Tags
Adam Kucharski, Andy Slovitt, Anthony Fauci, CDC, Degrees of Separation, Herd Immunity, Herd Immunity Threshold, Joe Biden, Jordan Schachtel, Nathan D. Grawe, Obesity, Phil Kerpen, Pre-existing Immunity, Precautionary Principle, Reproduction Rate, Seroprevalence, Sub-Herds, Super-Spreader Events, Vaccinations, Vitamin D, Zero COVID
Jordan Schachtel enjoyed some schadenfreude last week when he tweeted:
“I am thoroughly enjoying the White House declaring COVID over and seeing the confused cultists having a nervous breakdown and demanding the continuation of COVID Mania.”
It’s quite an exaggeration to say the Biden Administration is “declaring COVID over”, however. They’re backpedaling, and while last week’s CDC announcement on masking is somewhat welcome, it reveals more idiotic thinking about almost everything COVID: the grotesquely excessive application of the precautionary principle (typical of the regulatory mindset) and the mentality of “zero COVID”. And just listen to Joe Biden’s tyrannical bluster following the CDC announcement:
“The rule is now simple: get vaccinated or wear a mask until you do.
The choice is yours.”
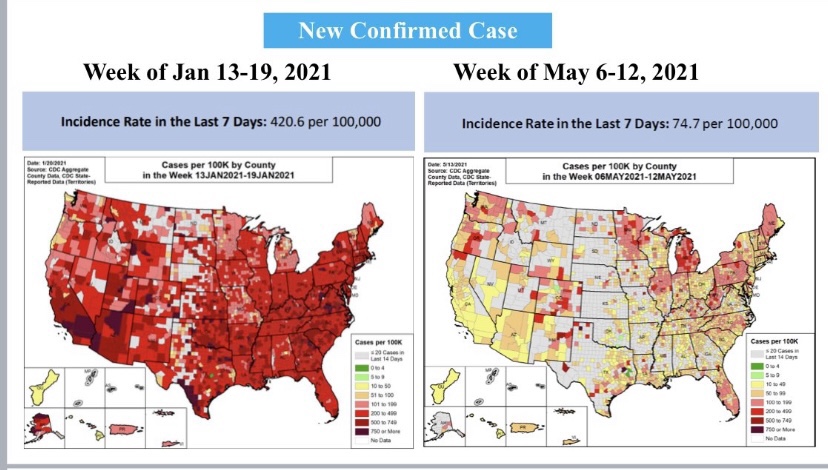
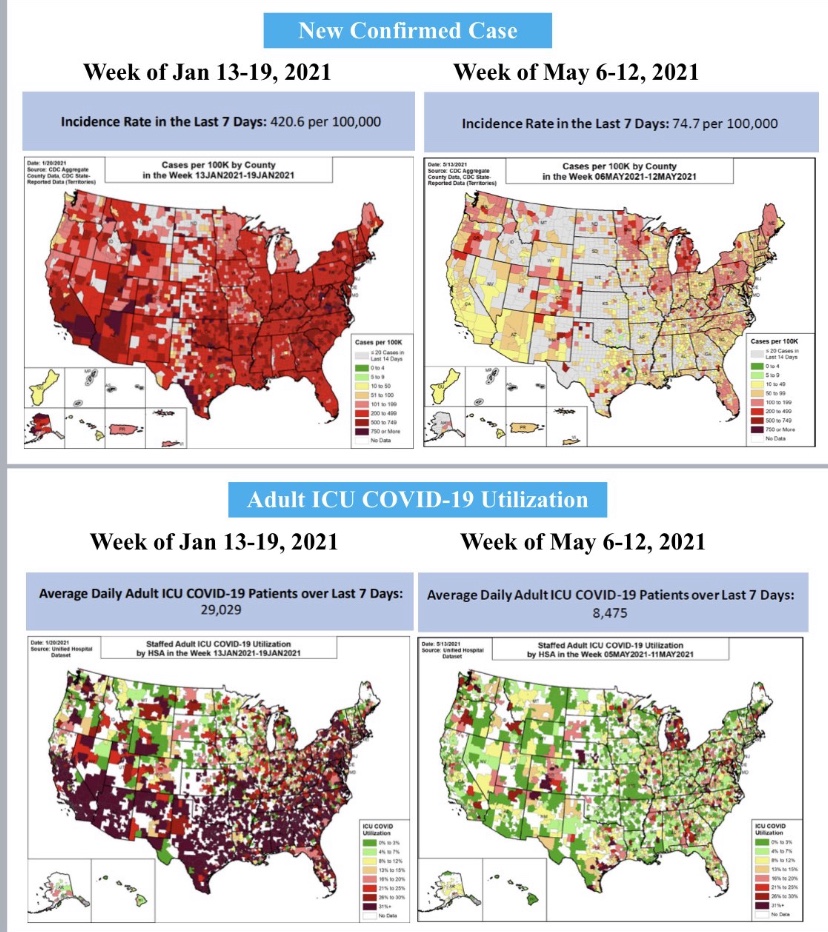
Is anyone really listening to this buffoon?Unfortunately, yes. But there’s no federal “rule”, unless your on federal property; it constitutes “guidance” everywhere else. I’m thankful our federalist system still receives a modicum of respect in the whole matter, and some states have chosen their own approaches (“Hooray for Florida”). Meanwhile, the state of the pandemic looks like this, courtesy of Andy Slavitt:
