Tags
Adverse Events, Anti-Coagulants, Avoidable Deaths, Blood Clotting, Blood Thinners, CDC, Covid-19, Death of Expertise, Deaths of Despair, Deferred Care, Emergency Use Authorization, EUA Shadow Deaths, Excess Deaths, Incidental Infections, Lockdown Deaths, Omicron Variant, Our World In Data, Post-Mortem Testing, Prime Age Deaths, Randomized Control Trials, The Ethical Skeptic, USMortality.com, Vaccine Efficacy, Vascular Integrity

Understanding the severity of the coronavirus pandemic is more straightforward when measured in terms of excess deaths, rather than total Covid deaths. We’ve had a large number of excess deaths in the U.S., but not all of them can be attributed to Covid. It’s also worth asking whether some of the deaths were avoidable, because that reflects even more profoundly on the success or failure of public policy and the health care system in dealing with the challenge. Unfortunately, while the precise number of avoidable deaths the nation has suffered is speculative, it is nevertheless significant.
Bad Metrics
A huge problem with using total Covid deaths as a measure of pandemic severity is that no one is confident in the accuracy of official statistics. There are reasons to suspect over-counting in the U.S. due to financial incentives created for hospital systems by the CARES Act. These were exacerbated by the CDC’s absurd 2020 recommendations for the completion of death certificates. Essentially, any non-primary Covid entry on a death certificate was sufficient to count the death as from Covid. No other disease is or has ever been tallied like that.
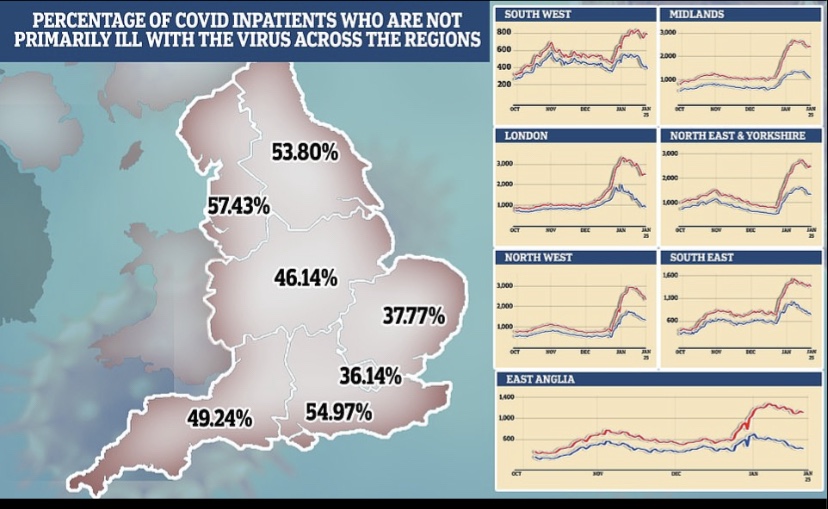
There is an important distinction between deaths “with Covid” and deaths “from Covid” that has been acknowledged only recently by health authorities. A death “with Covid” can occur when a patient tests positive for Covid after being admitted to a hospital for another primary ailment. Thus, deaths from other causes like heart failure have been improperly coded as Covid deaths under the CDC’s guidelines. Even tragedies like auto fatalities have been coded as Covid deaths.
At the same time, some public health “elites” insist that many Covid deaths in the community have gone unreported. That might have been true in the early weeks of the pandemic. However, post-mortem testing by medical examiners began to spread by April 2020, though there was a shortage of tests, and the CDC issued guidelines to encourage it late in the year.
