Tags
Acquired Immunity, Biden Administration, CDC, Child Risks, Covid-19, Covid-Like Symptoms, Covidestim.org, Delta Variant, EU Visits, HOLD2, Hope-Simpson Seasonal Pattern, Hospital Utilization, Hospitalizations, Incidental Infections, John Tierney, Lockdowns, Mask Efficacy, Natural Immunity, Omicron BA.1, Omicron BA.2, Omicron Variant, Our World In Data, Phil Kerpen, Staffed Beds, Teachers Unions, Tradeoffs, Transmissability, Vaccine Efficacy, Vaccine Risks, Virulence
We might be just be done with the coronavirus pandemic. That is, it appears to be transitioning to a more permanent endemic phase. What follows are a few details about the Omicron wave and its current status, an attempt to put the risks of Covid in perspective, and a few public policy lessons that are now gaining broad currency but should have been obvious long ago.
What’s The Status?
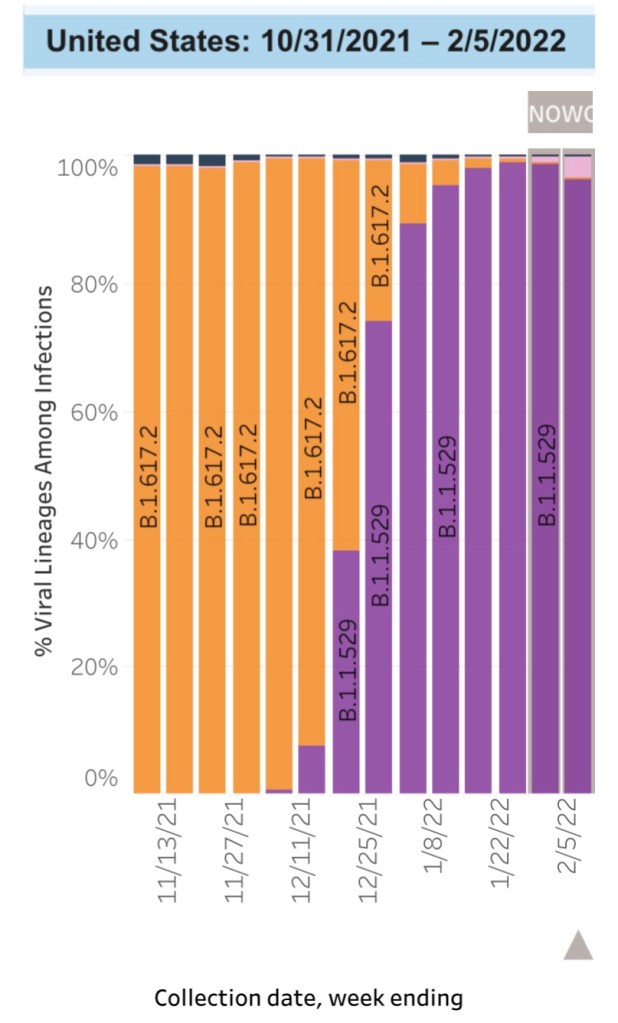
The Omicron variant became the dominant U.S. strain of the coronavirus in December. Omicron outcompeted Delta, which was very good news because Omicron is far less severe. The chart below (from the CDC Data Tracker site) shows Omicron’s rapid ascendance and displacement of the Delta variant. The orange bar segments represent the proportion of cases of the Delta strain, while the purple and pink segments are Omicron sub-variants known as BA.1 and BA.2, respectively. BA.2 is even more transmissible than BA.1 and is likely to become dominant over the next month or so. However, the BA.2 sub-variant appears to be far less virulent than Delta, like BA.1.
