Tags
Anaphylaxis, Antivax Propaganda, Bell’s Palsy, Breakthrough Infections, Co-Morbidities, Covid-19, Delta Variant, Hulk Syndrome, Mask Mandates, Myocarditis/Pericarditis, Natural Immunity, Non-Pharmaceutical interventions, Vaccination, Vaccine Adverse Events Reporting System, Vaccine Hesitancy, Vaccine Mandates, Vaccine Passports, VAERS

I was vaccinated in March and early April and I’m damn glad to have done it. I have certain co-morbidities, and I’m of an age at which contracting COVID seems like a very bad idea, I felt a little run-down on the day after my second jab, but that was my only side effect, notwithstanding the unending litany of antivax hysterics to which we’ve all been subjected (even on certain sites to which I contribute).
Freedom Without Misinformation
In the context of the pandemic, it’s important to take a stand for liberty. In that spirit, I oppose the imposition of mandates requiring face masks and vaccinations against COVID. Furthermore, vaccination is at best unnecessary for those having acquired immunity from infection and for those at low risk, especially children. In fact, the younger, healthier, and fitter you are, the less important it is to be vaccinated.
It’s disappointing, however, to see completely innumerate people cite statistics purporting to show that COVID-19 vaccines are deadly or even particularly dangerous to those lacking contra-indications. Far worse, and far more idiotic, is to suggest that a conspiracy is afoot to kill large numbers of people via vaccination! I’m truly embarrassed to hear individuals who otherwise share my libertarian ideals say such irresponsible bullshit.