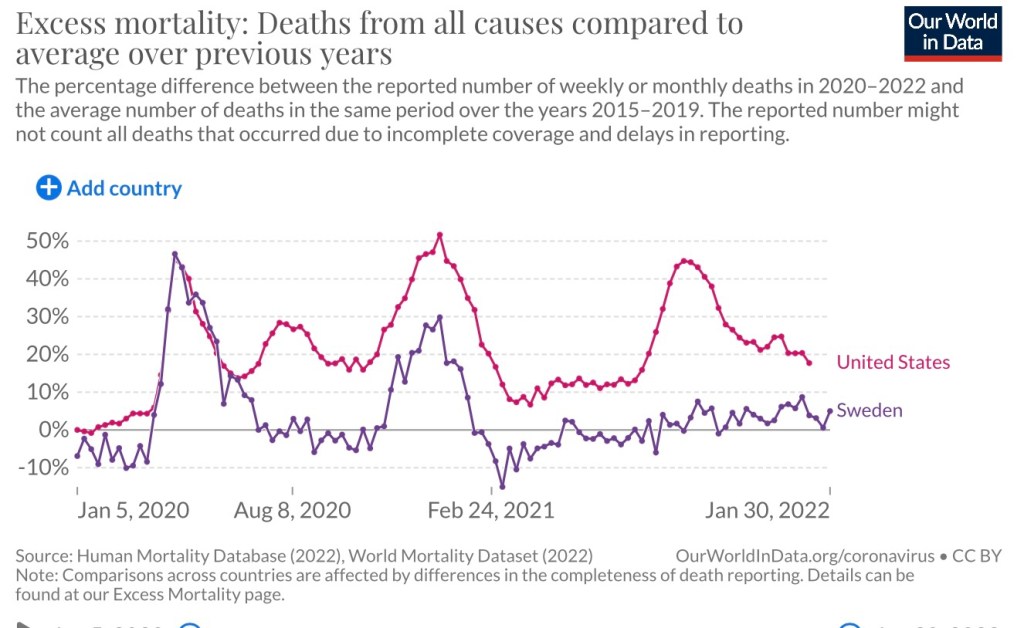
Counting excess deaths from all causes avoids these controversies, including differences across countries in the way they record Covid deaths. It’s also possible to break down excess death into broad categories of causes, though the task is complex.
How Many?
First some simple accounting. Let’s define all-cause mortality during a period (Mort) as Covid deaths (C) plus plus all other mortality (M), or Mort = C + M. Expected mortality in the absence of a pandemic would be Exp(Mort) = Exp(M). Usually this expected value is taken as an average of deaths over several previous years. Therefore, excess mortality during the pandemic is:
EM = C + M – Exp(M)
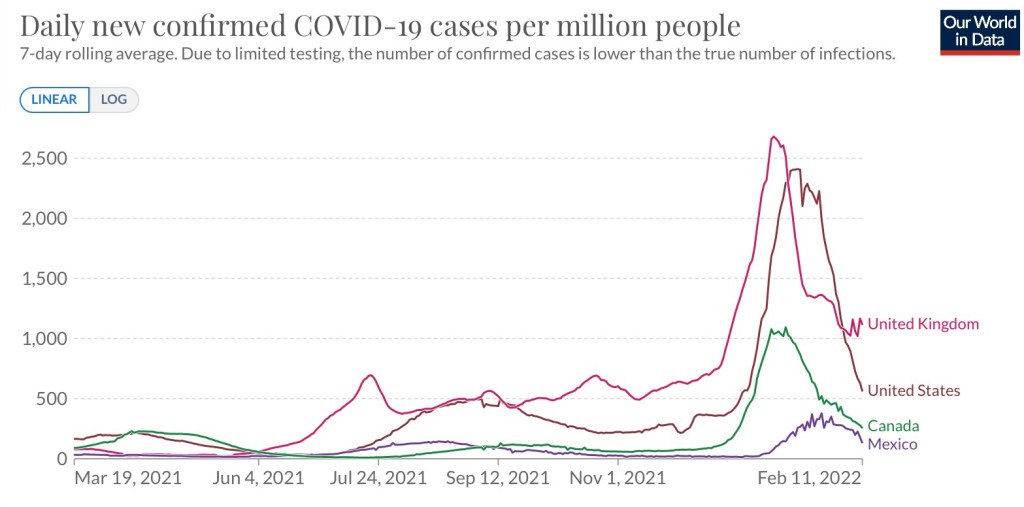
How many excess deaths have we actually seen during the pandemic? According to Our World In Data, the figure was 950,000 as of Jan 9th. USMortality.com puts the excess at about 965,000 through the end of 2021. So these two sources are in close agreement, which says a lot given the usual difficulty of getting pandemic numbers to tie-out across sources
Through 2021, cumulative Covid deaths (by date of death) were almost 850,000. That’s less than excess deaths, so it’s obvious that other factors have contributed to the excess. Interestingly, 2021 was worse for excess deaths than 2020 for all age groups except 85+. Some have suggested the most vulnerable in this highly vulnerable age group had already succumbed to Covid in 2020, but there may have been other reasons for the difference.
