lambda, do not appear to be making strong inroads in the U.S.
Fading Efficacy?
There have been questions about whether the effectiveness of the vaccines is waning, which is behind much of the hand-wringing about booster shots. For example, Israeli health officials are insisting that the effectiveness of vaccines is “fading”, though I’ll be surprised if there isn’t some sort of confounding influence on the data they’ve cited, such as age and co-morbidities.
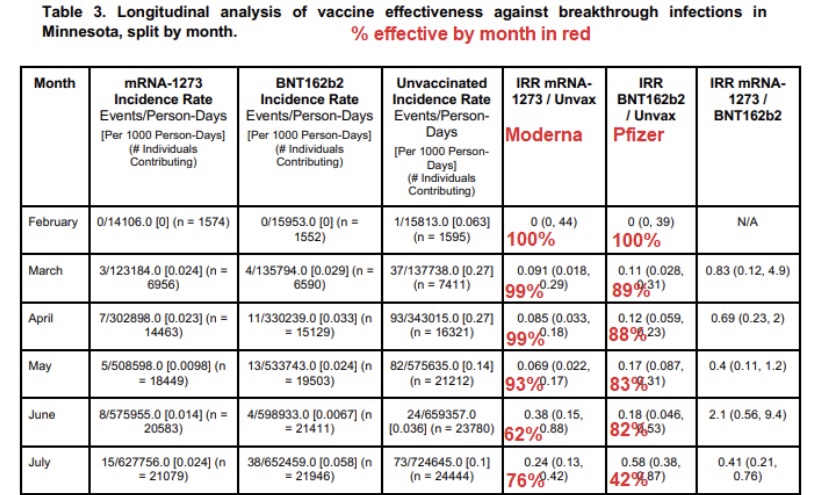
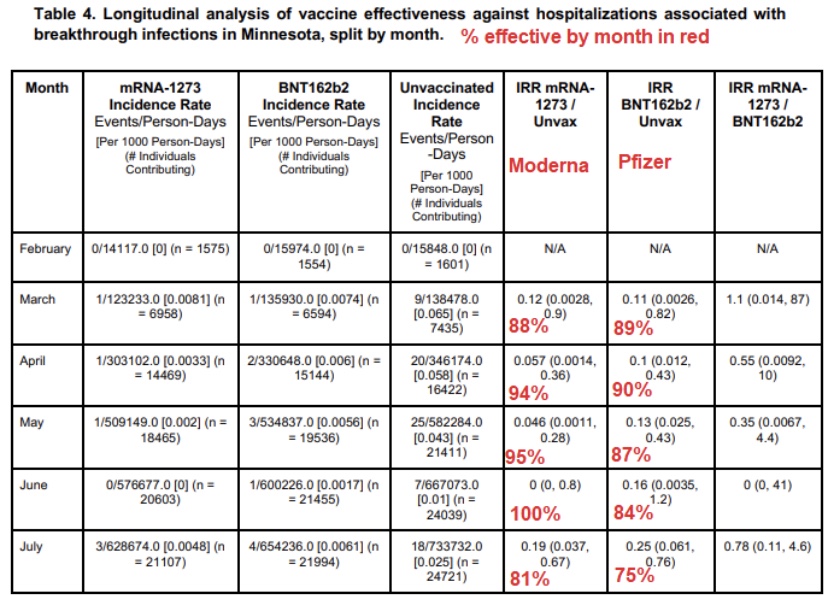
Here is a new Mayo Clinic study of so-called “breakthrough” cases in the vaccinated population in Minnesota. It essentially shows that the rate of case diagnosis among the vaccinated rose between February and July of this year (first table below, courtesy of Phil Kerpen). However, the vaccines appear only marginally less effective against hospitalization than in March (second table below).
The bulk of the vaccinated population in the U.S. received their jabs three to six months ago, and according to this report, evidence of antibodies remains strong after seven months. In addition, T-cell immunity may continue for years, as it does for those having acquired immunity from an earlier infection.
Breakthroughs
It’s common to hear misleading reports of high numbers of “breakthrough” cases. Not only will these cases be less menacing, but the reports often exaggerate their prevalence by taking the numbers out of context. Relative to the size of the vaccinated population, breakthrough cases are about where we’d expect based on the original estimates of vaccine efficacy. This report on Massachusetts breakthrough hospitalizations and deaths confirms that the most vulnerable among the vaxed population are the same as those most vulnerable in the unvaxed population: elderly individuals with comorbidities. But even that subset is at lower risk post-vaccination. It just so happens that the elderly are more likely to have been vaccinated in the first place, which implies that the vaccinated should be over-represented in the case population.
Conclusion
The COVID-19 vaccines do what they are supposed to do: reduce the dangers associated with infection. The vaccines remain very effective in reducing the severity of infection. However, they cannot and were not engineered to prevent infection. They also pose risks, but individuals should be able to rationally assess the tradeoffs without coercion. Poor messaging from public health authorities and the crazy distortions promoted in some circles does nothing to promote public health. Furthermore, there is every reason to believe that the current case surge in Delta infections will be short-lived and have less deadly consequences than earlier variants.

Pingback: Herd Immunity To Public Health Bullshitters and To COVID | Sacred Cow Chips
Pingback: Vax Results, Biden Boosters, Delta, and the Mask Charade | Sacred Cow Chips
Pingback: Vax Results, Biden Boosters, Delta, and the Mask Charade | Sacred Cow Chips
Pingback: Vax Results, Biden Boosters, Delta, and the Mask Charade – American Reveille
Pingback: Do Public Health Officials Believe Their Own Lies? Herd Immunity and Covid-19 Reporting – American Reveille