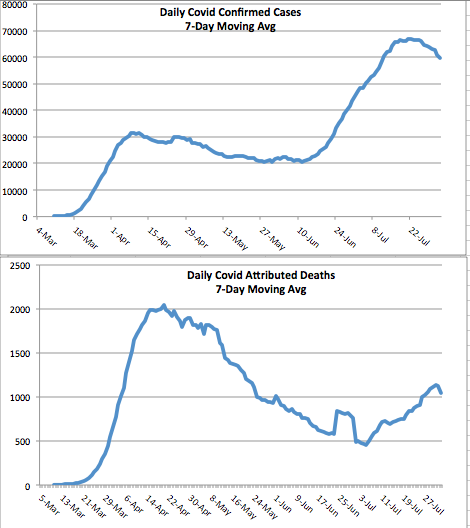
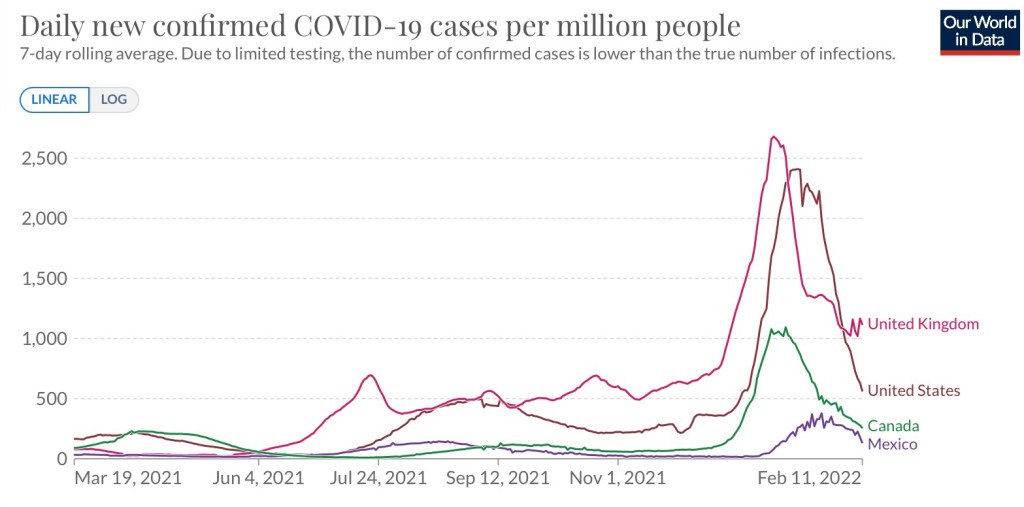
Despite a record number of infections over a period of a month or so, the Omicron wave is tapering just as rapidly as it ramped up, as the next chart demonstrates. In fact, covidestim.org shows that cases are now receding in all states, DC, and Puerto Rico. Here are new cases per million people from Our World in Data:
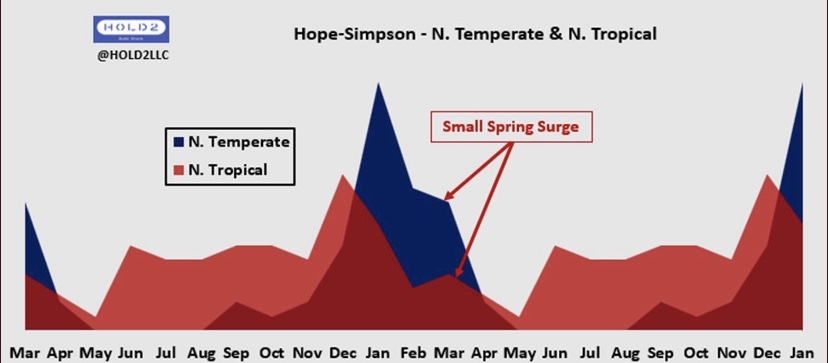
Whether BA.2 causes cases to plateau for a while, or even a secondary Omicron “wavelet”, is yet to be seen. That would be consistent with the normal Hope-Simpson seasonal pattern of viral prevalence in the northern hemisphere (hat tip: HOLD2):
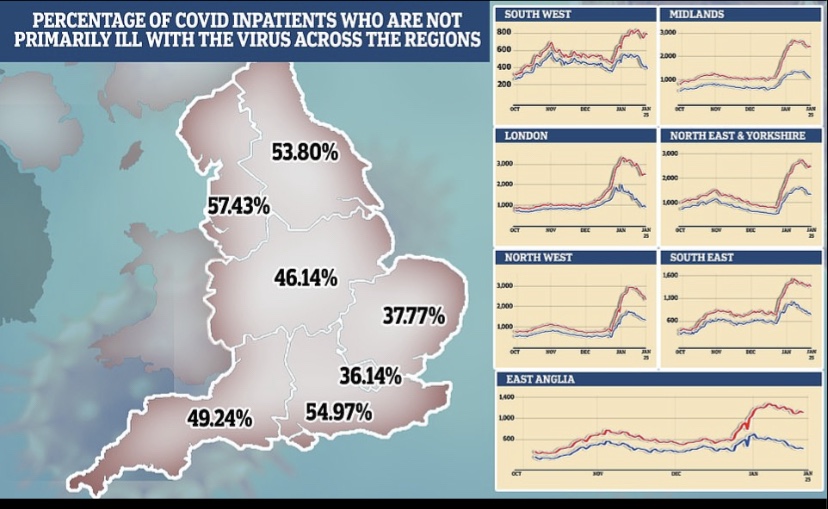
Data problems make the Omicron wave difficult to assess, however. We don’t know the share of incidental infections for the U.S. as a whole, but more than half of hospitalized Covid patients in Massachusetts and Rhode Island are classified with incidental infections. The proportion in the UK is estimated to be rising and approaching 30% of total cases, with much higher percentages in many regions of England, as shown below.