While the COVID vaccines seem to have more frequent side effects than earlier vaccines, they are not particularly risky. I’ll discuss the safety of the COVID vaccines in what follows. Even minuscule risks are unacceptable to some individuals, which of course is their right. However, others find these risks acceptable considering the far greater dangers posed by the early strains of COVID and even the more recent but less deadly Delta variant.
Unverified Adverse Events
The vaccine scaremongers often quote statistics from the CDC’s Vaccine Adverse Reporting Events System (VAERS). Here’s a disclaimer about the system from the CDC’s web site:
“Healthcare providers, vaccine manufacturers, and the public can submit reports to VAERS. While very important in monitoring vaccine safety, VAERS reports alone cannot be used to determine if a vaccine caused or contributed to an adverse event or illness. The reports may contain information that is incomplete, inaccurate, coincidental, or unverifiable.”
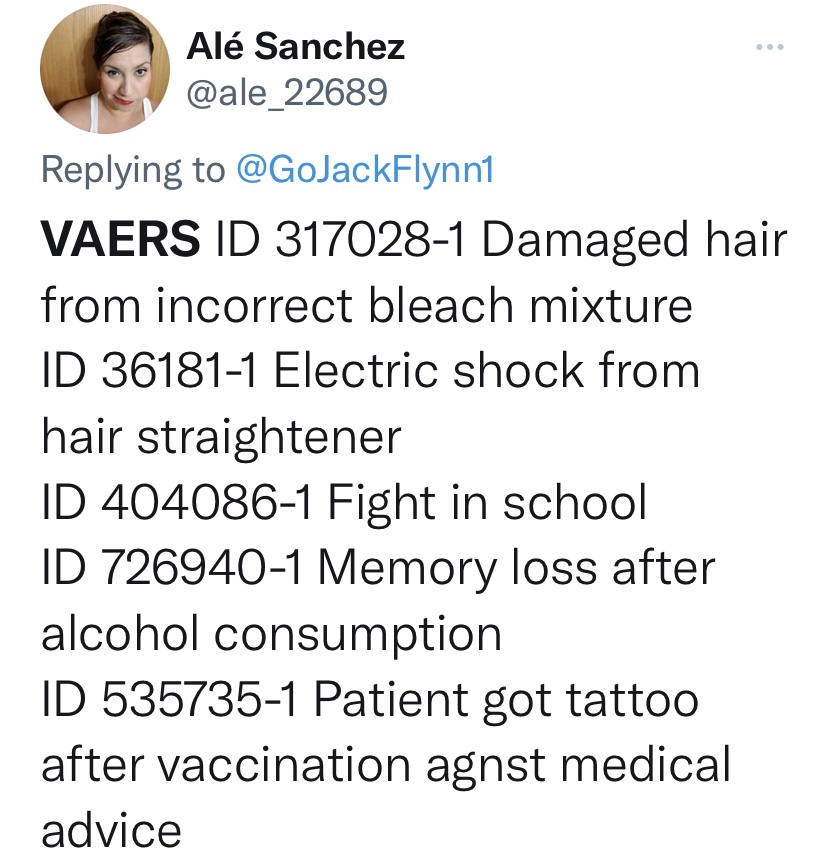
All kinds of reports are submitted alleging adverse events. For example, one observer cites the following reports from the system:
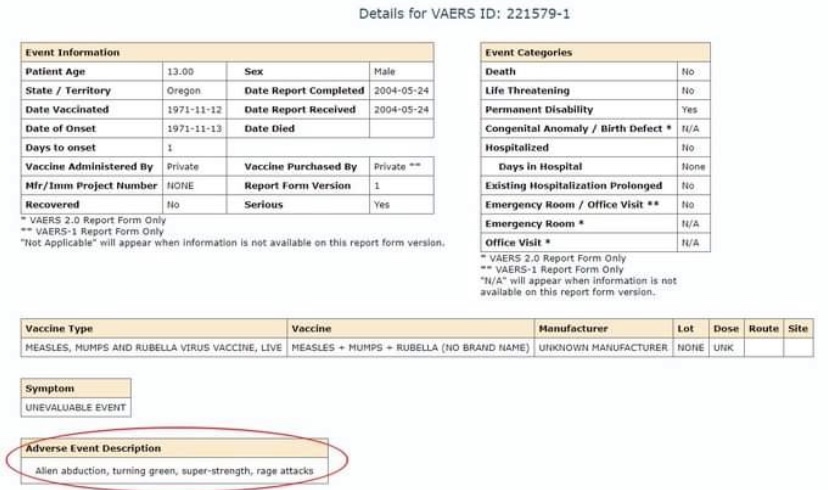
The link above refers to the following report as “Hulk Syndrome”, which was alleged to have been a side effect of the MMR vaccine:
Finally, we have this report related to the Pfizer COVID vaccine:
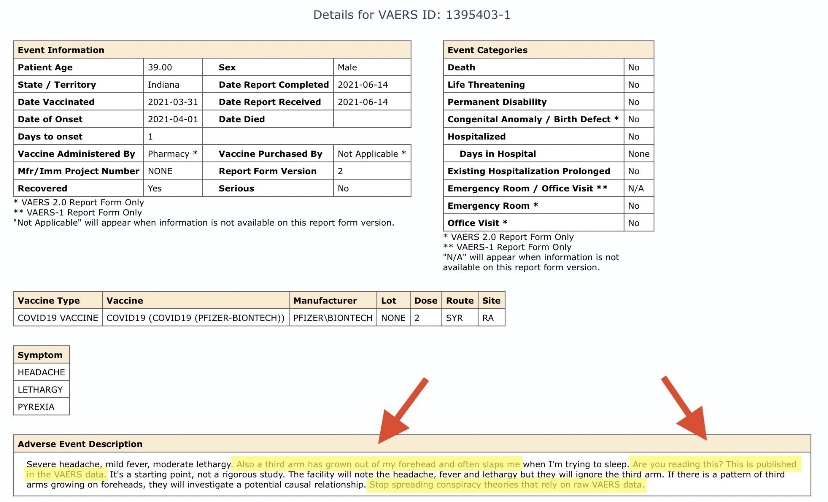
In case that’s hard to read, it claims that a COVID vaccine caused a third arm to grow from the reporting individual’s forehead, which constantly slaps him or her while trying to sleep. This report is a case of wonderful sarcasm, but it was submitted to VAERS! The real lesson is that the VAERS system collects many unverified accounts of side effects, so the aggregate counts of adverse events are not reliable, even by the CDC’s admission.
