Tags
Anders Tegnell, Closures, Coronavirus, Covid-19, Deaths of Despair, European Economic Area, Excess Deaths, Joakim Book, Johan Giesecke, Latitude, Lockdowns, Non-Pharmaceutical interventions, Nordic, NPIs, Our World In Data, Oxford Stringency Index, Pandemic, Quarantines, Sweden, Vitamin D
When Covid-19 began its awful worldwide spread in early 2020, the Swedes made an early decision that ultimately proved to be as protective of human life as anything chosen from the policy menu elsewhere. Sweden decided to focus on approaches for which there was evidence of efficacy in containing respiratory pandemics, not mere assertions by public health authorities (or anyone else) that stringent non-pharmaceutical interventions (NPIs) were necessary or superior.
The Swedish Rationale
The following appeared in an article in Stuff in late April, 2020,
“Professor Johan Giesecke, who first recruited [Sweden’s State epidemiologist Anders] Tegnell during his own time as state epidemiologist, used a rare interview last week to argue that the Swedish people would respond better to more sensible measures. He blasted the sort of lockdowns imposed in Britain and Australia and warned a second wave would be inevitable once the measures are eased. ‘… when you start looking around at the measures being taken by different countries, you find very few of them have a shred of evidence-base,’ he said.
Giesecke, who has served as the first Chief Scientist of the European Centre for Disease Control and has been advising the Swedish Government during the pandemic, told the UnHerd website there was “almost no science” behind border closures and school closures and social distancing and said he looked forward to reviewing the course of the disease in a year’s time.”
Giesecke was of the opinion that there would ultimately be little difference in Covid mortality across countries with different pandemic policies. Therefore, the least disruptive approach was to be preferred. That meant allowing people to go about their business, disseminating information to the public regarding symptoms and hygiene, and attempting to protect the most vulnerable segments of the population. Giesecke said:
“I don’t think you can stop it. It’s spreading. It will roll over Europe no matter what you do.”