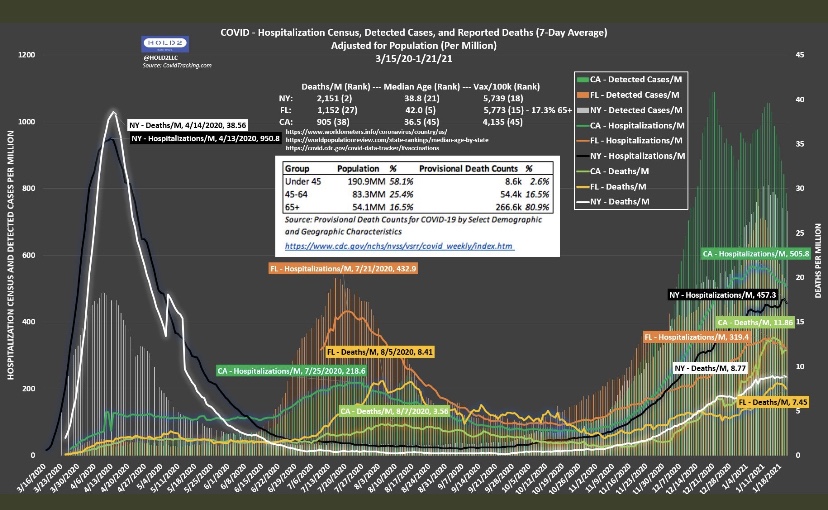
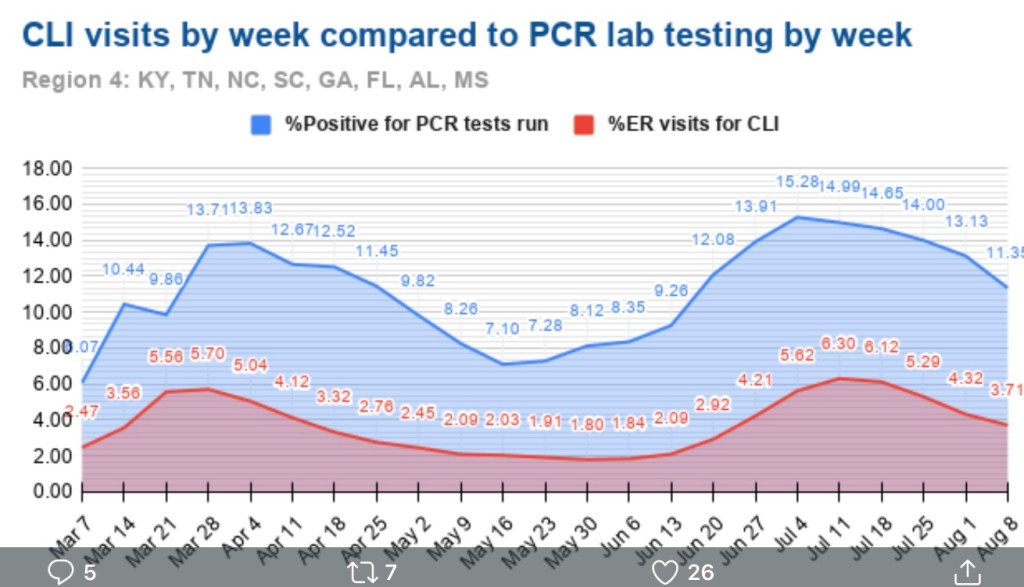
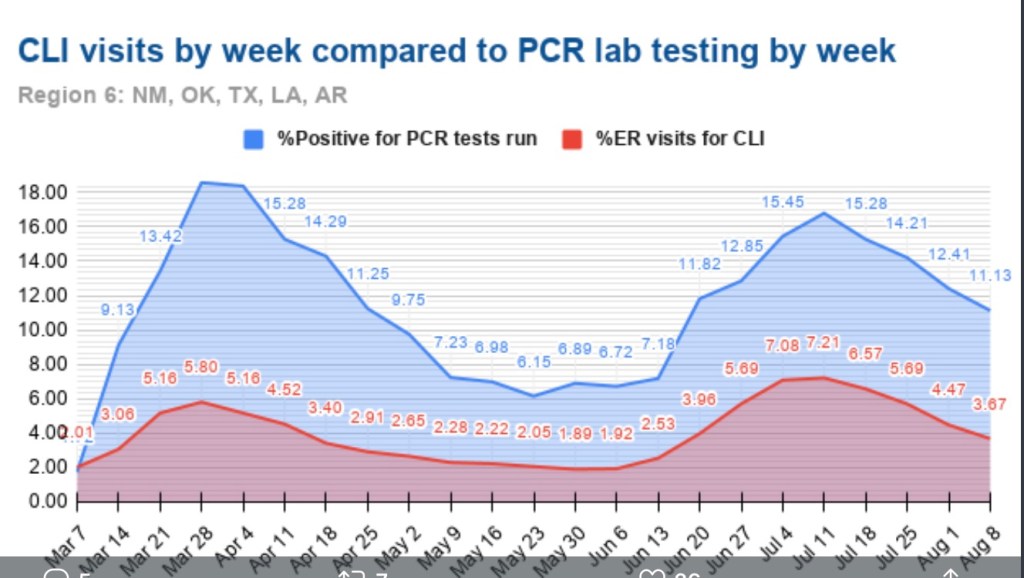
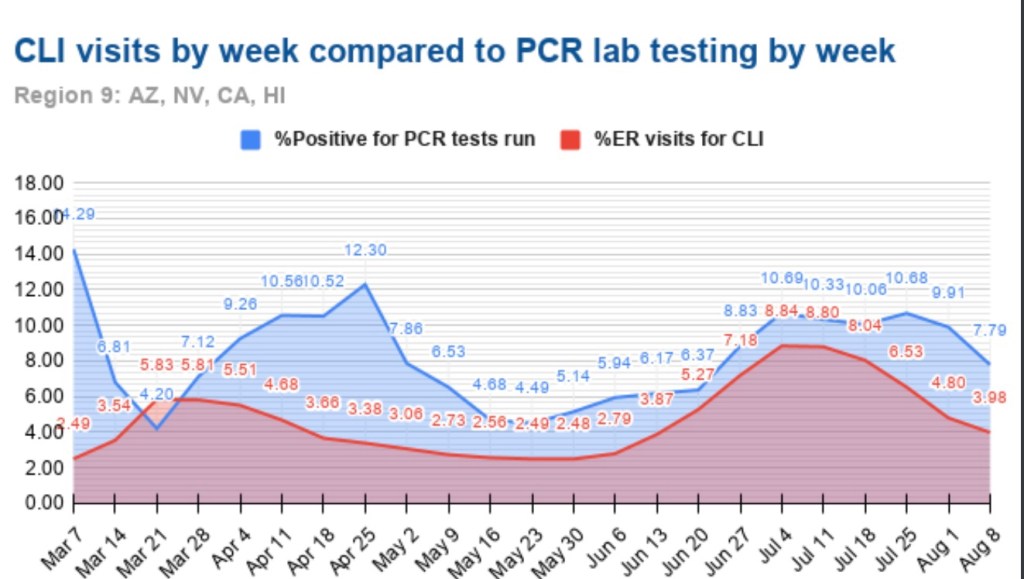
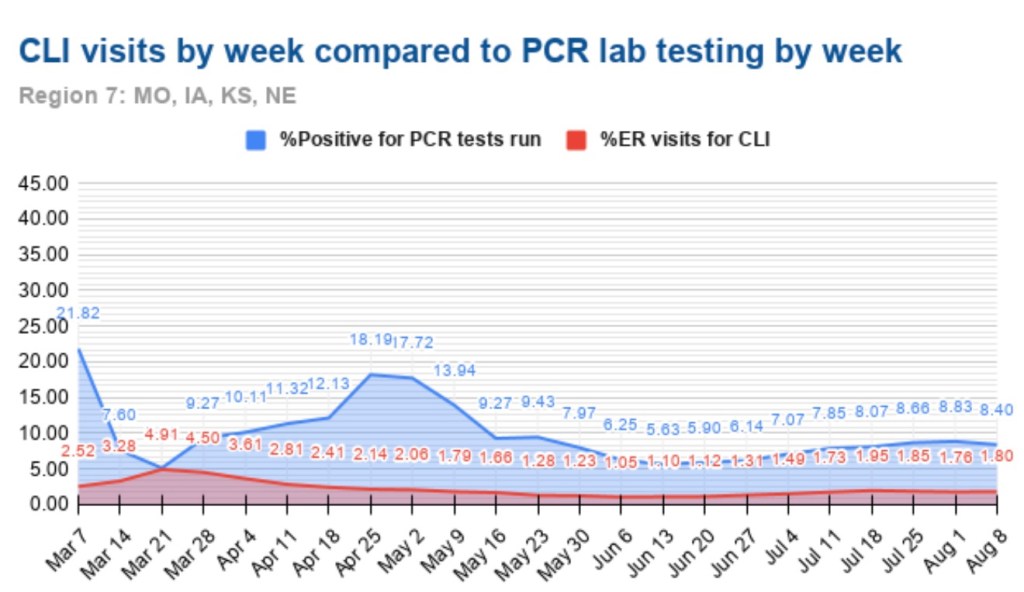
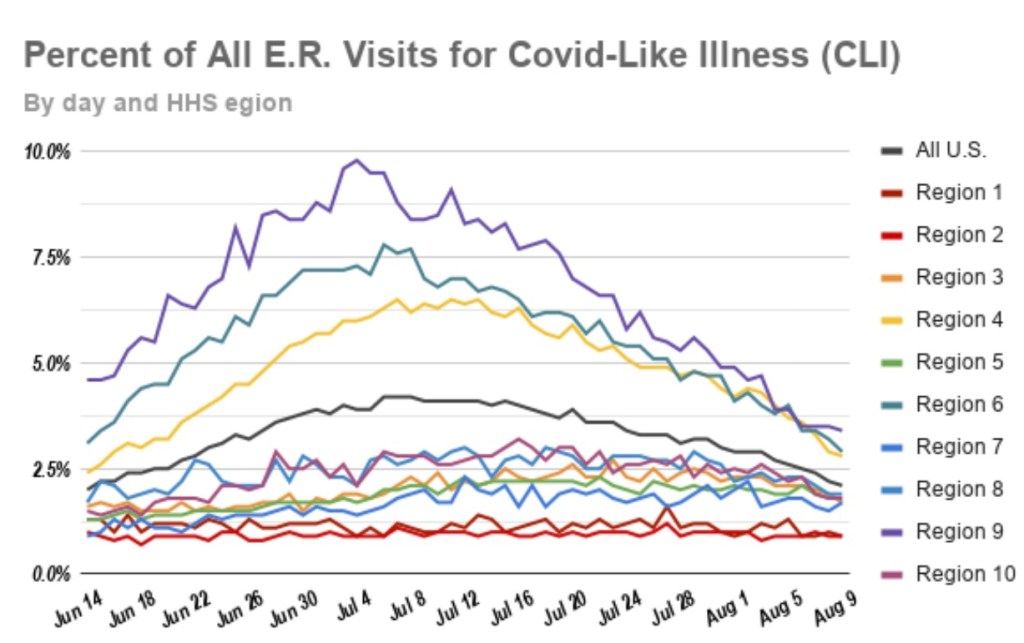
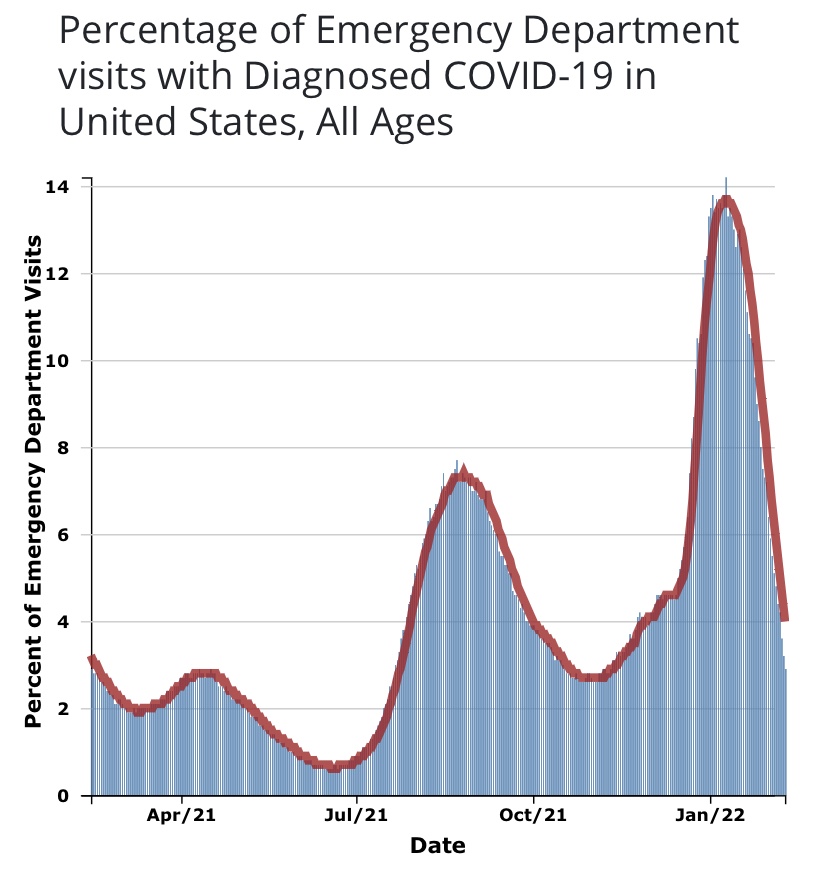
As I’ve emphasized in the past, case numbers should not be the primary gauge of the state of the pandemic, especially with a more highly contagious but relatively mild variant like Omicron. Hospitalizations are a better measure, but only if “incidental” infections are removed from the counts. That’s been acknowledged only recently by the public health establishment, and even the Biden Administration is emphasizing it as a