False Assertions
The CDC still operates under the misapprehension that kids need to wear masks, despite mountains of evidence showing children are at negligible risk and tend not to be spreaders. Here’s some evidence shared by Phil Kerpen on the risk to children:
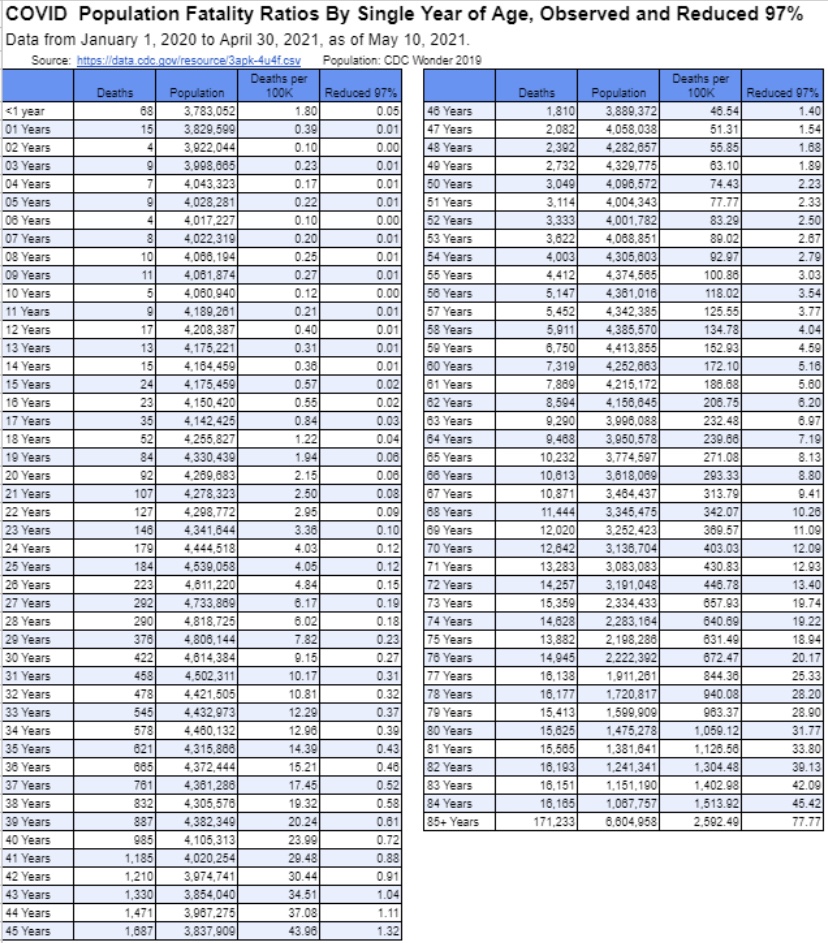
The chart shows the fatality risk by age (deaths per 100,000), and then under the assumption of a 97% reduction in that risk due to vaccination, which is quite conservative. Given that kind of improvement, an unvaccinated 9 year-old child has about the same risk as a fully vaccinated 30 year-old!
The CDC still believes the unvaccinated must wear masks outdoors, but unless you’re packed in a tight crowd, catching the virus outdoors has about the same odds as a piano falling on your head. And the CDC insists that two shots of mRNA vaccine (Pfizer or Moderna) are necessary before going maskless, but only one shot of the Johnson and Johnson vaccine, even though J&J’s is less effective than a single mRNA jab!
Other details in the CDC announcement are worthy of ridicule, but for me the most aggravating are the agency’s implicit position that herd immunity can only be achieved through vaccination, and its “guidance” that the unvaccinated should be dealt with coercively, even if they have naturally-acquired immunity from an infection!
