Tags
Aerosols, Anne Wheeler, Cloth Masks, Comorbitities, Coronavirus, Covid-19, Delta Variant, Emotional Interference, Endemicity, Germaphobia, Influenza, Mask Mandates, Masks, Michael Levitt, OCD Therapy, Outdoor Infectiions, Precautionary Principle, Randomized Control Trials, Seasonality, Viral Interference, Viral Transmission

It’s been clear since the beginning of the pandemic that your chance of getting infected with COVID outside is close to zero. (Also see here). Yet I still see a few masked people on the beach, in the park, on balconies, and walking in the neighborhood. Given the negligible risk of contracting COVID outdoors, the marginal benefit of masking outdoors is infinitesimal. Likewise, the benefit of a mask to the sole occupant of a vehicle is about zilch. Okay, some individuals might forget to remove their masks after leaving a “high-risk” environment. Sure, maybe, but cloth masks really don’t stop the dispersion of fine aerosols anywhere, indoors or outdoors. Of course, the immune-compromised have a reasonable excuse to apply the precautionary principle, but generally not outside with good air quality.
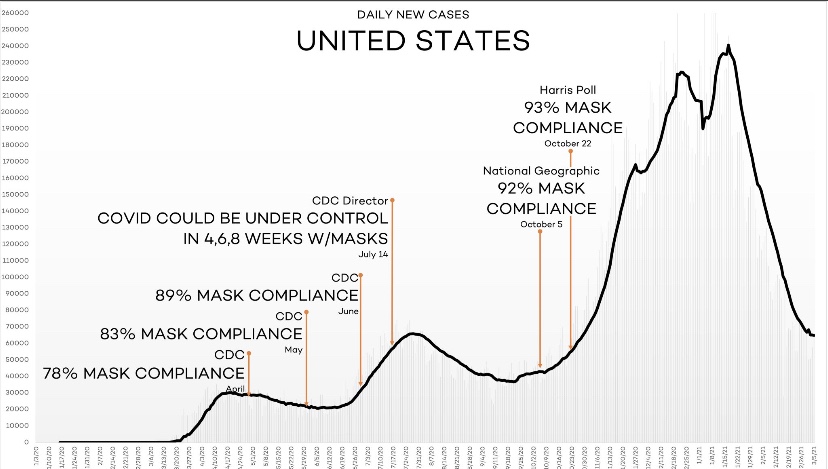
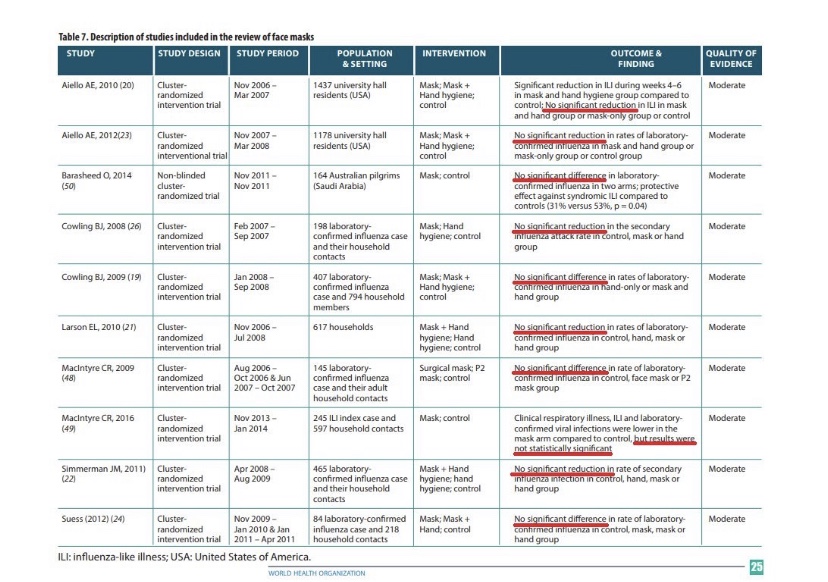
The following link provides a list of mask studies, and meta-studies. Several describe randomized control trials (RCTs). They vary in context, but all of them reject the hypothesis that masks are protective. Positive evidence on mask efficacy is lacking in health care settings, in community settings, and in school settings, and the evidence shows that masks create “pronounced difficulties” for young children and “emotional interference” for school children of all ages. Here’s another article containing links to more studies demonstrating the inefficacy of masks. Also see here. And this article is not only an excellent summary of the research, but it also highlights the hypocrisy of the “follow the science” public health establishment with respect to RCTs. Compliance is not even at issue in many of these studies, though if you think masks matter, it is always an issue in practice. Even studies claiming that cloth masks of the type normally worn by the public are “effective” usually concede that a large percentage of fine aerosols get through the masks… containing millions of tiny particles. In indoor environments with poor ventilation, those aerosols remain suspended in the air for periods long enough to be inhaled by others. That, in fact, is why masks are ineffective at preventing transmission.
