I’d just posted an article about the idiocy of masking outdoors, which included a call for an end to the confused public health messaging we’ve heard during the pandemic, when I witnessed something that made my eyes roll:
A fiftyish guy just ahead of me is wearing a mask, walking from the beach toward a public pavilion where there are restrooms. He is barefoot…. and he enters the men’s room and steps right up to the row of urinals. He leaves the restroom without washing his hands.
Perhaps he’s not quiteDarwin Award material, but I ask: do you think this guy’s precautions against potential pathogens and disease vectors were well balanced? It’s not terribly uncommon to see “moisture” or even shallow puddles around public urinals. Don’t go barefoot! Wear flip-flops to the john, at the very least. And wash your hands when you’re done!
Amazingly, the only message related to health and hygiene that our friend has absorbed is to wear a useless mask. And he wears it at the beach! I’m sure he got around to adjusting his mask with unwashed hands at some point. I’ll cut him some slack for wearing a mask inside the restroom, but as my last post noted, that precaution is almost surely wasted effort.
It’s been clear since the beginning of the pandemic that your chance of getting infected with COVID outside is close to zero. (Also see here). Yet I still see a few masked people on the beach, in the park, on balconies, and walking in the neighborhood. Given the negligible risk of contracting COVID outdoors, the marginal benefit of masking outdoors is infinitesimal. Likewise, the benefit of a mask to the sole occupant of a vehicle is about zilch. Okay, some individuals might forget to remove their masks after leaving a “high-risk” environment. Sure, maybe, but cloth masks really don’t stop the dispersion of fine aerosols anywhere, indoors or outdoors. Of course, the immune-compromised have a reasonable excuse to apply the precautionary principle, but generally not outside with good air quality.
The following link provides a list of mask studies, and meta-studies. Several describe randomized control trials (RCTs). They vary in context, but all of them reject the hypothesis that masks are protective. Positive evidence on mask efficacy is lacking in health care settings, in community settings, and in school settings, and the evidence shows that masks create “pronounced difficulties” for young children and “emotional interference” for school children of all ages. Here’s another article containing links to more studies demonstrating the inefficacy of masks. Also see here. And this article is not only an excellent summary of the research, but it also highlights the hypocrisy of the “follow the science” public health establishment with respect to RCTs. Compliance is not even at issue in many of these studies, though if you think masks matter, it is always an issue in practice. Even studies claiming that cloth masks of the type normally worn by the public are “effective” usually concede that a large percentage of fine aerosols get through the masks… containing millions of tiny particles. In indoor environments with poor ventilation, those aerosols remain suspended in the air for periods long enough to be inhaled by others. That, in fact, is why masks are ineffective at preventing transmission.
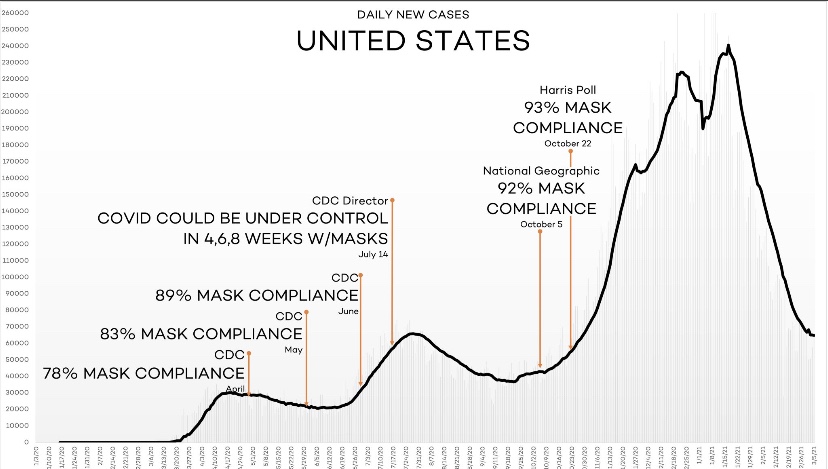
Another dubious claim is that masks are responsible for virtually eliminating cases of influenza in 2020 and 2021. Again, to be charitable, masks are of very limited effectiveness in stopping viral transmission. Moreover, compliance has been weak at best, and areas without mask mandates have experienced the same plunge in flu cases as areas with mandates. A far more compelling explanation is that viral interference caused the steep reduction in flu incidence. The chance of being infected with more than one virus at a time is almost nil. Simply put, COVID outcompeted the flu.
Again, I grant that there are studies (though only a single randomized control trial out of India of which I’m aware) that have demonstrated significant protective effects. Even then, however, the mixed nature of this body of research does not support intrusive masking requirements.
