
Tags
Biden Administration, Causality, CDC, COVID Relief Bill, Covid-19, Dining Restrictions, Hope-Simpson, Karl Dierenbach, Lockdowns, Mask Mandates, Masks, Non-Pharmaceutical interventions, NPIs, Seasonality, Spurious Correlation, Vaccinations, Zero COVID

The CDC’s new study on dining out and mask mandates is a sham. On its face, the effects reported are small. And while it’s true most of the reported effects are statistically significant, the CDC acknowledges a number of factors that might well have confounded the results. This study should remind us of the infinite number of spurious and “significant” correlations in the world. Here, the timing of the mandates (or their removal) relative to purported effects and seasonal waves is highly suspicious, and as always, attributing causality on the basis of correlation is problematic.
On one hand, the CDC’s results are contrary to plentiful evidence that mandates are ineffective; on the other hand, the results are contrary to earlier CDC “guidance” that masks and limits on indoor dining are “highly effective”. Nevertheless, the latest report has massive propaganda value to the CDC. The media lapped up the story and provided cover for Democrats eager to pass the COVID (C19) relief package. Likewise, the Biden Administration is apparently committed to the narrative of an ongoing crisis as cover for continued attempts to shame political opponents in states that have elected to “reopen” or remain open.
Right off the bat, the study’s authors assert that the primary mode of transmission of C19 is from respiratory droplets. This is false. We know that aerosols are the main culprit in transmission, against which cloth masks are largely ineffective.
Be that as it may, let’s first consider the findings on dining. There was no statistically significant effect on the growth rate of cases or deaths up to 40 days after restrictions were lifted, according to the report. In fact, case growth declined slightly. There was, however, a small but statistically significant increase after 40 days. The fact that deaths seemed to “respond” faster and with greater magnitude than cases makes no sense and suggests that the results might be spurious.
The CDC offers possible explanations the long delay in the purported impact, such as the time required by restaurants to resume operations and early caution on the part of diners. These are speculative, of course. More pertinent is the fact that the data did not distinguish between indoor and outdoor dining, nor did it account for other differences in regulation such as rules on physical distancing, intra-county variation in local government mandates, and compliance levels.
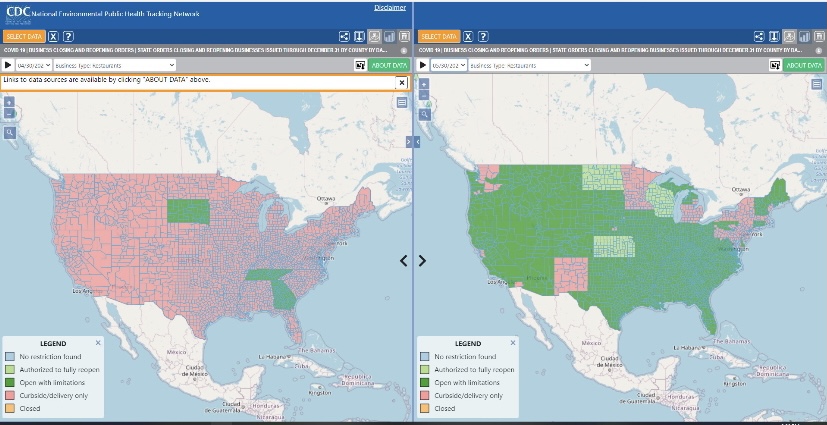
Finally, the measurement of effects covered 100 days after the policy change, but this window spans different stages of the pandemic. There were three waves of infections during 2020, which correspond to the classic Hope-Simpson pattern of virus seasonality. One was near year-end, but as each of the first two waves tapered (April-May, August-September), it should be no surprise that many restrictions were lifted. Within two months, however, new waves had begun. Karl Dierenbach notes that most of the reopenings occurred in May. Here’s how he explains the pattern:
“The map on the left shows counties where there was no on-premises dining (pink) in restaurants as of the beginning of May (4/30). … The map on the right shows that by the end of May, almost the entire country moved to allow some on-premises dining (green).”
“In the 100 days after May 1, cases nationwide fell slightly, then began to rise, and then plateaued.”
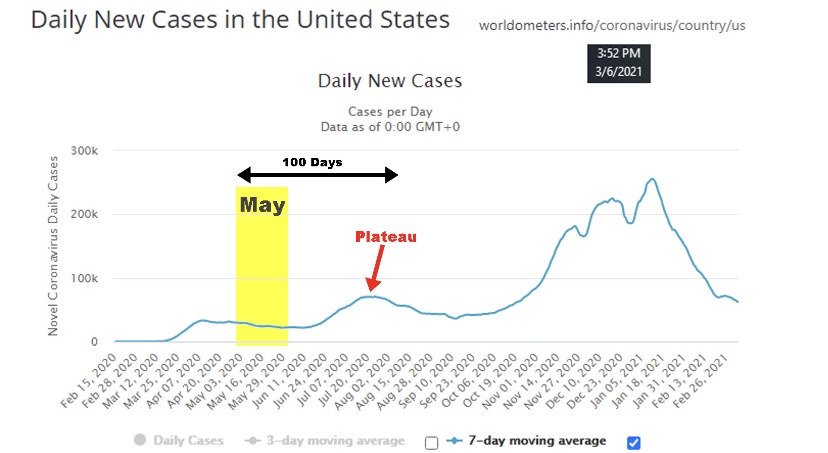
“And what did the CDC find happened after restaurants were allowed (changing mostly in May) to have on-premises dining? … Surprise! The CDC found that cases fell slightly, then began to rise, and then plateaued.”