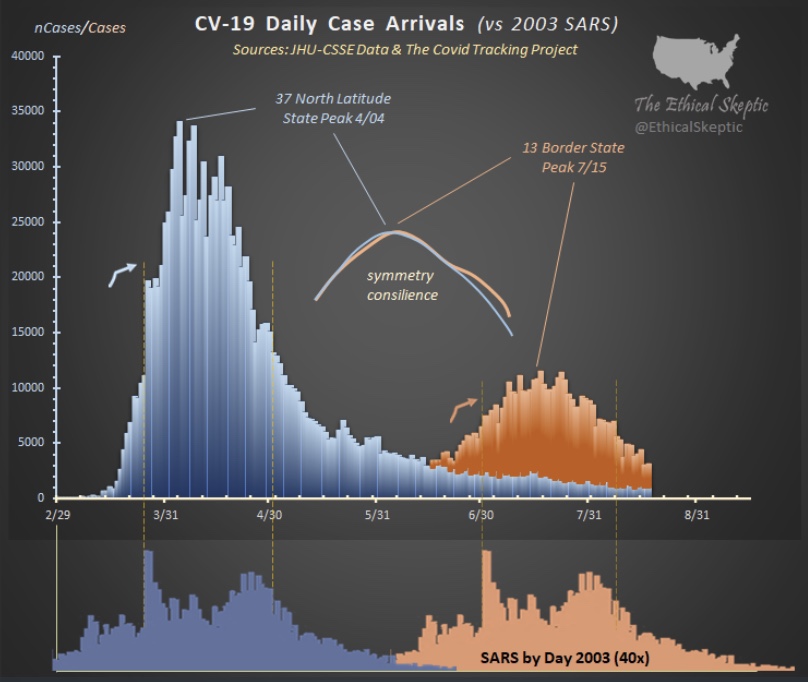
Another dubious claim is that masks are responsible for virtually eliminating cases of influenza in 2020 and 2021. Again, to be charitable, masks are of very limited effectiveness in stopping viral transmission. Moreover, compliance has been weak at best, and areas without mask mandates have experienced the same plunge in flu cases as areas with mandates. A far more compelling explanation is that viral interference caused the steep reduction in flu incidence. The chance of being infected with more than one virus at a time is almost nil. Simply put, COVID outcompeted the flu.
Again, I grant that there are studies (though only a single randomized control trial out of India of which I’m aware) that have demonstrated significant protective effects. Even then, however, the mixed nature of this body of research does not support intrusive masking requirements.
Nevertheless, masks are still mandated in some jurisdictions. Those mandates usually don’t apply outdoors, however, and not in your own damn car! Mask mandates contribute to the general climate of fear surrounding COVID, which is wholly unjustified for most children and healthy working-age people. Public health messaging should focus on high-risk individuals: the elderly, the obese, and those having so-called comorbidities and compromised immune systems. Those groups have obvious reasons to be concerned about the virus. They have excuses to be germaphobic! Still, they are at little risk outdoors, the value of masks is doubtful, and breathing deep of fresh air is good for you in any case!