Nevertheless, masks are still mandated in some jurisdictions. Those mandates usually don’t apply outdoors, however, and not in your own damn car! Mask mandates contribute to the general climate of fear surrounding COVID, which is wholly unjustified for most children and healthy working-age people. Public health messaging should focus on high-risk individuals: the elderly, the obese, and those having so-called comorbidities and compromised immune systems. Those groups have obvious reasons to be concerned about the virus. They have excuses to be germaphobic! Still, they are at little risk outdoors, the value of masks is doubtful, and breathing deep of fresh air is good for you in any case!
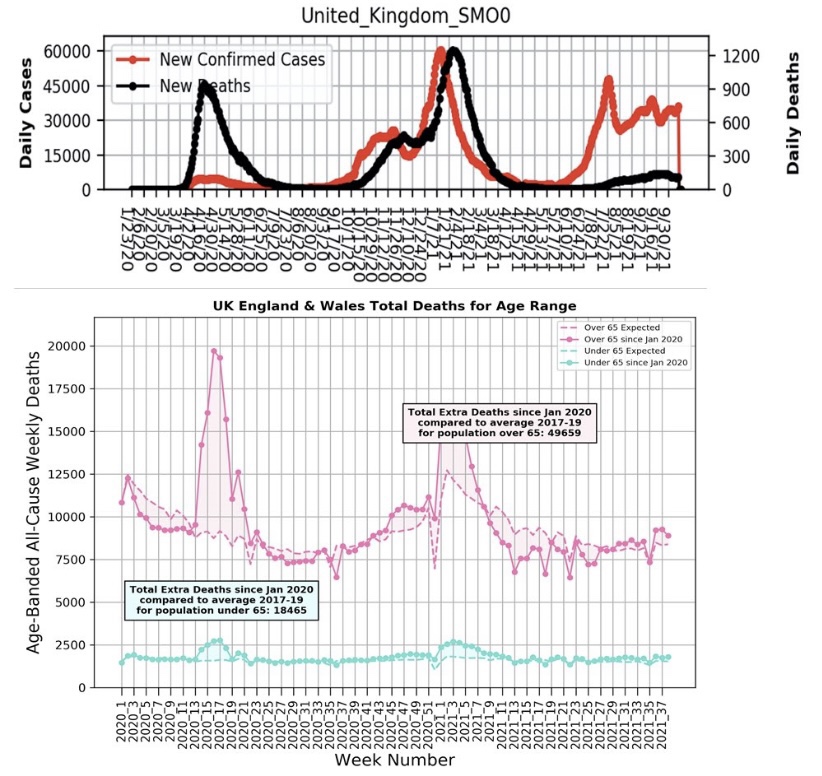
The incidence of COVID has declined substantially in many areas since early September, but the virus is now almost certainly endemic and is likely to return in seasonal waves. However, the Delta wave was far less deadly than earlier variants, a favorable trend many believe will continue. These charts from the UKposted by Michael Levitt demonstrate the improvement vividly. Perhaps the mask craze will fade away as the evidence accumulates.
The pandemic has been a moment of redemption for germaphobes, but no reasonable assessment of risk mitigation relative to the cost, inconvenience, discomfort, and psychological debasement of face jackets can prove their worth outdoors. Their value indoors is nearly as questionable. Yet there remains a stubborn reluctance by public health authorities to lift mask mandates. There are far too many individuals masking outdoors, and to be nice, perhaps it’s mere ignorance. But there are still a few would-be tyrants on Twitter presuming to shame others into joining this pathetic bit of theatre. I believe Anne Wheeler nailed it with this recent tweet:
“This is one of the first things you learn in OCD therapy – you don’t get to make people participate in your compulsions in order to lesson your own anxiety. It’s bizarre that it’s been turned into a virtue.”
There’s also no question that masks are still in vogue as a virtue signal in some circles, but a mask outdoors, especially, is increasingly viewed as a stupid-signal, and for good reason. I’ll continue to marvel at the irrationality of these masked alarmists, who just don’t understand how foolish they look. Give yourself permission to get some fresh air!
She looks good in a mask, and I grant you: masquerades often convey exciting undertones of sexual adventurism. But masquerades and masks should be novelties, not a constant way of life dictated by over-precautious public health authorities.
That brings me to the subject of an outdoor concert I’m attending with some friends on May 8th. It’s to be held at a grassy amphitheater along the Mississippi River in south St. Louis County. Unfortunately, the county health department imposes idiotic rules at this and other outdoor facilities. In the document at the link, it’s clear the rules were given some spin by the band who will perform that night, Jake’s Leg, a very good Grateful Dead cover band. And I get it: these guys just want to play music and perform for their fans, who will be happy to soak in the sounds, party, and dance the night away. Still, some of the rules are absurd and fly in the face of “the science”.