Non-Covid Excesses
As noted above, some of the Covid deaths were misattributions. If we understand C to include only deaths “from Covid”, then we must acknowledge that M includes deaths from other causes but “with Covid”, as well as all deaths without Covid diagnoses. For example, because of the confounded way in which Covid deaths have been counted, a death from heart disease could end up in the official count of C, but it should be included in M instead.
The figures above imply 100,000+ excess deaths during the pandemic not associated with Covid diagnoses. If we add to those the “with Covid”, incidental total, then perhaps 300,000 – 400,000 excess deaths during the pandemic were from non-Covid primary causes!
Lockdown effects are a prime suspect in these non-Covid deaths. For example, if health care was deferred because hospitals cancelled or delayed elective procedures, or because patients feared the hospital environment, that would certainly manifest in premature deaths. Deaths of despair or neglect were also in excess, as one should expect when populations are subjected to prolonged periods of isolation.
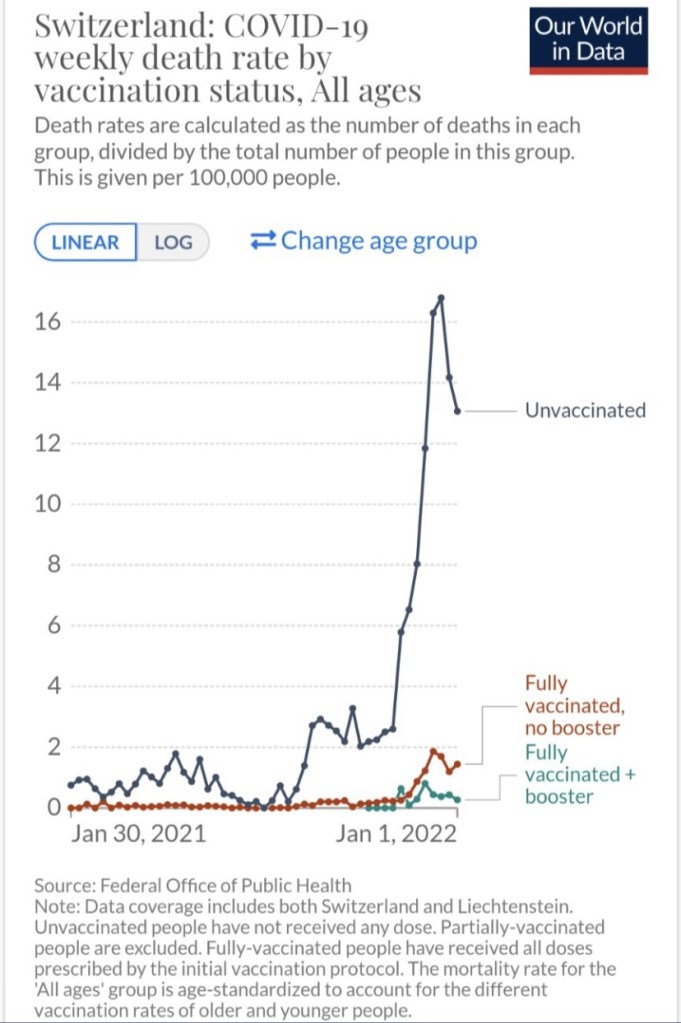
These kinds of deaths are so-called “lockdown” deaths because they could have been avoided without such stringent policy measures and the propagation of fear by public health authorities. Those who might protest this nomenclature should note that lockdowns have been unsuccessful in mitigating the pandemic (and see here). After all, in terms of excess deaths, the Swiss approach was quite successful!