A More Sober Risk Assessment
Therefore, the VAERS system has obvious limitations. But even stipulating the use of VAERS reports, the risks of the COVID vaccines are vanishingly low. For example, roughly 198 million people in the U.S. have received at least one dose of a vaccine. As of last week, there had been about 13,600 reports of post-vaccination death in VAERS. The raw number is very high, and I don’t wish to minimize the seriousness of those losses. Nevertheless, if those deaths were all attributable to vaccination, and that is a BIG “if”, the risk of death from vaccination to-date is just 0.007%. That is seven thousandth of 1%.
To put those VAERS deaths into perspective, I should first add the caveat that I am highly skeptical of the COVID case and death statistics. Nevertheless, let’s take the official U.S. COVID death toll of 646,000 at face value. I’m also treating reported vaccine deaths from VAERS at face value, which is a huge stretch. So, we have COVID mortality of 0.2% of the U.S. population, which is more than 28 times the risk of death from vaccination. I grant you the risk posed by COVID is lower going forward than in the past, which is due both to vaccinations and the declining virulence of the virus itself.
There are a range of vaccine side effects reported in VAERS, from pain near the injection site to such alarming conditions as anaphylaxis, Bell’s Palsy, and myocarditis/pericarditis. VAERS would attribute over 54,000 hospitalizations to the vaccines, a rate of 3 hundredths of one percent of those receiving at least one dose. Like COVID deaths, the number of COVID hospitalizations is likely inflated. Still, at 1.9% of the U.S. population, the risk of hospitalization from COVID is 68 times that of hospitalization from vaccine side effects reported in VAERS.
A large share of VAERS reports, covering all adverse events, are from middle aged individuals. It’s unclear how concentrated that reporting is among those with co-morbidities, including obesity, but I suspect they are heavily represented.
Coincidental Events
Perhaps less obvious is that many sincere reports to VAERS from both the public and health care providers represent coincidental events. A number of states have given heavy vaccine priority to the elderly and those with co-morbidities, and demand from those groups has been disproportionate in any case. Most of the VAERS-reported deaths also happen to be among the elderly and co-morbids.
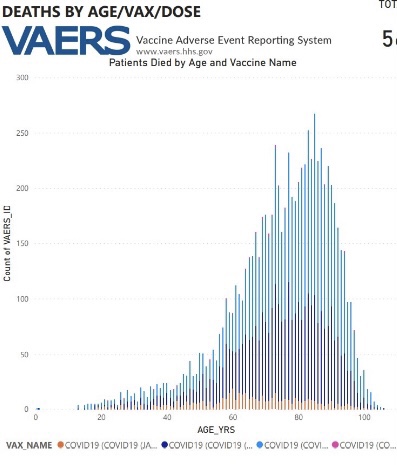
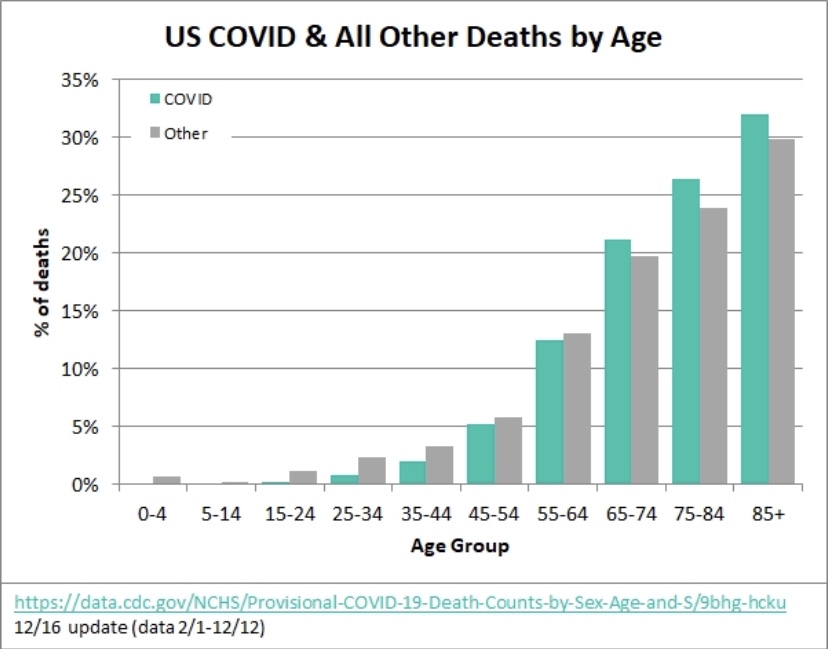
For example, more than 38% of VAERS death reports come from the 80+ age cohort, accounting for roughly 5,200 deaths. That’s four hundredths of one percent of the 12.9 million people of ages 80+ in the U.S., most of whom have been vaccinated. Well over 1.2 million 80+ year-olds can be expected to die each year under normal circumstances. That a few would occur within days, weeks, or months of a vaccination should be expected. Furthermore, it would not be surprising, given the controversy surrounding vaccines and the suggestive power of antivax propaganda, for families or some caregivers to imagine a connection between vaccination and subsequent death. File a report! Who knows? Perhaps a class action award might be in it someday.
