Tags
Antonin Scalia, CDC, Department of Education, Executive Action, Federal Reserve, HEROES Act, Higher Education Act, Inflation Reduction Act, Jack V. Hoover, Joe Biden, Legal Standing, Lujan v. Defenders of Wildlife, Pandemic, Paycheck Protection Program, regressivity, Remain in Mexico, Standing Dead Zone, Student Loan Forgiveness, Supreme Court, Virginia Law Review

I hate to contribute to the deluge of ink spilled over Joe Biden’s latest executive action, which forgives massive amounts of federal student loan debt, but there’s an angle that hasn’t received adequate treatment. Of course, Biden’s action is an abridgment of taxpayer rights, a violation of the separation of powers, and an affront to borrowers who already paid off their student loans, but it will be nearly impossible for any challenger(s) to show that they have standing in court. Writing in the Virginia Law Review earlier this year, Jack V. Hoover says this kind of action lies within what he calls a “standing dead zone” created by the courts.
I’ll start with a few preliminaries. Note that student loan forgiveness was NOT legislated, unlike the Paycheck Protection Program, which the Administration keeps referencing in defense of the action. And I’d be remiss if I failed to mention that Biden’s action looks like a pathetic attempt to salvage votes ahead of what some democrats fear could be a disastrous midterm election. In addition, the action is regressive, with benefits weighted heavily toward high-income debtors with graduate degrees. The cost (write down, loss) to the federal government was originally said to be near $300 billion, depending on uptake, but independent estimates now put the full cost at $600 billion. This wipes out the hoped-for deficit reduction in the ridiculous but much ballyhooed “Inflation Reduction Act”, and yes, student loan forgiveness may well be inflationary. At a minimum, it makes the Fed’s job of restraining inflation by tamping down demand that much harder. Loan forgiveness will not solve the underlying problem of runaway cost escalation in higher education. In fact, it will exacerbate the problem by encouraging non-payment and additional borrowing, while tuition to colleges and universities will escalate all the more. So this is really bad policy all the way around!
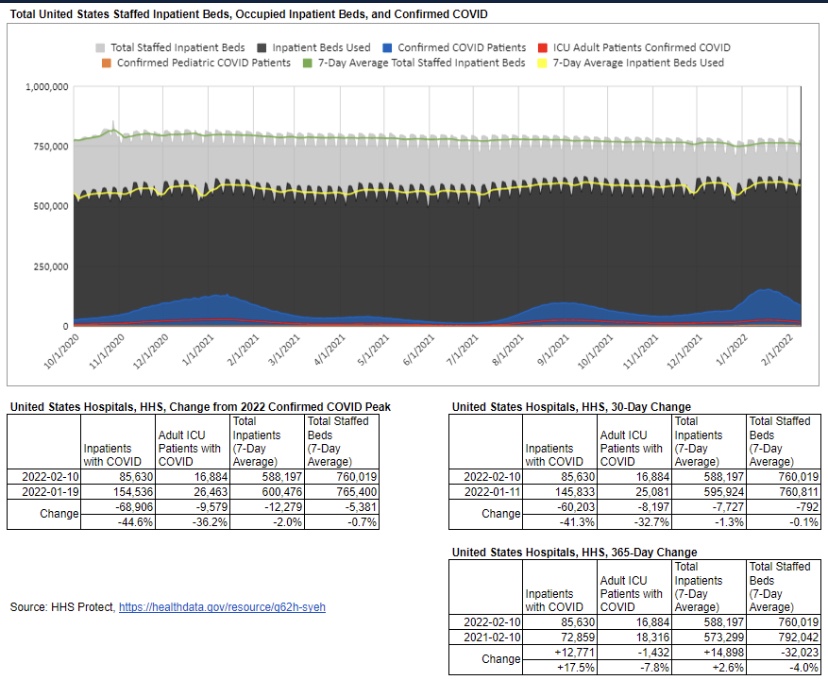
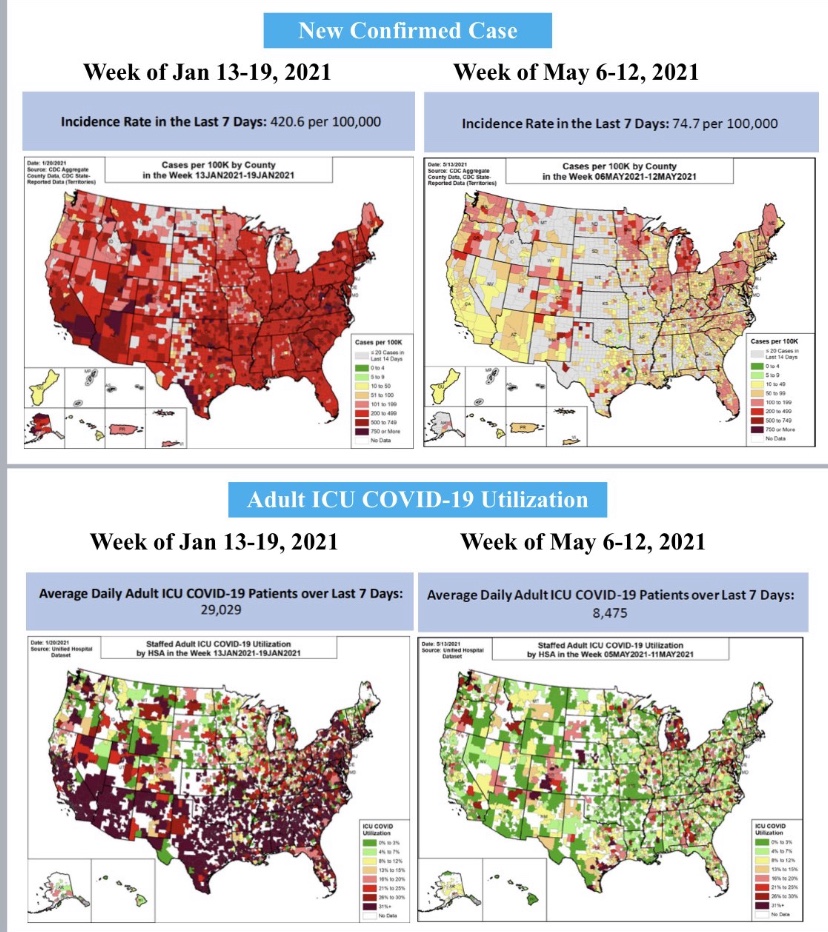
Biden’s action is clearly a huge stretch on statutory grounds. In particular, the Administration invoked the HEROES Act, which authorizes the Secretary of Education to waive loan requirements during periods of national emergency. In this case, the Administration appeals to hardships caused by the pandemic for individuals with student debt. Of course, just two weeks ago, the CDC rolled back their emergency pandemic guidelines on social distancing and quarantines, so the “emergency” seems to be over, officially. Also, the Administration recently ended the “return to Mexico” policy at the border on the pretext that it had only been necessary because of the pandemic! Pardon my incredulity, but playing the “pandemic card” at this point is both dishonest and hypocritical.
“Standing” in the legal sense can’t be found in the text of the Constitution. It was itself created by the courts. Even so, why do taxpayers, Congress, or past borrowers lack standing to challenge the action on student loans through the judicial system? How can that be when the harms are so obvious? Well, courts tend to avoid interfering with the executive branch, and they’d rather leave such disputes up to the political system to hash out. That doesn’t seem like a terribly effective way to practice the game of “checks and balances”. Nevertheless, for many years the courts have relied on a strict test for establishing plaintiff standing promulgated in the Supreme Court decision in Lujan v. Defenders of Wildlife. In that majority opinion, Justice Antonin Scalia laid out a three-part test, which Hoover describes thusly:
“… (1) injury in fact that is actual, concrete, and particularized; (2) a causal connection between the injury and the conduct complained of; and (3) a likelihood that exercise of judicial power will redress the injury.28 The Court furthermore differentiated between cases in which government regulation targets the plaintiff and cases where the plaintiff complains about ‘unlawful regulation (or lack of regulation) of someone else,’ in which case “much more is needed” for standing to exist.29 The Court has regularly reaffirmed this formulation of its standing requirements.3”
Hoover discusses the executive’s authority to cancel debt under the Higher Education Act (HEA) of 1965. In terms of the impregnability of Biden’s action to legal challenge, Hoover implies that the president might just as well have fallen back on HEA as HEROES. However, the Department of Education (DOE) opined last year that it lacked the power to forgive debt. Here’s what the DOE said in 2021:
“… the Secretary does not have statutory authority to provide blanket or mass cancellation, compromise, discharge, or forgiveness of student loan principal balances, and/or materially modify the repayment amounts or terms thereof, whether due to the COVID-19 pandemic or for any other reason.”
Hoover seems to be saying that it is all but impossible to challenge Biden’s bald assertion of extra-legal power in forgiving student loans. Hoover goes on to discuss all classes of potential litigants who might challenge student loan forgiveness: taxpayers, former borrowers, Congress, state governments, and loan servicers. He is skeptical of all those, citing various reasons for their lack of standing, but I’ll focus on only the first three classes.
Taxpayers: The logic of denying taxpayers standing is at least two-fold. First, taxpayers cannot show direct harm from the action, though they are likely to pay a higher inflation tax over time as a consequence. Second, Congress appropriated funds for student loans, but it did so as an entitlement, and it did not restrict loan amounts nor the executive’s ability to waive “the government’s claim that borrowers must return the funds to the Treasury”. Hoover believes that the courts would defer to the political branches of government in settling such issues. The whole thing sounds rather thin to my ears, but precedent will probably hold sway unless the Supreme Court revisits its position on standing.
Congress: The standing of Congress is another matter. If, in the view of the legislature, an executive agency has exceeded its statutory authority, the matter might reflect as much on Congress as elsewhere, in failing to provide adequate limitations, guideposts, or oversight. However, in this case:,
“Congress duly appropriated funds for student loans,83 and the Executive is responsible for the funding’s disbursement. This means that any claim of standing due to institutional injury from compromising Congress’s control of the federal purse would fail.”
Here again, it will be left to settle by the political branches of government. To avoid such conflicts, it is up to the legislature to write laws that bind the discretion of the executive to varying degrees. Unrestrained entitlements are a damn good way to cede control of the “keys to the Treasury”.
Other borrowers who’ve managed their student loan debt responsibly will also lack standing, according to Hoover. Like taxpayers, they cannot show any direct harm or injury. In addition, standing is difficult to establish when an action or inaction by an executive agency pertains to someone else.
It’s my hope that a court challenge will be brought all the way to the Supreme Court, and at some level a court will define a new standard or test under which plaintiffs can attempt to establish standing against executive or agency actions. This is sorely needed as a check on the explosive growth of the administrative state. Furthermore, the “standing dead zone” allows all sorts of politically-motivated mischief by the executive branch, and the Biden Administration seems more than willing to push executive authority to extremes. However, I’m not too optimistic about the possibility of a new test for standing. Before all is said and done, Biden is likely to expand student loan forgiveness well beyond $20,000 per borrower. Federal finance is looking more precarious with Biden’s every step, and many of those steps cannot be walked back by Congress, no matter who holds the majority.