Avoidable Deaths
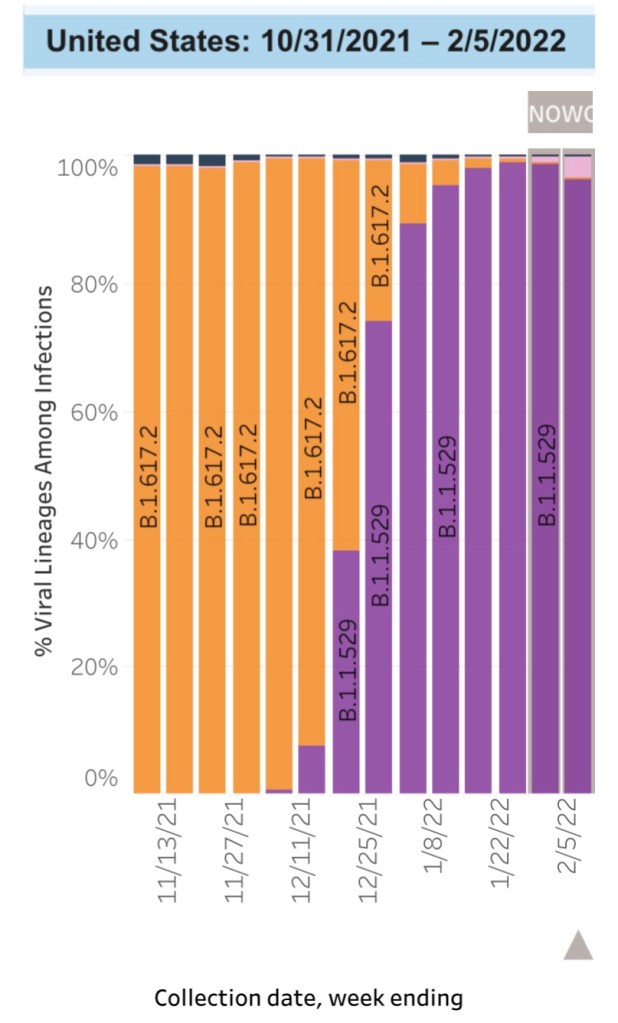
Many of the excess pandemic deaths were avoidable. Prolonged lockdown policies were driven by politics rather than sound public health reasoning. However, within the Covid death totals there is another category of avoidable deaths, and it is every bit as controversial. This post from The Ethical Skeptic (TES) goes into great detail on the matter. He takes a strong position, and some of his assertions and his accounting are subject to challenge. I sometimes find that TES’s posts contain ambiguities, and the graphical evidence he presents is often poorly labeled. Still, he has proven correct on other controversial issues, such as the ancestry and surprisingly early “vintage” of the Omicron variant.
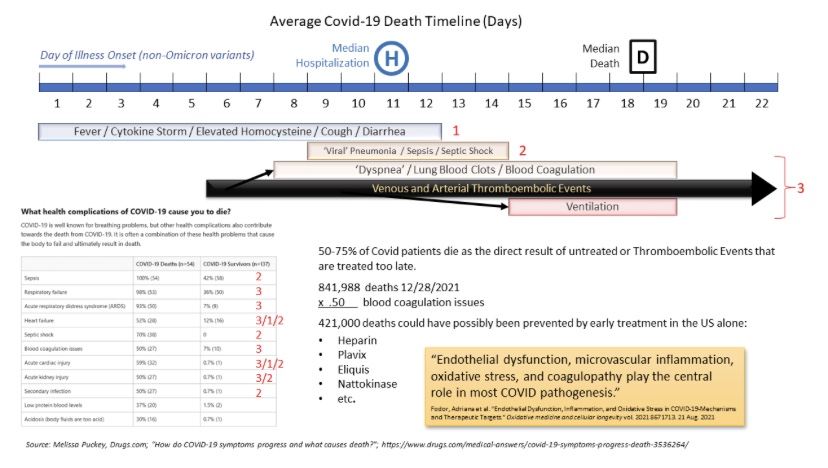
Most of the “avoidable” Covid deaths (again, as distinct from the non-Covid lockdown deaths) occurred well after the primary symptoms of the infection (fever, cough, and cytokine storm) had passed. In the end, the real killers were follow-on problems induced by Covid, primarily related to blood clotting and compromised vascular integrity from endothelial dysfunction. These deadly complications were known very early in the pandemic. The following schematic from TES shows a Covid “death timeline”. The figures listed under the schematic show the large share of clotting and vascular problems involved in these deaths.