This is not to deny that a small number of individuals could be in such weakened states, or perhaps have unknown vulnerabilities, that the vaccines have catastrophic consequences. No doubt there are a few deaths precipitated by COVID vaccines in combination with other conditions. However, a large share of the deaths reported to VAERS are likely to have been coincidental. Likewise, people develop conditions all the time… sore joints, rashes, coughs, and headaches. It runs the gamut. Some of the VAERS reports of a less serious nature are undoubtedly coincidental, and perhaps some are due to the vivid imaginations of a subset of those having consented to the vaccine with great reluctance.
What Kills and What Doesn’t
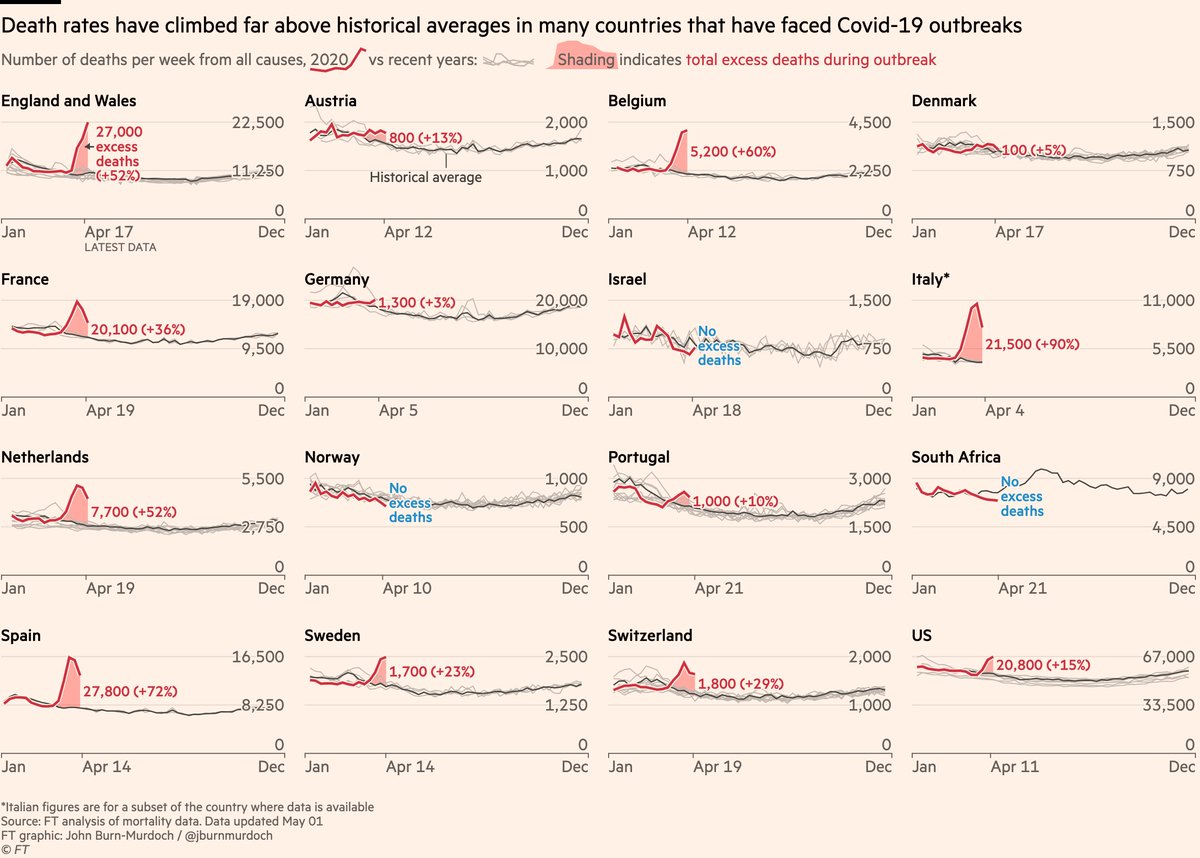
Everything comes with a risk, and tradeoffs between risks must be balanced. The COVID pandemic was deadly, and I’ll be the first to admit that I underestimated its potential to kill. However, its deadliness was magnified by the non-pharmaceutical interventions imposed in many jurisdictions. Lockdowns and closures took a massive toll on the health of the population, cutting short many lives due to economic and personal despair as well as deferred and cancelled health care. While those interventions were deadly, I do not believe that kind of harm was intended. I do suspect the concomitant assault on liberty was welcomed in certain circles.