matter of sheer political expediency. Another measure that might be more reliable for assessing the pandemic in the community as a whole is the number of emergency room patients presenting Covid-like symptoms. From the CDC Data Tracker:
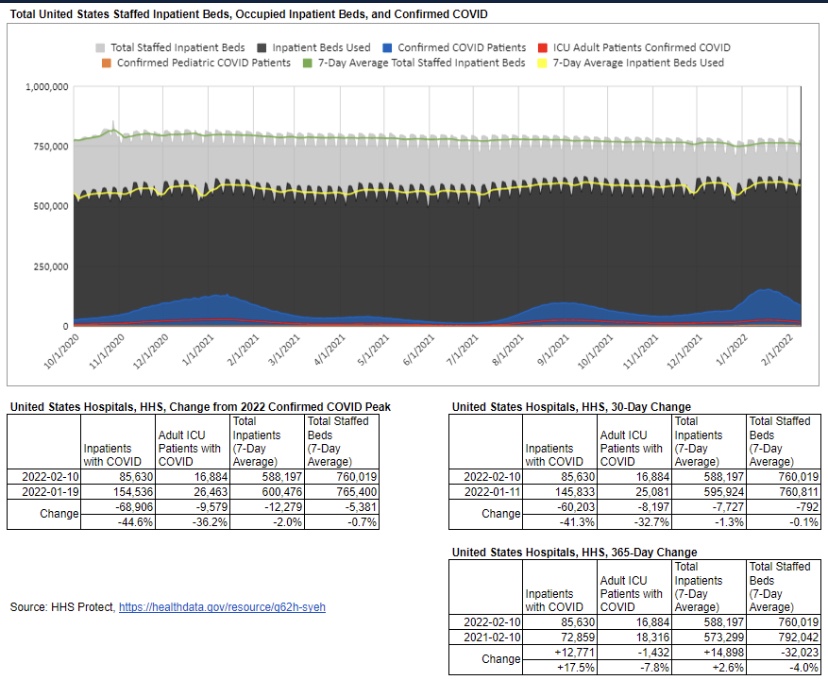
There is no doubt that incidental infections create complications in caring for patients with other ailments. That has a bearing on the utilization of hospital capacity. Generally, however, strains on hospital capacity during the pandemic have been greatly exaggerated. This is not to diminish the hard work and risks faced by health care workers, and there have been spot shortages of capacity in certain localities. However, in