Over the past two years, not all of these patients were placed on anticoagulants or blood thinners early in the course of their infections. Indeed, many of them were told to “go home and sleep it off”. This is what happened to TES as well as a number of commenters on his Twitter account. I know several individuals who received the same advice from medical professionals. Even among the hospitalized, many were not placed on these drugs in a timely fashion, or until it was too late. TES adds the wrinkle that his physician indicated he should have been vaccinated! Short of that, tough luck, said the healer.
TES blames this medical “malfeasance” on the CDC’s Emergency Use Authorizations (EUA) for the Covid vaccines. In fact, he calls these deaths “EUA Shadow Deaths”, citing legal requirements associated with EUAs that would appear to prohibit alternatives such as therapies and even tests or studies of alternatives. That contention seems questionable given the CDC’s issuance of other EUAs for certain treatments, and there was no shortage of published experiments conducted during 2020-21.
The vaccine EUAs were not issued until late 2020, but TES claims that forces leading up to those EUAs were responsible for the failure to put patients on anticoagulants/blood thinners even earlier in 2020. The schematic says more than half of Covid deaths through the end of 2021 involved blood coagulation issues, and I have no reason to doubt those figures, which TES sources from the CDC. But He uses a value of 50% of Covid deaths to estimate that 421,000 Covid deaths were avoidable.
I’m not sure about that total, or rather, the use of the term “avoidable” in all those cases. I am sure, however, that we’ve seen a remarkable under-emphasis on therapeutics (and see here and here) relative to the emphasis on vaccines. The news media contributed to the dysfunction by condemning certain promising therapies for political reasons.
I’m also sure that there have been a meaningful number of patients who should have received anticoagulants/thinning agents but did not. Why did they not? Plausibly, the restrictions imposed by the vaccine EUAs made a difference, but clearly the medical community was not tuned into what should have been an obvious treatment regimen.
How many Covid deaths were truly avoidable? TES’s estimate of 421,000 seems too high if only because we can’t expect the dissemination of information through the medical community to be perfect. Moreover, some of these patients were undoubtedly on blood thinners already, or there might have been contraindications preventing the use of anticoagulants/thinners.
Nevertheless, a substantial number of deaths could have been avoided by more timely use of therapeutics and less stringent lockdown measures. Here is a chart from a tweet by TES showing another accounting for excess deaths:
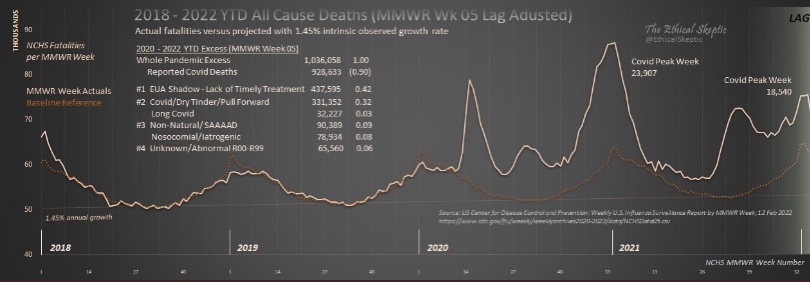
Here, TES uses a slightly longer time frame, through about February 5, 2022, so the “EUA Shadow Death” total is somewhat larger, about 437,000, than shown in the earlier schematic. He attributes about 800,000 excess deaths, or 77%, to Covid, most of which he believes were avoidable deaths.