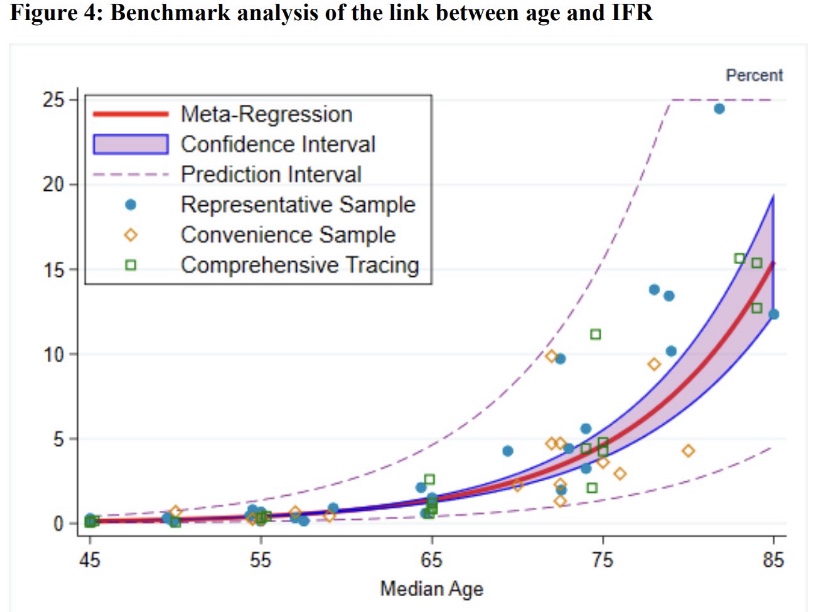
There are certainly downsides to the COVID vaccines. There have been more side effects and deaths than have ever been reported relative to earlier vaccines. It’s also a shame that public health authorities refuse to recognize the superior effects of natural immunity and the heightened risk of vaccinations to those with prior infections. And it’s a travesty that “vaccine passports” are now being demanded for various forms of travel, entertainment, and entry to some places of business. Despite these issues, it’s blatantly false to assert that the vaccines are generally harmful. Many more of the remaining vaccine-hesitant can benefit from vaccination. Let’s advocate for better assessments of risk by age and co-morbidity, and simply avoid the vaccines if that is your preference.
Addendum: I just came across this nice piece entitled “A Statistical Analysis of COVID-19 Breakthrough Infections and Deaths“. I thought I should share the link in case anyone supposes that so-called breakthrough infections somehow invalidate some of the comparisons I made above. This chart is particularly revealing: