
Tags
Andrew Bostom, Coffee Grounds Test, Covid-19, Ct, Cycle Threshold, False Positives, FDA, PCR Test, Rapid Tests, Rhode Island, Viral RNA
Here’s some incredible data on PCR tests demonstrating a radically excessive lab practice that generates false positives. I’m almost tempted to say we’d do just as well using a thermometer and the coffee ground test. Open a coffee tin and take a sniff. Can you smell the distinct aroma of the grounds? If not, and if you have other common symptoms, there’s a decent chance you have an active COVID infection. That test is actually in use in some parts of the globe!
The data shown below on PCR tests are from the Rhode Island Department of a Health and the Rhode Island State Health Lab. They summarize over 5,000 positive COVID PCR tests (collected via deep nasal swabs) taken from late March through early July. The vertical axis in the chart measures the cycle threshold (Ct) value of each positive test. Ct is the number of times the RNA in a sample must be replicated before any COVID-19 (or COVID-like) RNA is detected. It might be from a live virus or perhaps a fragment of a dead virus. A positive test with a low Ct value indicates that the subject is likely infected with billions of live COVID-19 viruses, while a high Ct value indicates perhaps a handful or no live virus at all.
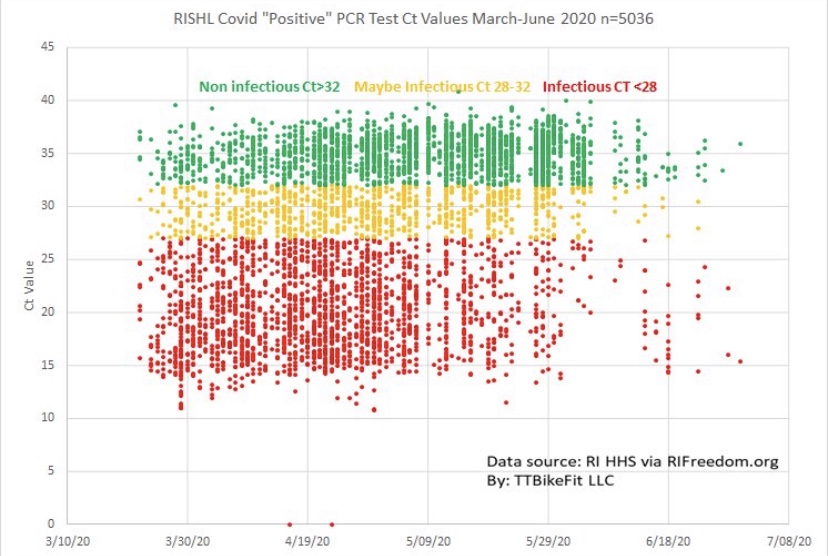
The range of red dots in the chart (< 28 Ct) indicates relatively low Ct values and active infections. The yellow range of dots, for which 28 < Ct <= 32, indicates possible infections, and the upper range of green dots, where Ct > 32, indicates that active infections were highly unlikely. It’s important to note that all of these tests were recorded as new COVID cases, so the range of Ct values suggest that testing in Rhode Island was unreasonably sensitive. That’s broadly true across the U.S. as well, which means that COVID cases are over-counted by perhaps 30% or more. And yet it is extremely difficult for subjects testing positive to learn their Ct values. You can ask, but you probably won’t get an answer, which is absurd and counterproductive.
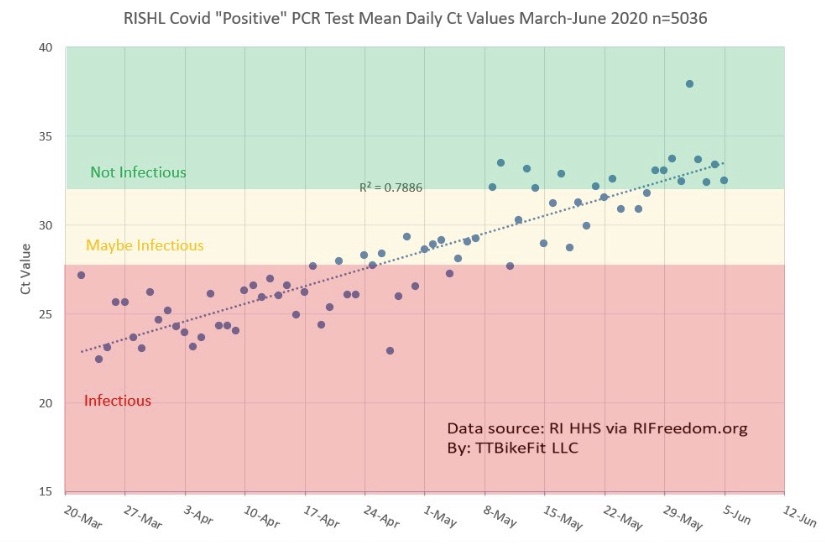
Notice that the concentration of red dots diminished over time, and we know that the spring wave of the virus in the Northeast was waning as the summer approached. The share of positives tests with high Ct values increased over that time frame, however. This is borne out by the next chart, which shows the daily mean Ct of these positive tests. The chart shows that active infections became increasingly rare over that time frame both because positive tests decreased and the average Ct value rose. What we don’t know is whether labs bumped up the number of cycles or replications to which samples were subjected. Still, the trend is rather disturbing because most of the positive cases in May and the first half of June were more likely to be virus remnants than live viruses.