Lockdown deaths account for some of the additional 236,000 excess deaths reported in the chart, and probably a large share of the roughly 90,000 non-natural deaths labeled #3 (SAAAAD = “Suicide Addiction Abandonment Abuse Accident & Despair”; the two other categories in #3 relate to non-Covid illnesses acquired in-hospital or adverse reactions to medications). The Unknown/Abnormal category may include some lockdown deaths, but more on that category below.
If TES is correct about shadow deaths, the “avoidable” pandemic death total might account for well over half of all excess deaths. I suspect it might account for half, but even if less, it’s clear that avoidable deaths have been a huge part of the pandemic’s toll.
Vaccine Adverse Events
There’s been much speculation about the large number of Unknown/Abnormal deaths that have been coded during the pandemic: more than 65,000 in the chart above. One caveat is that an “unknown” cause of death usually means the cause is ambiguous: there might have been several factors contributing to the death such that the medical examiner was unable to assign a definitive cause. That status can be temporary as well. Still, the surge is noteworthy.
Unfortunately, there were an unusual number of excess deaths in younger age brackets in 2021, especially in the second half of the year after vaccinations had reached a fairly large share of the population. The pace of those deaths hasn’t yet abated in 2022. The next chart, from USMortality.com, shows excess mortality in the 25 – 44 age bracket in 2020 – early 2022.
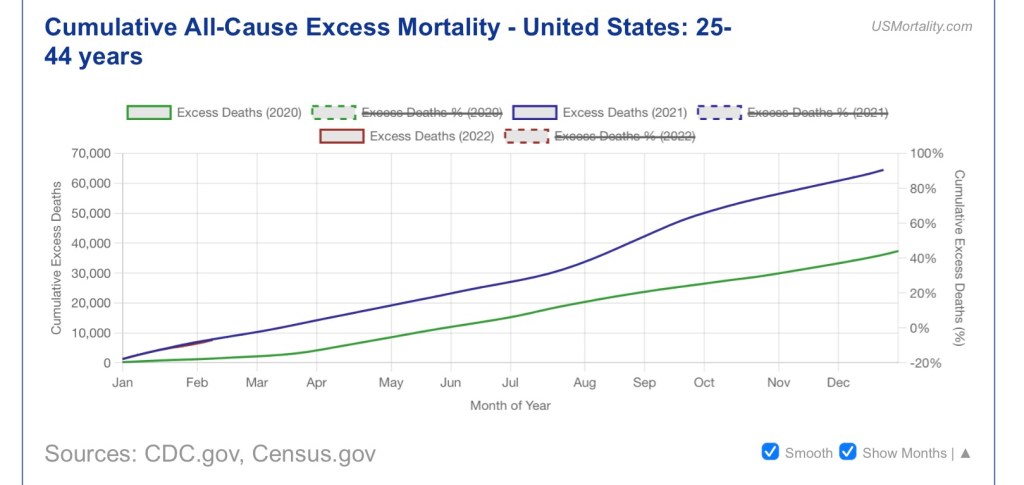
Many of these prime age deaths could be a continuing hangover from deferred medical care and depression. There are claims, however, that the vaccines themselves killed a significant number of individuals. The upsurge in excess deaths suggests to some that the vaccines have had a much greater number of “adverse events” than we’ve seen reported by the CDC and the news media.
Here is how TES presents the data on excess deaths and vaccinations. The chart title is his somewhat confusing attempt to summarize the meaning of the lines plotted. The left axis measures the pace of vaccinations by week and the right access measures weekly excess non-Covid natural-cause deaths.