He was right. Sweden had a large number of early Covid deaths primarily due to its large elderly population as well as its difficulty in crafting effective health messages for foreign-speaking immigrants residing in crowded enclaves. Nevertheless, two years later, Sweden has posted extremely good results in terms of excess deaths during the pandemic.
Excess Deaths
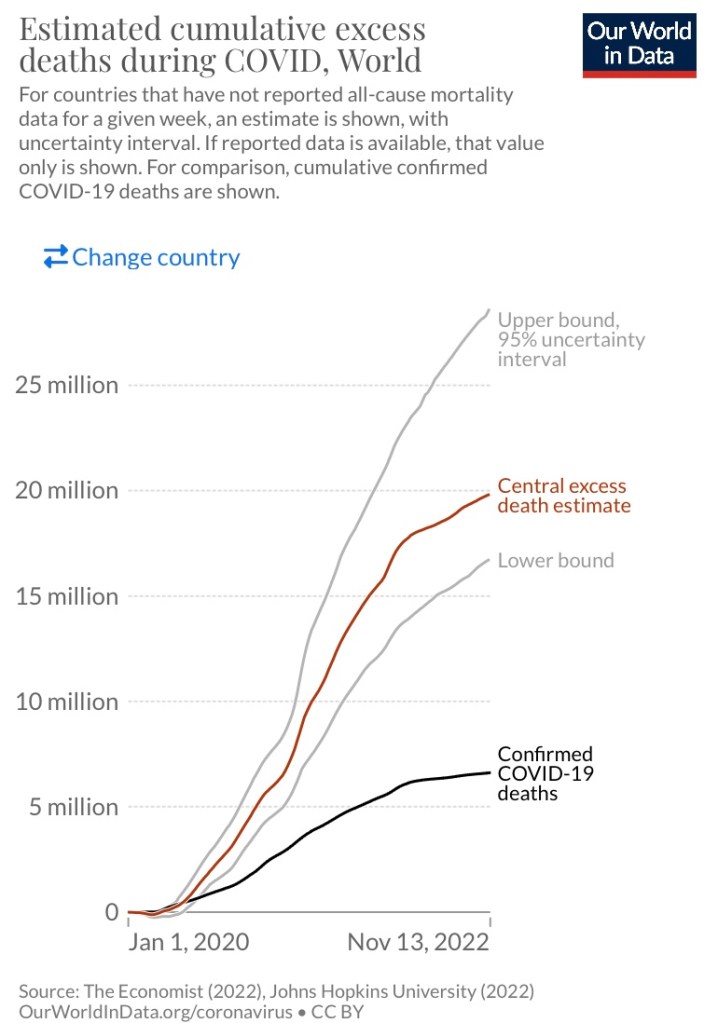
Excess deaths, or deaths relative to projections based on historical averages, are a better metric than Covid deaths (per million) for cross-country or jurisdictional comparisons. Among other reasons, the latter are subject to significant variations in methods of determining cause of death. Moreover, there was a huge disparity between excess deaths and Covid deaths during the pandemic, and the gap is still growing:
Excess deaths varied widely across countries, as illustrated by the left-hand side of the following chart:
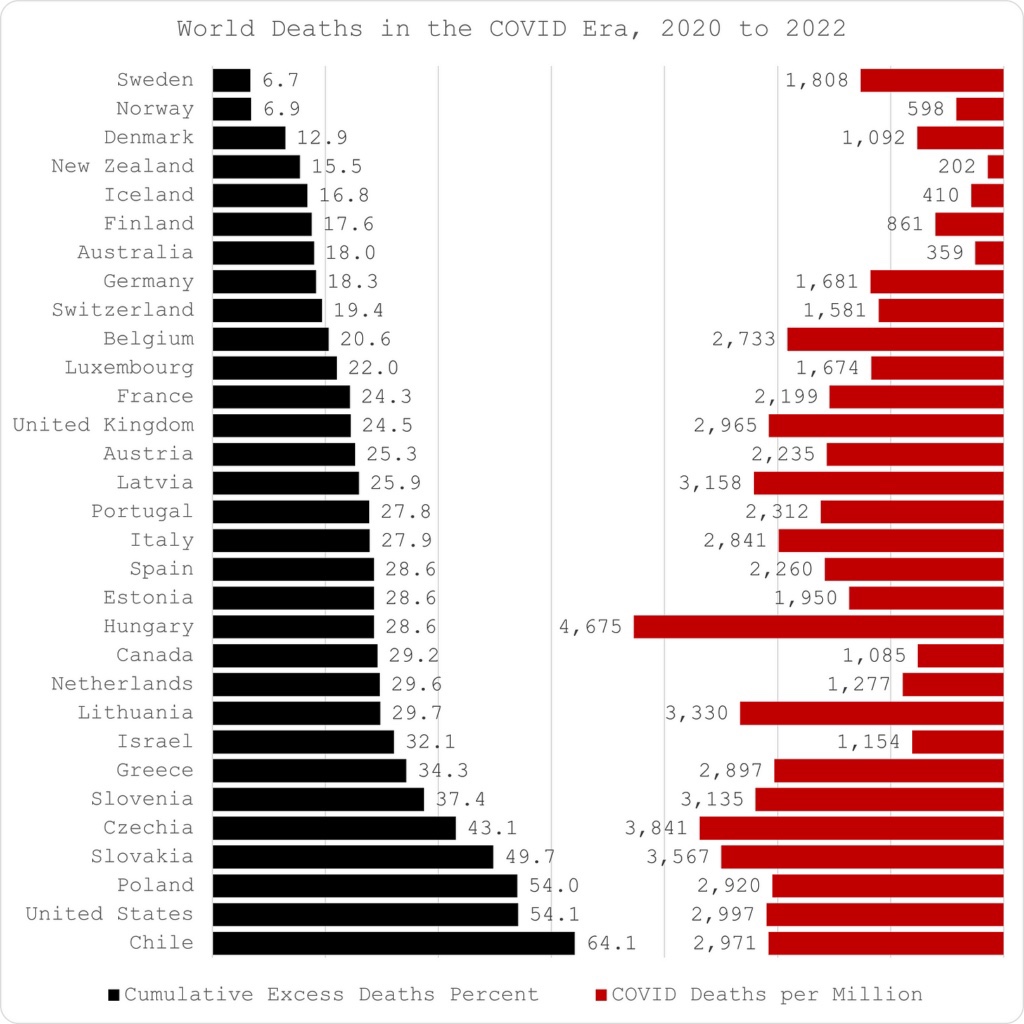
Interestingly, most of the lowest excess death percentages were in Nordic countries, but especially Sweden and Norway. That might be surprising in terms of high Nordic latitudes, which may have created something of a disadvantage in terms of sun exposure and potentially low vitamin D levels. Norway enacted more stringent public policies during the pandemic than Sweden. Globally, however, lockdown measures showed no systematic advantage in terms of excess deaths. Notably, the U.S. did quite poorly in terms of excess deaths at 8X the Swedish rate,
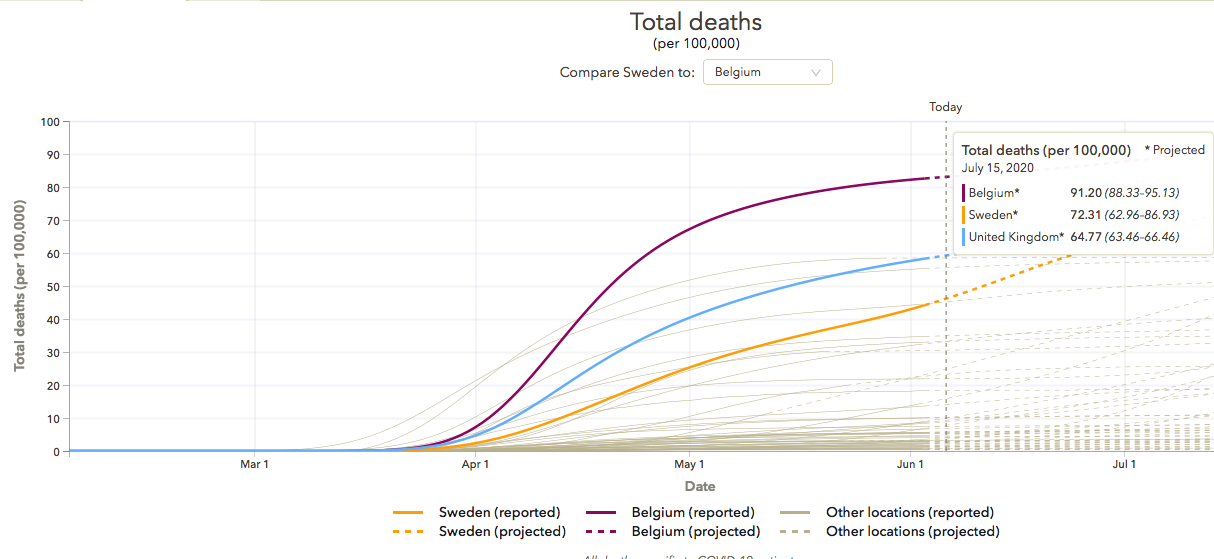
Covid Deaths
The right-hand side of the chart above shows that Sweden experienced a significant number of Covid deaths per million residents. The figure still compares reasonably well internationally, despite the country’s fairly advanced age demographics. Most Covid deaths occurred in the elderly and especially in care settings. Like other places, that is where the bulk of Sweden’s Covid deaths occurred. Note that U.S. Covid deaths per million were more than 50% higher than in Sweden.
NPIs Are Often Deadly