Tallying Immunity
Vaccination is only one of several routes to herd immunity, as I’ve noted in the past. For starters, consider that a significant share of the population has a degree of pre-existing immunity brought on by previous exposure to coronaviruses, including the common cold. That doesn’t mean they won’t catch the virus, but it does mean they’re unlikely to suffer severe symptoms or transmit a high viral load to anyone else. Others, while not strictly immune, are nevertheless unlikely to be sickened due to protections afforded by healthy vitamin D levels or because they are not obese. Children, of course, tend to be fairly impervious. Anyone who’s had a bout with the virus and survived is likely to have gained strong and long-lasting immunity, even if they were asymptomatic. And finally, there are those who’ve been vaccinated. All of these groups have little or no susceptibility to the virus for some time to come.
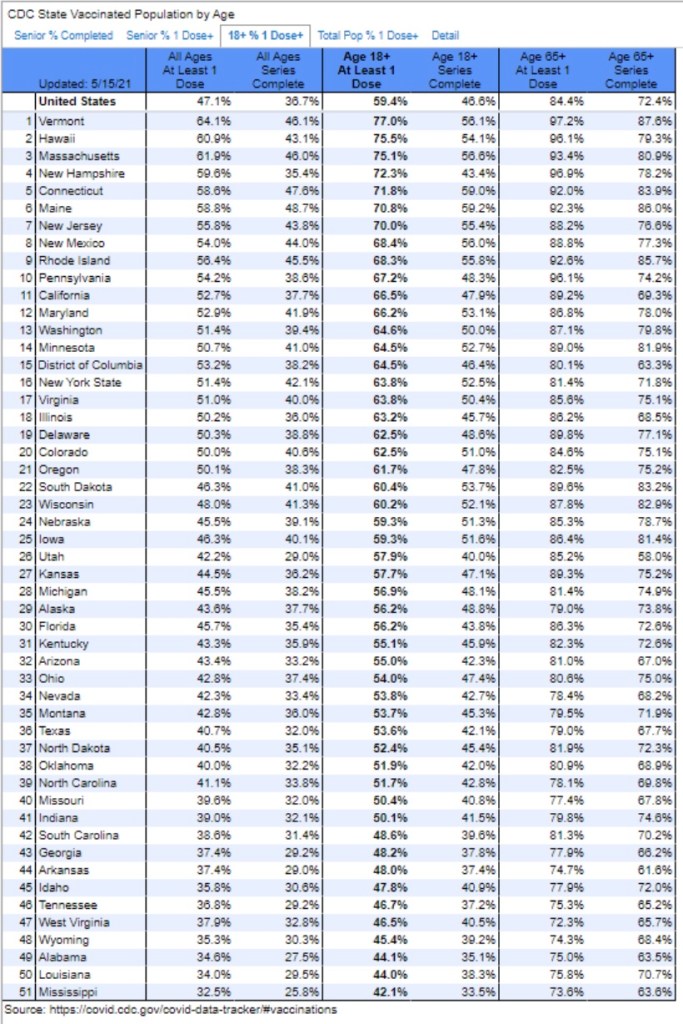
It’s not necessary to vaccinate everyone to achieve herd immunity, nor is it necessary to reach something like an 85% vax rate, as the fumbling Dr. Fauci has claimed. Today, almost 47% of the U.S. population has received at least one dose, or about 155 million adults. Here’s Kerpen’s vax update for May 14.
Another 33 million people have had positive diagnoses and survived, and estimates of seroprevalence would add perhaps another 30 million survivors. Some of those individuals have been vaccinated unnecessarily, however, and to avoid double counting, let’s say a total of 50 million people have survived the virus. Some 35 million children in the U.S. are under age 12. Therefore, even if we ignore pre-existing immunity, there are probably about 240 million effectively immune individuals without counting the remaining non-susceptibles. At the low end, based on a population of 330 million, U.S. immunity is now greater than 70%, and probably closer to 80%. That is more than sufficient for herd immunity, as traditionally understood.
The Herd Immunity Threshold
Here and in the following section I take a slightly deeper dive into herd immunity concepts.
Herd immunity was one of my favorite topics last year. I’m still drawn to it because it’s so misunderstood, even by public health officials with pretensions of expertise in the matter. My claim, about which I’m not alone, is that it’s unnecessary for a large majority of the population to be infected (or vaccinated) to limit the spread of a virus. That’s primarily because there is great variety in individuals’ degree of susceptibility, social connections, aerosol production, and viral load if exposed: call it heterogeneity or diversity if you like. Variation across individuals naturally limits a contagion relative to a homogeneous population.
Less than 1% of those who caught the virus died, while the others recovered and acquired immunity. The remaining subset of individuals most vulnerable to severe illness was thus reduced over time via acquired immunity or death. This is the natural dynamic that causes contagions to slow and ultimately peter out. In technical jargon, the virus reproduction rate “R” falls below a value of one. The point at which that happens is called the “herd immunity threshold” (HIT).