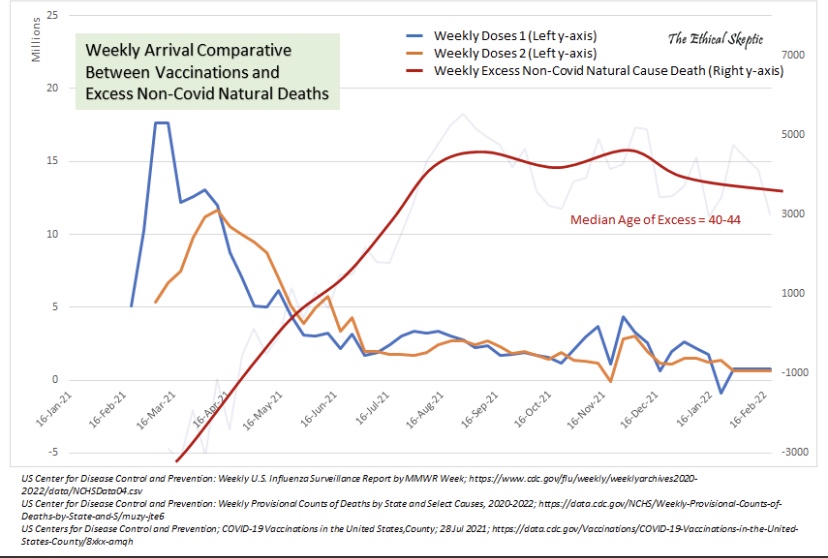
I have no doubt as to the efficacy of the vaccines against serious Covid outcomes in high-risk groups, though vaccine efficacy has been drastically overstated by the Biden Administration. The balance of risks for older individuals is clearly in favor of vaccination. Still, I’ve long felt that vaccination is less compelling for people in younger age brackets, and it’s possibly a bad idea. That’s both because Covid is a much smaller risk to them and because of possible vaccine risks, such as myocarditis.
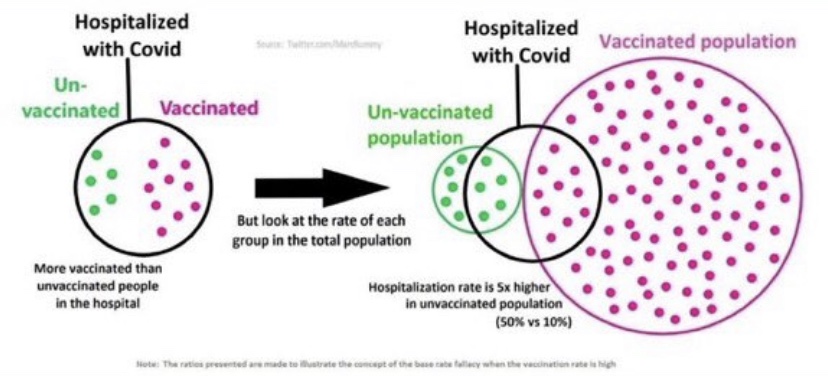
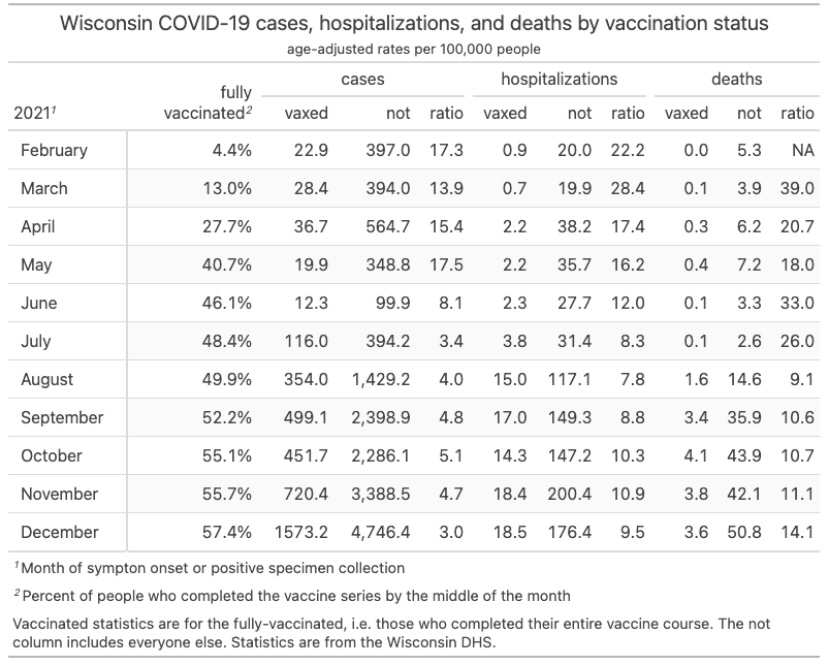
To the extent that natural-cause, non-Covid excess deaths among younger age cohorts have been driven by unnecessary vaccinations, those deaths were avoidable. I’m not convinced of the significance, and it’s clear that among hospitalized Covid patients, outcomes have been better among the vaccinated. The following chart is from the link in the previous paragraph:
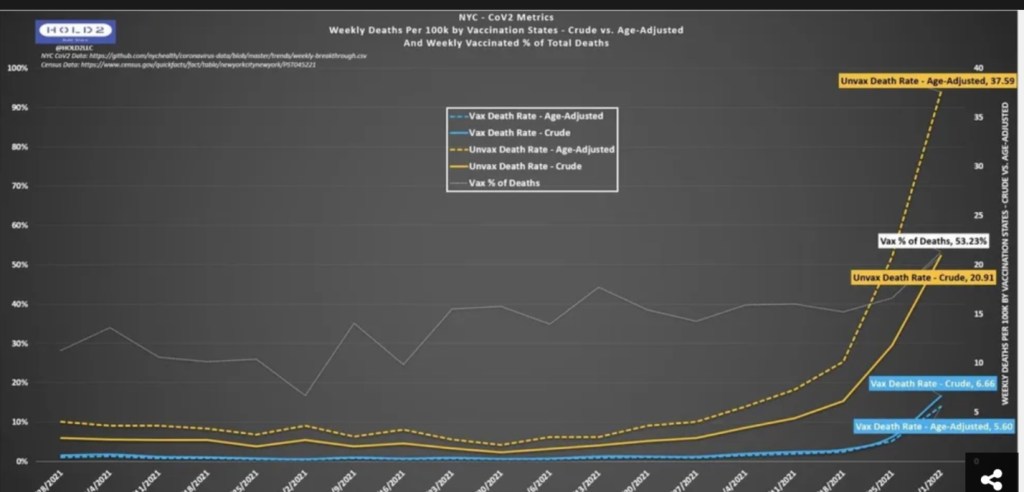
That sort of pattern might mean more deaths among the unvaccinated could have been avoided, on balance, had they opted for the jab. In almost all things, however, I believe we should eschew blanket mandates and instead offer protection to those seeking it in the high-risk population.
Conclusion
As many as 30% of Covid deaths to date are likely misattributions in which Covid was not really the primary cause of death. Nevertheless, excess Covid deaths “from Covid” as the primary cause are probably approaching 700,000 today.