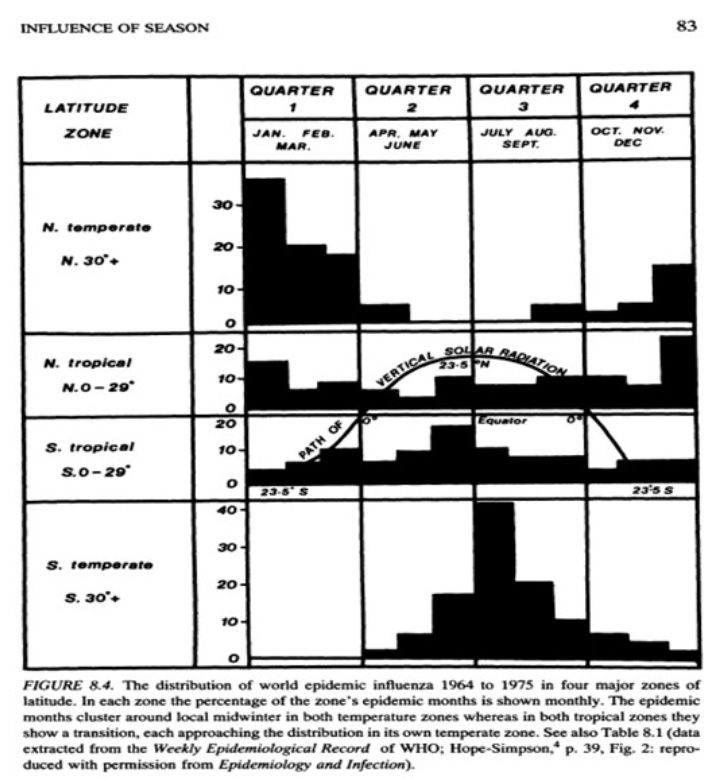
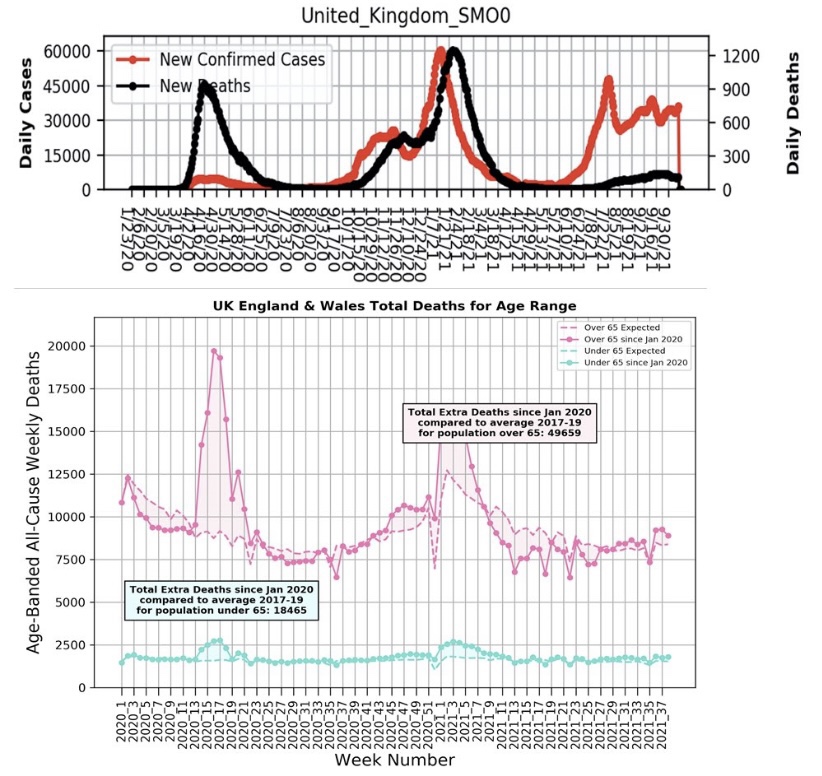
The incidence of COVID has declined substantially in many areas since early September, but the virus is now almost certainly endemic and is likely to return in seasonal waves. However, the Delta wave was far less deadly than earlier variants, a favorable trend many believe will continue. These charts from the UK posted by Michael Levitt demonstrate the improvement vividly. Perhaps the mask craze will fade away as the evidence accumulates.
The pandemic has been a moment of redemption for germaphobes, but no reasonable assessment of risk mitigation relative to the cost, inconvenience, discomfort, and psychological debasement of face jackets can prove their worth outdoors. Their value indoors is nearly as questionable. Yet there remains a stubborn reluctance by public health authorities to lift mask mandates. There are far too many individuals masking outdoors, and to be nice, perhaps it’s mere ignorance. But there are still a few would-be tyrants on Twitter presuming to shame others into joining this pathetic bit of theatre. I believe Anne Wheeler nailed it with this recent tweet:
“This is one of the first things you learn in OCD therapy – you don’t get to make people participate in your compulsions in order to lesson your own anxiety. It’s bizarre that it’s been turned into a virtue.”
There’s also no question that masks are still in vogue as a virtue signal in some circles, but a mask outdoors, especially, is increasingly viewed as a stupid-signal, and for good reason. I’ll continue to marvel at the irrationality of these masked alarmists, who just don’t understand how foolish they look. Give yourself permission to get some fresh air!