A population with lots of variation in susceptibility will have a lower HIT. Some have estimated a HIT in the U.S. as low as 15% -25%. Ultimately, total exposure will go much higher than the HIT, perhaps well more than doubling exposure, but the contagion recedes once the HIT is reached. So again, it’s unnecessary for anywhere near the full population to be immune to achieve herd immunity.
One wrinkle is that CIVID is now likely to have become endemic. Increased numbers of cases will re-emerge seasonally in still-susceptible individuals. That doesn’t contradict the discussion above regarding the HIT rate: subsequent waves will be quite mild by comparison with the past 14 months. But if the effectiveness of vaccines or acquired immunity wanes over time, or as healthy people age and become unhealthy, re-emergence becomes a greater risk.
Sub-Herd Immunity
A further qualification relates to so-called sub-herds. People are clustered by geographical, social, and cultural circles, so we should think of society not as a singular “herd”, but as a collection of sub-herds having limited cross-connectivity. The following charts are representations of different kinds of human networks, from Nathan D. Grawe’s review of “The Rules of Contagion, by Adam Kucharski:
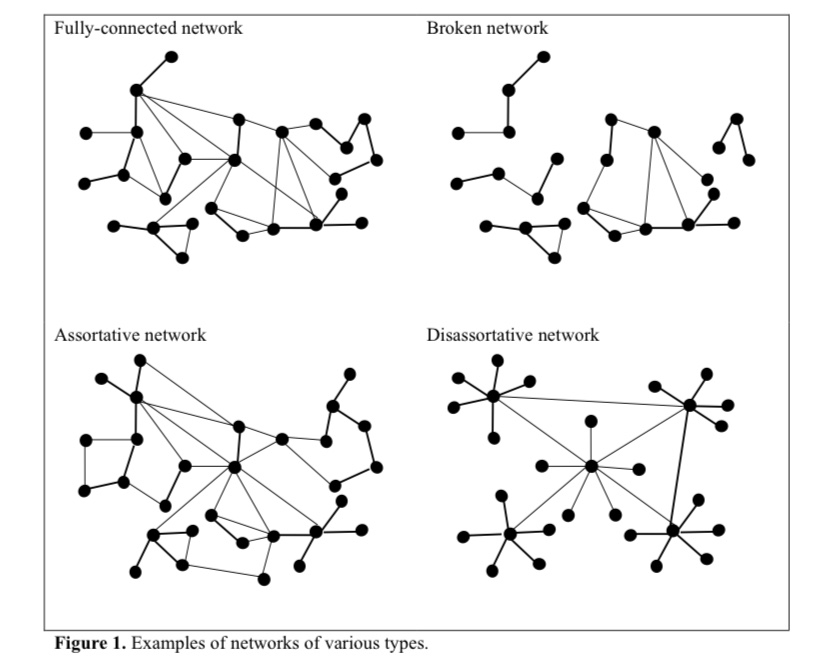
Sub-herd members tend to have more degrees of separation from individuals in other sub-herds than within their own sub-herd. The most extreme example is the “broken network” (where contagions could not spread across sub-herds), but there are identifiable sub-herds in all of the examples shown above. Less average connectedness across sub-herds implies barriers to transmission and more isolated sub-herd contagions.
We’ve seen isolated spikes in cases in different geographies, and there have been spikes within geographies among sub-herds of individuals sharing commonalities such as race, religious affiliation, industry affiliation, school, or other cultural affiliation. Furthermore, transmission of COVID has been dominated by “super-spreader” events, which tend to occur within sub-herds. In fact, sub-herds are likely to be more homogeneous than the whole of society, and that means their HIT will be higher than we might naively calculate based on higher levels of aggregation.
We have seen local, state, or regional contagions peak and turn down when estimates of total incidence of infections reach the range of 15 – 25%. That appears to have been enough to reach the HIT in those geographically isolated cases. However, if those geographical contagions were also concentrated within social sub-herds, those sub-herds might have experienced much higher than 25% incidence by the time new infections peaked. Again, the HIT for sub-herds is likely to be greater than the aggregate population estimates implied, The upshot is that some sub-herds might have achieved herd immunity last year but others did not, which explains the spikes in new geographic areas and even the recurrence of spikes within geographic areas.
Conclusion
It’s unnecessary for 100% of the population to be vaccinated or to have pre-existing immunity. Likewise, herd immunity does not imply that no one catches the virus or that no one dies from the virus. There will be seasonal waves, though muted by the large immune share of the population. This is not something that government should try to stanch, as that would require the kind of coercion and scare tactics we’ve already seen overplayed during the pandemic. People face risks in almost everything they do, and they usually feel competent to evaluate those risks themselves. That is, until a large segment of the population allows themselves to be infantalized by public health authorities.