general, staffed beds have been more than adequate to meet needs. This chart, like a few others below, is courtesy of Phil Kerpen:
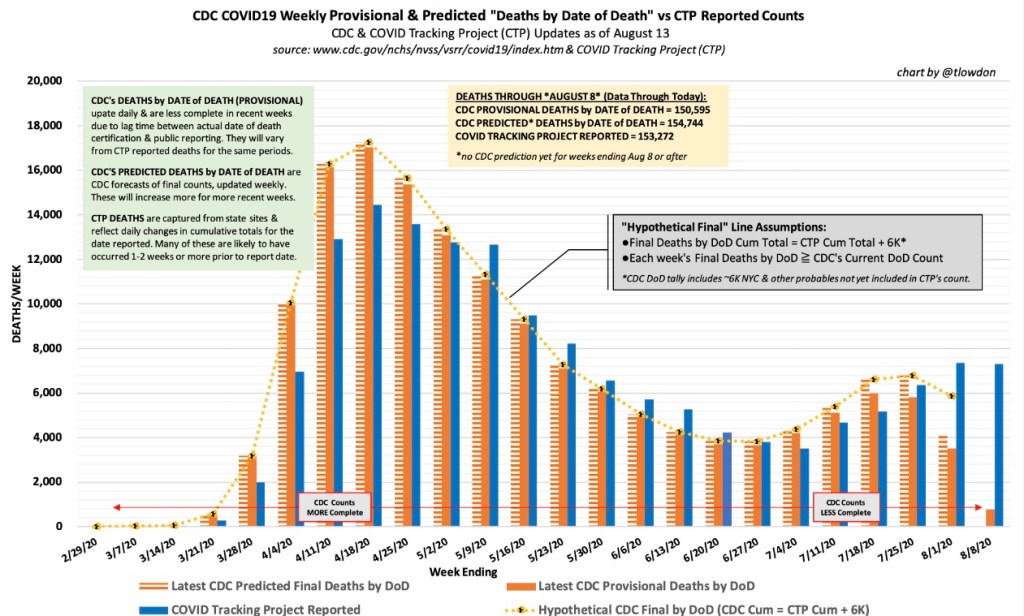
With the more highly transmissible variants we have now, it’s not at all surprising to see a high proportion of incidental cases among inpatients. Incidental infections are likely to inflate counts of Covid deaths as well, given the exceptional and odd way in which Covid deaths are being recorded. It will be some time until we see full U.S. data on cases and deaths net of incidental infections. Moreover, many of the Covid deaths in December and January were from lingering Delta infections, which might still be a factor in the February counts.
