
Tags
Cause of Death, CDC, Civid-Only Deaths, Co-Morbidities, Coronavirus, Covid-19, Denmark Covid, Eastern Europe Covid, Euromomo, Excess Mortality, Germany Covid, Jacob Sullum, John Burn-Murdoch, New York Covid, New York Times, Probable Covid Deaths
The New York Times ran a piece this week suggesting that excess mortality from Covid-19 in the U.S. is, or will be, quite high. The analysis was based on seven “hard hit” states, including three of the top four states in Covid death rate and five of the top ten. Two states in the analysis, New York and New Jersey, together account for over half of all U.S. active cases. This was thinly-veiled cherry picking by the Times, as Jacob Sullum notes in his discussion of what excess mortality does and doesn’t mean. Local and regional impacts of the virus have varied widely, depending on population density, international travel connections, cultural practices, the quality of medical care, and private and public reaction to news of the virus. To suggest that the experience in the rest of the country is likely to bear any similarity to these seven states is complete nonsense. Make no mistake: there have been excess deaths in the U.S. over the past few weeks of available data, but again, not of the magnitude the Times seems to intimate will be coming.
Beyond all that, the Times asserts that the CDC’s all-cause death count as of April 11 is a significant undercount, though the vast majority of deaths are counted within a three week time frame. In fact, CDC data at this link show that U.S. all-cause mortality was at a multi-year low during the first week of April. The author admits, however, that the most recent data is incomplete. The count will rise as reporting catches up, but even an allowance for the likely additions to come would leave the count for the U.S. well below the kinds of levels suggested by the Times‘s fear-mongering article, based as it was on the seven cherry-picked states.
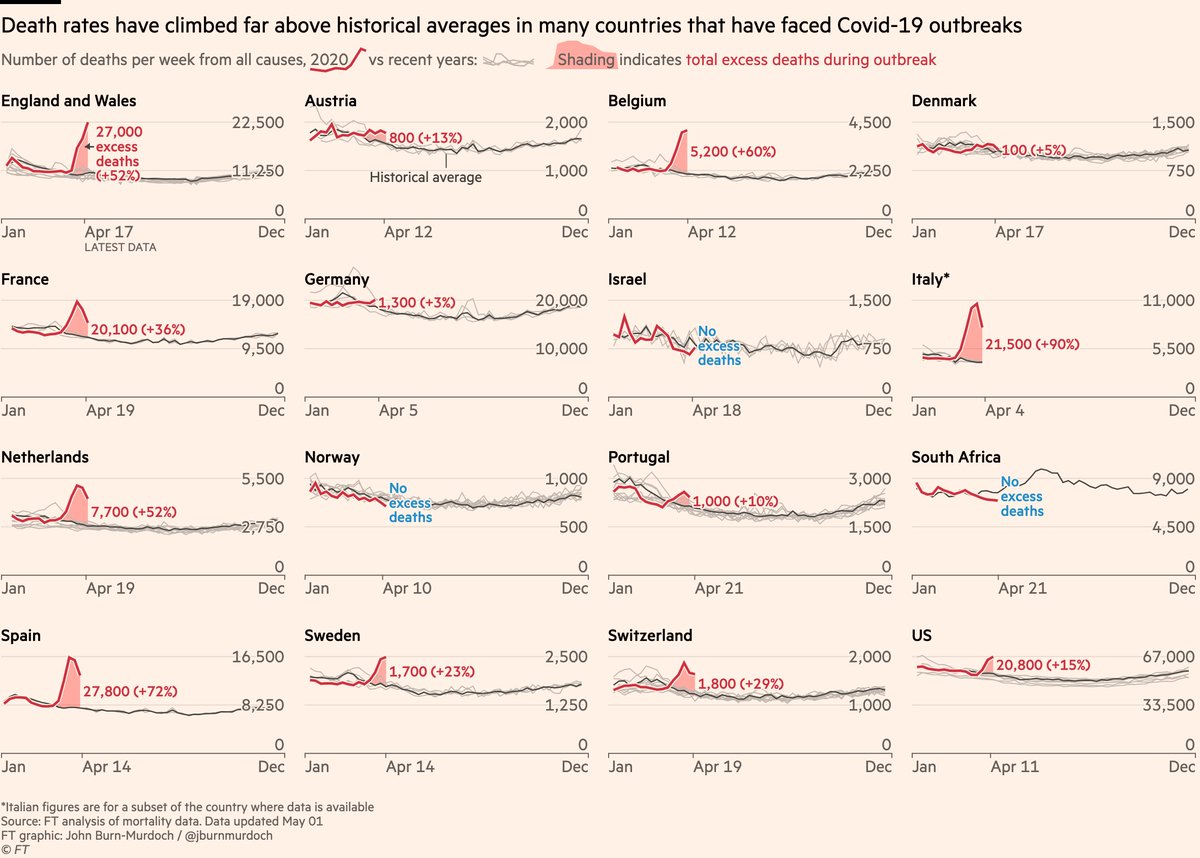
The author of this Twitter thread, John Burn-Murdoch, seems to engage in the same practice with respect to Europe. He shows charts with excess deaths in 12 countries, almost all of which show significant, recent bumps in excess deaths (the sole exception being Denmark). Inexplicably, he excludes Germany and a number of other countries with low excess deaths or even “valleys” of negative excess deaths. His most recent update is a bit more inclusive, however. (It was the source of the chart at the top of this post.) Euromomo is a site that tracks excess mortality in 24 European countries or major regions (non-overlapping), and by my count, 13 of have no or very little excess mortality. And by the way, even this fails to account for a number of other Eastern European nations having low Covid deaths.