Perhaps a more important reason to emphasize excess deaths over Covid deaths is that public policy itself had disastrous consequences in many countries. In particular, strict NPIs like lockdowns, including school and business closures, can undermine public health in significant ways. That includes the inevitably poor consequences of deferred health care, the more rapid spread of Covid within home environments, the physical and psychological stress from loss of livelihood, and the toll of isolation, including increased use of alcohol and drugs, less exercise, and binge eating. Isolation is particularly hard on the elderly and led to an increase in “deaths of despair” during the pandemic. These were the kinds of maladjustments caused by lockdowns that led to greater excess deaths. Sweden avoided much of that by eschewing stringent NPIs, and Iceland is sometimes cited as a similar case.
Oxford Stringency Index
I should note here, and this is a digression, that the most commonly used summary measure of policy “stringency” is not especially trustworthy. That measure is an index produced by Oxford University that is available on the Our World In Data web site. Joakim Book documented troubling issues with this index in late 2020, after changes in the index’s weightings dramatically altered its levels for Nordic countries. As Book said at that time:
“Until sometime recently, Sweden, which most media coverage couldn’t get enough of reporting, was the least stringent of all the Nordics. Life was freer, pandemic restrictions were less invasive, and policy responses less strong; this aligned with Nordic people’s experience on the ground.”
Again, Sweden relied on voluntary action to limit the spread of the virus, including encouragement of hygiene, social distancing, and avoiding public transportation when possible. Book was careful to note that “Sweden did not ‘do nothing’”, but it’s policies were less stringent than its Nordic neighbors in several ways. While Sweden had the same restrictions on arrivals from outside the European Economic Area as the rest of the EU, it did not impose quarantines, testing requirements, or other restrictions on travelers or on internal movements. Sweden’s school closures were short-lived, and its masking policies were liberal. The late-2020 changes in the Oxford Stringency Index, Book said, simply did not “pass the most rudimentary sniff test”.