How Are Your Odds?
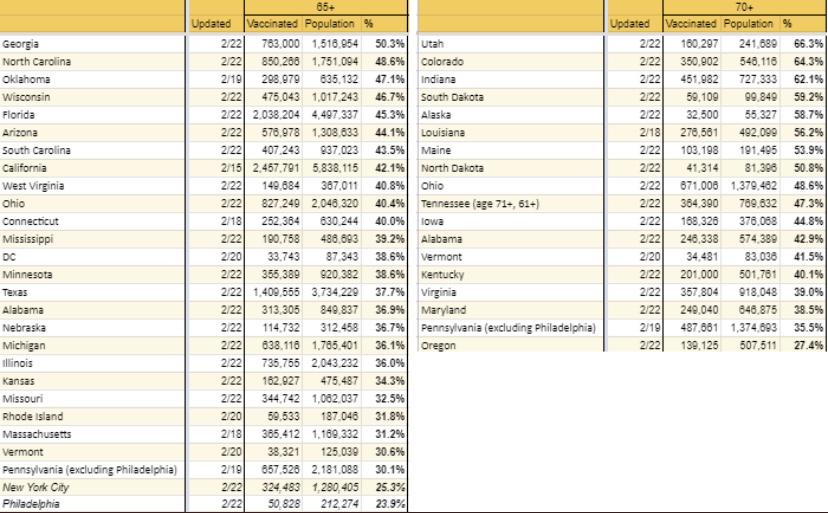
The mild or asymptomatic nature of most Omicron cases, the large proportion of incidental hospitalizations, and the knowledge that Omicron is not a deep respiratory threat should offer strong reassurance to healthy individuals that the variant does not pose a great risk. According to a recent CDC report, in a sample of almost 700,000 vaccinated individuals aged 65 or less without co-morbidities, there were no Covid fatalities or ICU admissions during the 10 months from December 2020 through October 2021. There was only one fatality in the sample of healthy individuals older than 65. There were just 36 fatalities across the full sample of over 1.2 million vaccinated individuals, so COVID’s fatality risk was only about 0.3%. Of those deaths, 28 were among those with four or more risk factors (including co-morbidities and > 65 years). And this was before the advent of Omicron!
I have a few doubts about the CDC’s sample selection and vagaries around certain definitions used. Nevertheless, the results are striking. However, the study did not address risks to unvaccinated adults. Another more limited CDC study found that vaccinated patients were still less likely than the unvaccinated to require critical care during the Omicron wave.
A separate CDC study found a 91% reduction in the likelihood of death for Omicron relative to Delta. A study from the UK (see summary here) found that Omicron cases were 59% less likely than Delta cases to require hospitalization and 69% less likely to result in death within 28 days of a positive test. Omicron was far less deadly among both the vaccinated and the unvaccinated, and the latter had a larger reduction in the likelihood of death. The study was stratified by age as well, with less severe outcomes for Omicron among older cohorts except in the case of death, for which there was no apparent age gradient.
Another unnecessarily contentious issue has been the risk to children during the pandemic. Based on the data, there should never have been much doubt that these risks are quite low. Apparently, however, it was advantageous for teachers’ unions to insist otherwise. Phil Kerpen soundly debunks that claim with the following chart:
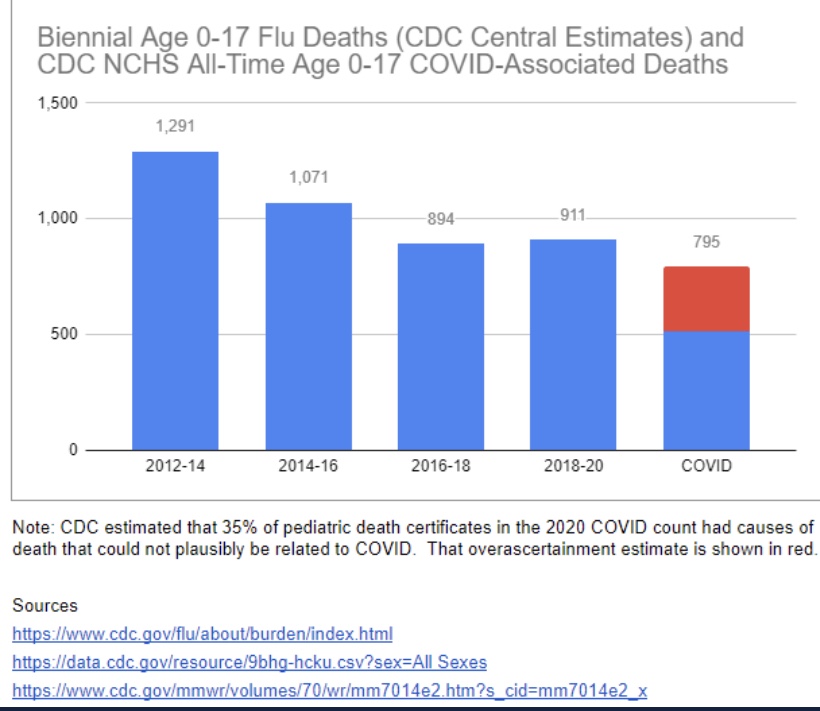
Covid has been less deadly to children from infancy through 17 years than the pre-pandemic flu going back to 2012! Oh yes, but teachers FEAR transmission from the children! That claim is just as silly, since children are known to be inefficient transmitters of the virus (and see here).