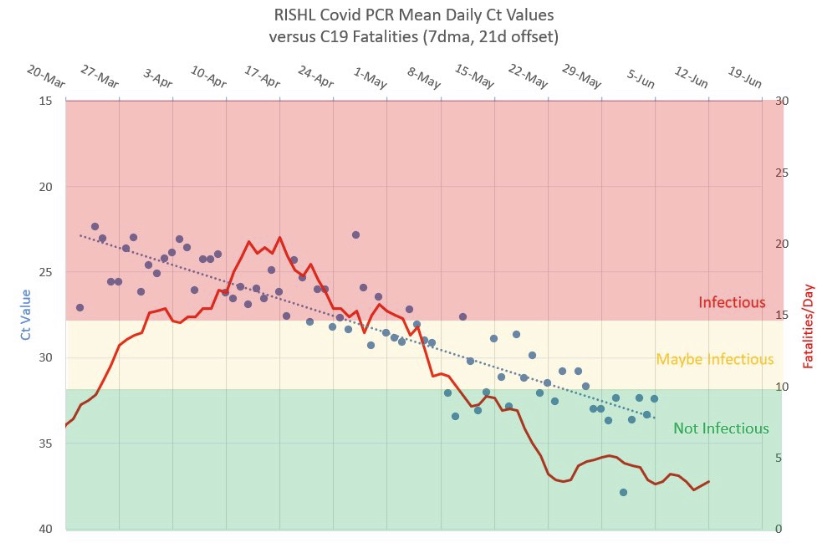
It’s also worth noting that COVID deaths declined in concert with the upward trend in Ct values. This is shown in the chart below (where the Ct scale is inverted). This demonstrates the truly benign nature of positive tests having high Ct values.
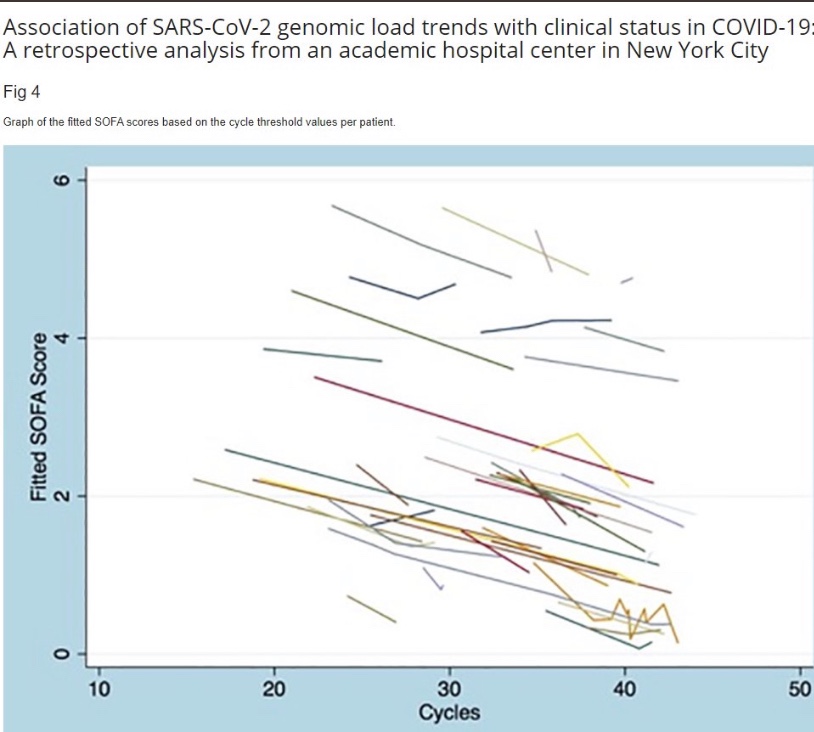
This is also demonstrated by the following data from a New York City academic hospital, which was posted by Andrew Bostom. It shows that a more favorable “clinical status” of COVID patients is associated with higher Ct values.
It’s astounding that the U.S. has relied so heavily on a diagnostic tool that gets so many subjects wrong. And it’s nearly impossible for subjects testing positive to obtain their Ct values. Instead, they are subject to self-quarantine for up to two weeks. Even worse, until recently there were delays in reporting the results of these tests of up to a week or more. That made them extremely unhelpful. On the other hand, the coffee ground test is fast and cheap, and it might enhance the credibility of a subsequent positive PCR test, if one is necessary … and especially if the lab won’t report the Ct value.
The PCR test has identified far too many false infections, but it wouldn’t have been quite so damaging if 1) a reasonably low maximum cycle threshold had been established; 2) test results had not been subject to such long delays; and 3) rapid retests had been available for confirmation. The cycle threshold issue is starting to receive more attention, quite belatedly, and more rapid tests have become available. As I’ve emphasized in the past, cheap, rapid tests exist. But having dithered in February and March in approving even the PCR test, the FDA has remained extremely grudging in approving newer tests, and it persists in creating obstacles to their use. The FDA needs to wake up and smell the coffee!