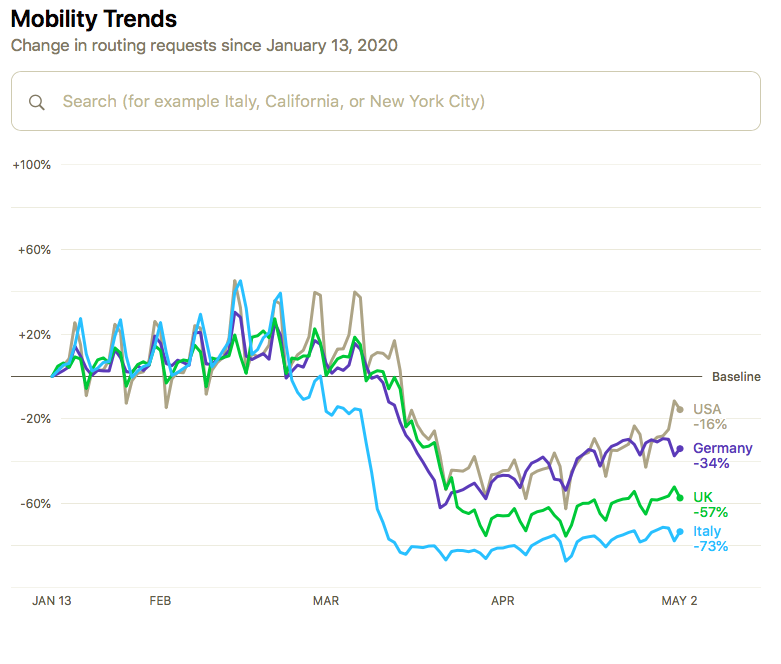
Economic Stability
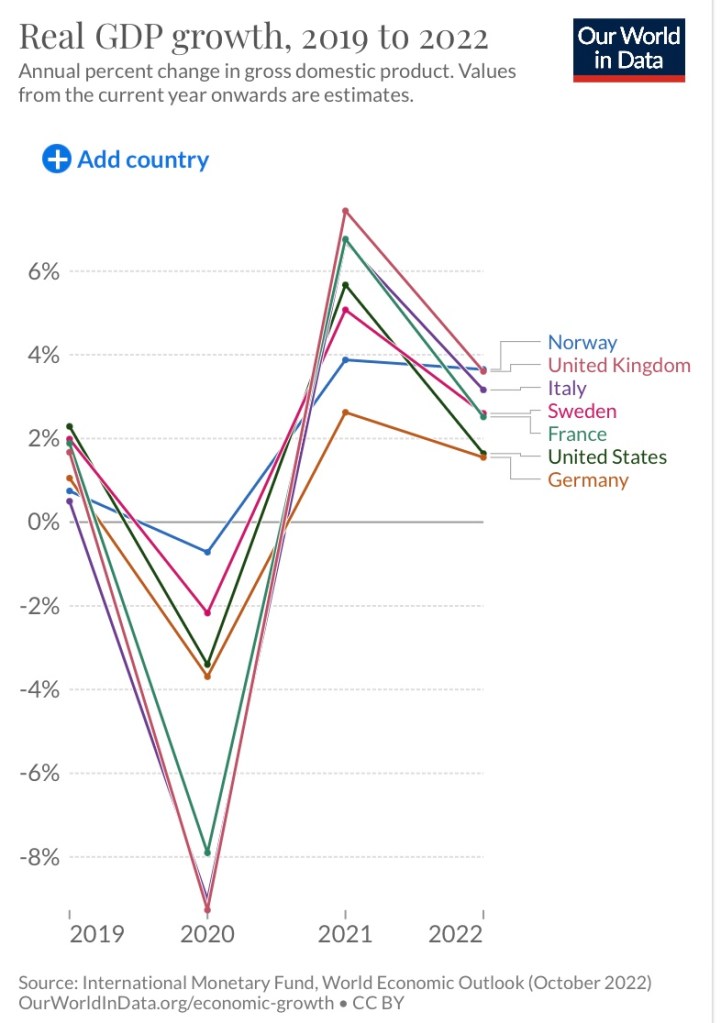
Sweden’s economy performed relatively well during the pandemic. The growth path of real GDP was smoother than most countries that succumbed to the excessive precautions of lockdowns. However, Norway’s economy appears to have been the most stable of those shown on the chart, at least in terms of real output, though it did suffer a spike in unemployment.
The Bottom Line
The big lesson is that Sweden’s “light touch” during the pandemic proved to be at least as effective, if not more so, than comparatively stringent policies imposed elsewhere. Covid deaths were sure to occur, but widespread non-Covid excess deaths were unanticipated by many countries practicing stringent intervention. That lack of foresight is best understood as a consequence of blind panic among public health “experts” and other policymakers, who too often are rewarded for misguided demonstrations that they have “done something”. Those actions failed to stop the spread in any systematic sense, but they managed to do great damage to other aspects of public health. Furthermore, they undermined economic well being and the cause of freedom. Johan Giesecke was right to be skeptical of those claiming they could contain the virus through NPIs, though he never anticipated the full extent to which aggressive interventions would prove deadly.