The pandemic was certainly bad enough without a slew of bad calls by the public health and medical establishments. Of the 950,000+ excess deaths that occurred through the end of 2021, over 100,000 were not attributed to Covid. If we include deaths mis-attributed to Covid, the non-Covid total is likely in excess of 300,000 and could be as high as 400,000. It’s time to acknowledge that lockdowns and fear-mongering led to a large number of those deaths, and most of those deaths were avoidable. However, while I am skeptical, the number of deadly adverse effects from vaccines in the prime age population is an open question.
Another class of avoidable deaths was a product of the underemphasis on Covid therapies by the medical establishment. There were many cases of promising, repurposed drugs that were shouted down after so-called experts insisted that their use must be withheld until adequate randomized control trials (RCTs) had confirmed their efficacy. Not only did this ignore the long history of clinical evidence as a guide to medical practice. It also ignored the frequent real-world inadequacies that plague RCTs.
At the same time, obvious complications of the vascular system, primarily blood clotting, were not treated in a timely way or as a precautionary treatment’s, at least prior to hospitalization. Adding a conservative allowance for these deaths to the other avoidable deaths probably means that at least half of the excess deaths during the pandemic were avoidable. As of March 2022, that’s over half a million deaths! We can chalk it up to mismanagement and miscommunication by the public health establishment with a dash of ignorance, and perhaps some malfeasance, by health care practitioners. The death of expertise, indeed!