Now that Omicron has relegated the Delta variant to the history books, the risks going forward seem much more manageable. Omicron is less severe, especially for the vaccinated. Levels of acquired (natural) immunity from earlier infections are now much higher against older strains, and Omicron infections seem to be protective against Delta.
In commentary about the first CDC study discussed above, John Tierney lends perspective to the odds of death from pre-Omicron Covid:
“Those are roughly the same odds that in the course of a year you will die in a fire, or that you’ll perish by falling down stairs. Going anywhere near automobiles is a bigger risk: you’re three times more likely during a given year to be killed while riding in a car, and also three times more likely to be a pedestrian casualty. The 150,000-to-1 odds of a Covid death are even longer than the odds over your lifetime of dying in an earthquake or being killed by lightning.”
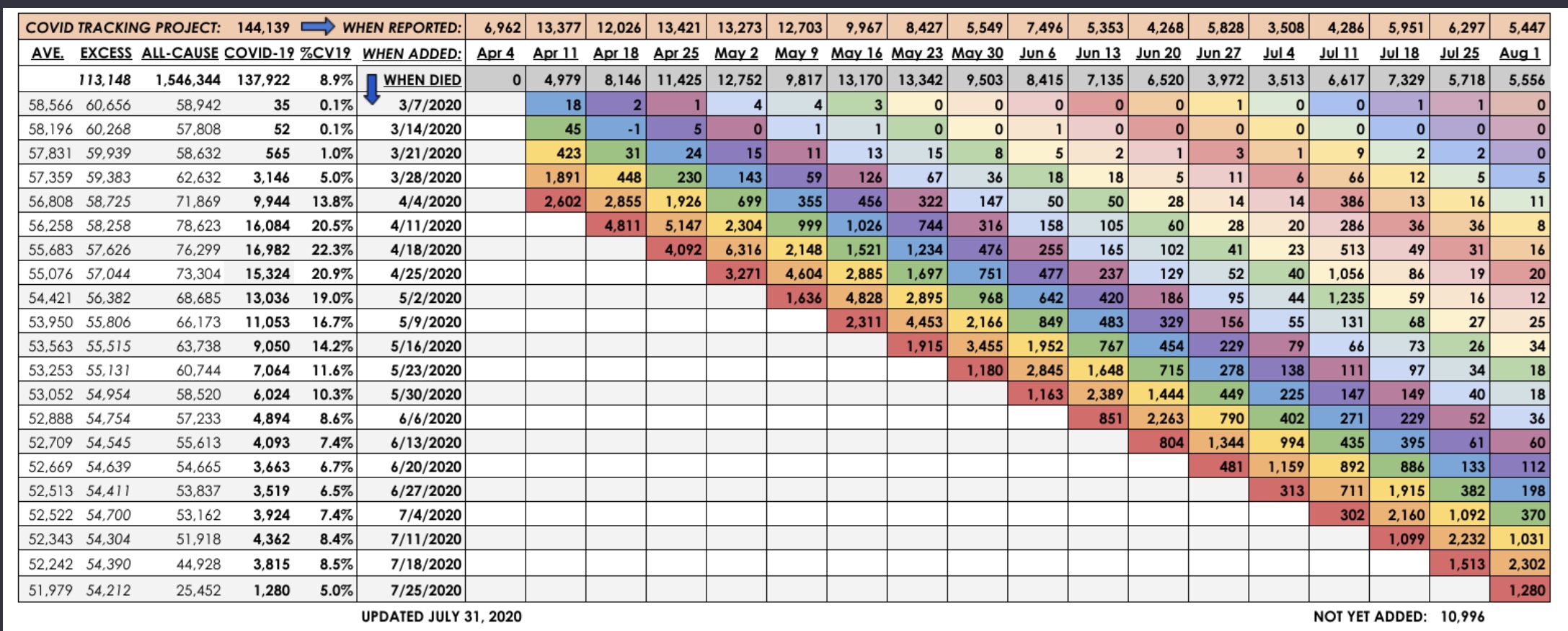
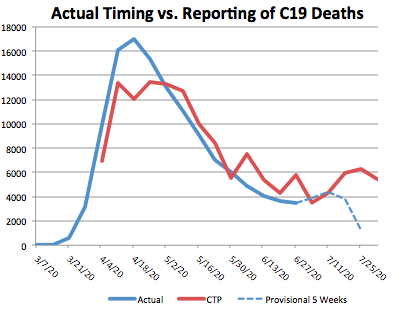
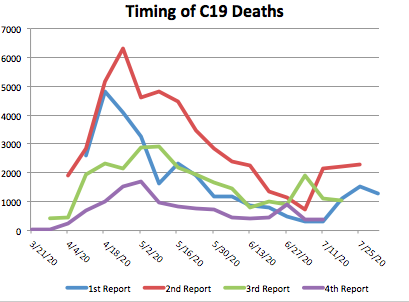
Yet with all this research confirming the low odds of death induced by Omicron, why have we seen recent deaths at levels approaching previous waves? First, many of those deaths are carried over from Delta infections. That means deaths should begin to taper rapidly as February reports roll in. And remember that daily reports do not show deaths by date of death. Deaths usually occur weeks or even months before they are reported. That also means some of the deaths reported might be “harvested” from much earlier fatalities. Second, given the high levels of incidental Omicron infections, some of those deaths are misattributed to Covid, an issue that is not new by any means. Finally, while Omicron is relatively mild for most people, the high rate of transmission means that a high number of especially vulnerable individuals may be infected with severe outcomes. We have seen much more severe consequences for the unvaccinated, of course, and for those with co-morbidities.