Excess mortality is a tricky metric: it cannot be measured with certainty, and almost any measure has conceptual shortcomings. In the case of Covid-19, excess mortality seeks to measure the number of deaths attributable to the virus net of deaths that would have occurred anyway in the absence of the virus. For example, abstracting from some of the details, suppose there are 360 deaths per hundred-thousand of population during the average month of a pandemic. If the “normal” mortality rate is 60 per hundred-thousand, then excess mortality is 300 per month. It can also be expressed as a percentage of the population (0.3% in the example). But that’s just one way to measure it.
In the spirit of Sullum’s article, it’s important to ask what we’re trying to learn from statistics on excess mortality. It’s easy to draw general conclusions if the number of Covid-19 deaths is far in excess of the normal death rate, but that depends on the quality of the data, and any conclusion is subject to limits on its applicability. Covid deaths are not that high in many places. By the same token, if the number of Covid deaths (defined narrowly) is below the normal death rate (measured by an average of prior years), it really conveys little information about whether excess mortality is positive of negative: that depends on the nature of the question. For each of the following I offer admittedly preliminary answers:
- Are people dying from Covid-19? Of course, virtually everywhere. There is no “normal” death rate here. And while this is the most direct question, it might not be the “best” question.
- Is Covid-19 causing an increase in respiratory deaths? Yes, in many places, but perhaps not everywhere. Here and below, the answer might depend on the time frame as well.
- Is Covid-19 increasing deaths from infectious diseases (biological and viral)? Yes, but perhaps not everywhere.
- Is Covid-19 increasing total deaths from natural causes? Yes, but not everywhere.
- Is all-cause mortality increasing due to Covid-19? In some places, not others. Accurate global and national numbers are still a long way off.
All-cause mortality is the most “rough and ready” comparison we have, but it includes deaths that have no direct relationship to the disease. For example, traffic fatalities might be down significantly due to social distancing or regulation during a pandemic. Thus, if our purpose is purely epidemiological, traffic fatalities might bias excess mortality downward. On the other hand, delayed medical treatments or personal malaise during a pandemic might lead to higher deaths, creating an upward bias in excess deaths via comparisons based on all-cause mortality.
Do narrow comparisons give a more accurate picture? If we focus only on respiratory deaths then we exclude deaths from other causes and co-morbidities that would have occurred in the absence of the virus. That may create a bias in excess mortality. So narrow comparisons have their drawbacks, depending on our purpose.
That also goes for the length of time over which excess mortality is measured. It can make a big difference. Again, much has been made of the fact that so many victims of Covid-19 have been elderly or already ailing severely before the pandemic. There is no question that some of these deaths would have occurred anyway, which goes to the very point of calculating excess mortality. If the pandemic accelerates death by a matter of weeks or months for a certain percentage of victims, it is reasonable to measure excess mortality over a lengthier period of time, despite the (perhaps) highly valuable time lost by those victims (that being dependent on the decedent’s likely quality of life during the interval).
Conversely, too narrow a window in time can lead to biases that might run in either direction. Yet a cottage industry is busy calculating excess mortality even as we speak with the pandemic still underway. There are many fatalities to come that are excluded by premature calculations of excess mortality. On the other hand, if the peak in deaths is behind us, a narrow window and premature calculation may sharply exaggerate excess mortality.
Narrow measures of excess mortality are affected by the accuracy of cause-of-death statistics. There are always inaccuracies in this data because so many deaths involve multiple co-morbidities, so there is often an arbitrary element in these decisions. For Covid-19, cause-of-death attribution has been extremely problematic. Some cases are easy: those testing positive for the virus, or even its presence immediately after death, and having no other respiratory infections, can fairly be counted as Covid-19 deaths. But apparently just over half of Covid-19 deaths counted by the CDC are “Covid-Only” deaths. A significant share of deaths involve both Covid and the flu, pneumonia, or all three. There are also “probable” Covid-19 deaths now counted without testing. In fact, hospitals and nursing homes are being encouraged to code deaths that way, and there are often strong financial incentives to do so. Many deaths at home, sans autopsy, are now routinely classified as Covid-19 deaths. While I have no doubt there are many Covid deaths of untested individuals both inside or outside of hospitals, there is no question this practice will overcount Covid deaths. Whether you believe that or not, doubts about cause-of-death accuracy is another reason why narrow comparisons can be problematic.
More trustworthy estimates of the coronavirus’ excess mortality will be possible with the passage of time. It’s natural, in the heat of the pandemic, to ask about excess mortality, but such early estimates are subject to tremendous uncertainty. Unfortunately, those calculations are being leveraged and often mis-applied for political purposes. Don’t trust anyone who would use these statistics as a cudgel to deny your Constitutional rights, or otherwise to shame or threaten you.
New York’s Covid experience is not applicable to the country as a whole. Urban mortality statistics are not applicable to areas with lower population densities. Excess mortality for the elderly cannot be used to make broad generalizations about excess mortality for other age groups. And excess mortality at the peak of a pandemic cannot be used to make generalizations about the full course of the pandemic. In the end, I expect Covid-19 excess mortality to be positive, whether calculated by all-cause mortality or more narrow measures. However, it will not be uniform in its impact. Nor will it be of the magnitude we were warned to expect by the early epidemiological models.

What utter nonsense. History will be the judge.
To what specifically do you refer? Please articulate.