The summer “mini-wave” is typical of mid- and tropical-latitude seasonality. Thus, the CDC’s findings with respect to dining restrictions are likely an artifact of the strong seasonality of the virus, rather than having anything to do with the lifting of restrictions between waves.
What about the imposition of mask mandates? The CDC’s findings show a much faster response in this case, with statistically significant changes in growth during the first 20 days. Another indicator of spurious correlation is that the growth response of deaths did not lag that of cases, but in fact deaths have reliably lagged cases by over 18 days during the pandemic. Again, the CDC’s caveats apply equally to its findings on masks. A large share of individuals adopted mask use voluntarily before mandates were imposed, so it’s not even clear that the mandates contributed much to the practice.
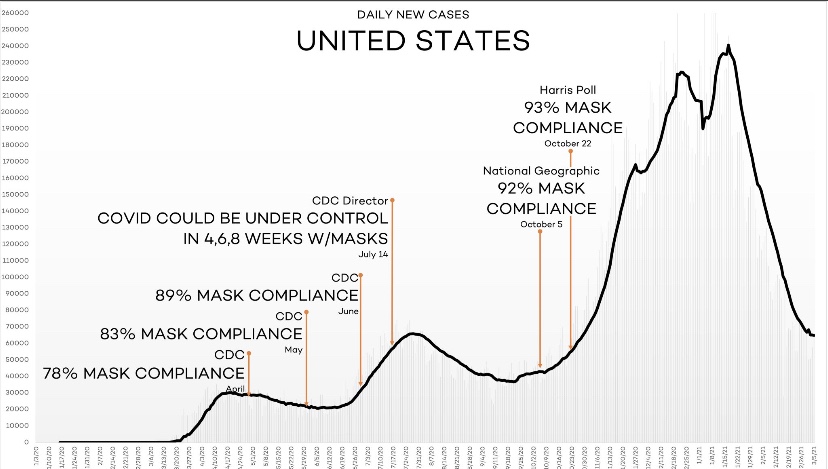
It’s a stretch to believe that mask mandates would have had an immediate, incremental effect on the growth of cases and deaths, given probable lags in compliance, exposure, and onset of symptoms. Moreover, a number of mask mandates in 2020 were imposed near the very peak of the seasonal waves. Little wonder that the growth rates of cases and deaths declined shortly thereafter.
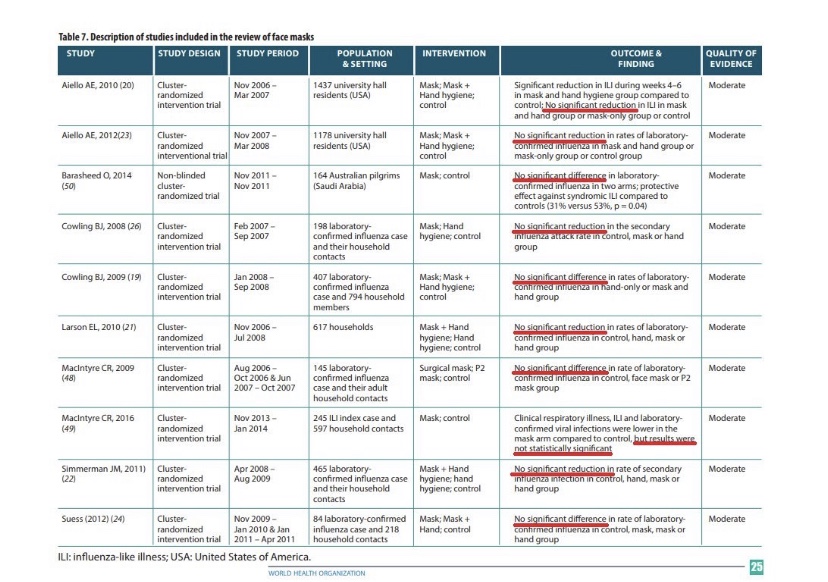
We’ve known for a long time that masks do little to stop the spread of viral particles. They become airborne as aerosols which easily penetrate the kind of cloth masks worn by most members of the public, to say nothing of making contact with their eyes. The table below contains citations to research over the past 10 years uniformly rejecting the hypothesis of a significant protective effect against influenza from masks. There is no reason to believe that they would be more effective in preventing C19 infections.
The CDC’s report on dining restrictions and mask mandates is a weak analysis. They wish to emphasize their faith in non-pharmaceutical interventions (NPIs) to minimize risks. They do so at a time when the vaccinated share of the most vulnerable population, the elderly, has climbed above 50% and is increasing steadily. Thus, risks are falling dramatically, so it’s past time to weigh the costs and benefits of NPIs more realistically. The timing of the report also seemed suspicious, coming as it did in the heat of the battle over the $1.9 trillion COVID relief bill, which subsequently passed.
It’s also a good time to note that zero risk, including “Zero COVID”, is not a realistic or worthwhile goal under any reasonable comparison of costs and benefits. Furthermore, NPIs have proven weak generally (also see here); claims to the contrary should always make us wary.