Things We Should Have Known
I’ll try to keep this last section brief, but as an introduction I’ll just say that it’s almost as if we’ve been allowing the lunatics to run the asylum. To paraphrase one comment I saw recently, if you wonder why there is so much dissent, you ought to consider the fact the much of what our governments have done (along with many private organizations) was to prohibit things that were demonstrably safe (e.g., going outside, using swing sets, or attending schools) and to encourage things that were demonstrably harmful (e.g., deferring medical care, or masking small children).
The following facts are only now coming into focus among those who’ve been “following the politics” rather than “the science”, despite pretensions to the latter.
- Specific public health initiatives often face steep economic, emotional, social, and countervailing health tradeoffs.
- Lockdowns do NOT work.
- Masks do NOT work (despite the CDC’s past and recent confusion on the matter).
- Children are at very low-risk from Covid.
- Children do NOT present high risks to teachers.
- Natural immunity is more protective than vaccines.
- Vaccines do NOT “stop the spread”.
- Vaccine risks might outweigh benefits for certain groups and individuals.
- Vaccines should NOT be relied upon at the expense of treatments.
- Don’t reject treatments based on politics.
- Vaccine mandates are unethical.
Grow Up and Chill Out!
Life is full of risks, and nothing has changed to alter wisdom gained in earlier pandemics. For example, this pearl from a 2006 publication on disease mitigation measures should be heeded (hat tip: Phil Kerpen):
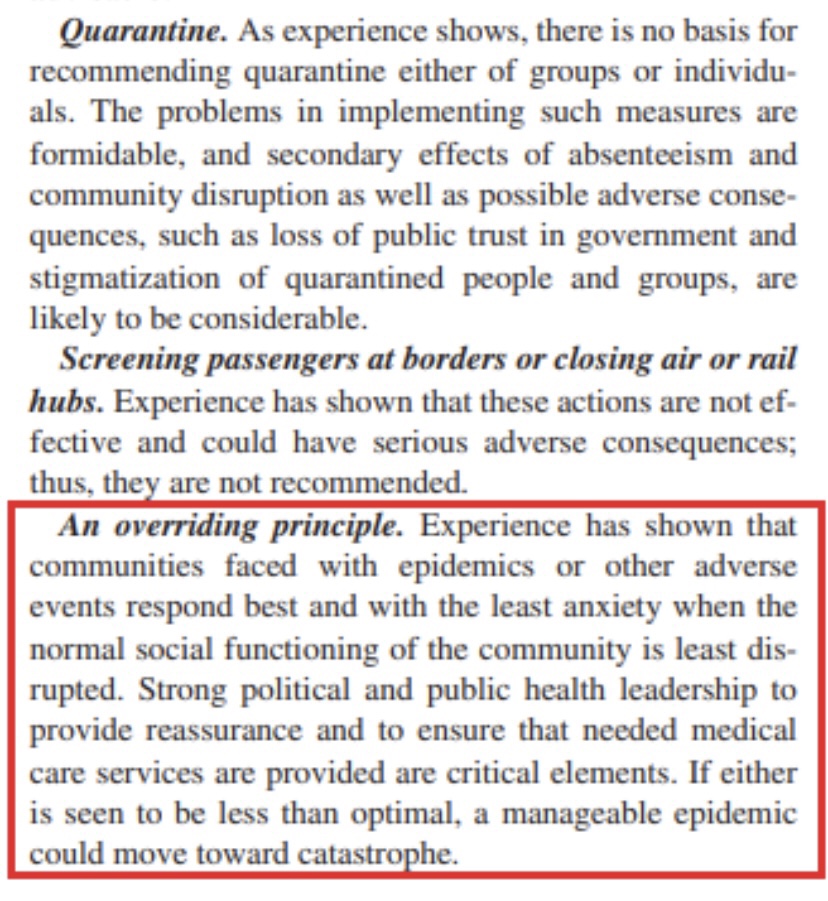
If there is one simple message everyone needs to hear, it is to stop allowing the virus bogeyman to rule your life. It will never go away completely, and it is likely to present risks that is are comparable to the flu going forward. In fact, it might well compete with the flu, which means we won’t be dealing with endemic Covid plus historical flu averages, but some smaller union of the two case loads.
So get out, go back to work, or go have some fun! Get back truckin’ on!