There is a certain libertarian streak among Grateful Deadheads, though in terms of realpolitik, probably the majority is of a more collectivist persuasion (not me). Some in the crowd will welcome the rules and might even go so far as to rat-out anyone whose behavior they find “unsafe”. Others will just go along with the rules as they interpret them. Some like me might push the envelope. But as the evening wears on… what a nice expression, … “as the evening wore on…”, it will be interesting to see whether forces tear loose from the prescriptive axis.
I’ve excerpted some of the rules below and added brief commentary. They appear in the order listed in the document, though it might seem a bit jumbled. I’m sorry to have left out most of the friendly color added by the band:
“Bring a cloth or paper face covering. You will not be allowed entry if you do not have one. Gaiters, bandanas and full-face shields are not acceptable as primary or only face covering. Face coverings must completely cover the nose and mouth. Children under 2 years old are not required to wear a face covering.”
The chances of contracting COVID outdoors are virtually nil, and don’t tell me we’re just learning these details … we’ve known that since almost the beginning of the pandemic. Second, in any case, cloth and paper masks are ineffective at stopping the aerosols responsible for most viral transmission. That’s been known for many years. Our public health experts are only now starting to admit these facts. Allowing toddlers to go maskless is the only concession, and it’s true that transmission by children is unlikely and COVID severity in children is very low. But that goes for older children as well, not just toddlers. Asymptomatic spread is similarly rare, so if you feel good enough to go (and they’ll check your temperature at the gate), you are unlikely to present a risk to anyone.
“Please bring small personal coolers only (no coolers w/ wheels) for your favorite beverages (cans and non- breakables please), along with snacks and food, chairs, blankets and personal use items for you and your small group.”
So, maybe not so bad… it’s about like the usual charade at restaurants: we must enter wearing masks, but then we can rip them off as soon as we find a spot to enjoy the music, our snacks, beverages and those all-important personal use items. Hmm, I guess the unsanitary passing of spleefs ist verboten. A hookah with several hoses could accommodate a small group, but that never goes over with an event staff! Edibles are fine!
“Have your ticket ready to be scanned … and always maintain at least 6 feet social distancing while you’re in line. Markers will be placed as a reminder for you.”
Even indoors, three feet of distancing has been acknowledged as adequate by the undeservedly celebrated Dr. Anthony Fauci.
“Please spread out and maintain at least six feet social distancing from other attendees outside of your small group.There is plenty of room to move and dance.”
More of the same hogwash. Note that the requirements offer no definition of “small group”. To appreciate the absurdity and unnecessary ass-covering inherent in all this, let me point out that my “small group” will consist of six or seven friends who haven’t met as a group in more than a year, We are almost sure to mix with other friends whom we’ll see at the show. So group members will migrate between groups, or small groups might merge into somewhat larger “small groups”. This will be happening all over, and it’s a pretty sure bet there will be lapses in mask compliance. If you happen to be spinning or dancing, the last thing you should do is wear a mask. You need oxygen, and you should avoid trapping hot breath and spittle right up against your face (see the latter part of this article).
“Once you’ve found a place to watch the show, please stay with your group at your area. If you must leave your space, you must wear a face covering at all times whenever you are not able to maintain at least 6 foot social distancing.”
Uh-huh… “Distancing” is not always clear-cut behavior. You pass people coming and going and dancing around. Are you “distancing” on average? Will you be ejected if you briefly come within a few feet of another concert-goer, sans mask? These are matters of uncertain degree, and it’s generally why police don’t enforce mask mandates in pedestrian areas, aside from a few draconian “mask traps” outside stores. Outdoors, it’s absurd.
“Please wash/sanitize your hands before and after using all restroom facilities. Always be kind, think of others and practice social distancing when waiting.”
Post-toilet hand washing is always a good practice, of course, but these guys are nuts! When I arrive at the restroom, I’m generally not worried about the remote chance that my hands will pass the virus to my genitals or vice-versa, and we know that the virus isn’t transmitted from surfaces. It’s also regrettable that masks and distancing will limit those sometimes entertaining conversations in bathroom lines.
“All attendees must adhere to these guidelines regardless of vaccination status.”
This also is sheer stupidity, and I’m complaining only because it reflects the “Zero COVID” mentality of the public health authorities holding us hostage. I guess I’d rather not bring my vaccination card along in any case, and at least they aren’t requiring “vaccine passports” for entry to the venue. But just in case I’m misunderstood, the chance that a fully vaccinated individual will catch or transmit the virus is very low and not even worthy of concern in any rational balancing of risk and benefit.
“Disclaimer: All venue initiatives to prevent the spread of COVID-19 are strictly followed and enforced. Those on premises are subject to compliance with all venue safety procedures and protocols. Non-compliance will result in refused entry or ejection from venue without refund. Upon purchasing tickets for the event, you acknowledge and agree to adhere to all venue policies.”
Again, as a practical matter, some of the rules listed above are virtually unenforceable, but we’ll see how the evening unfolds with a crowd of free-wheeling Deadheads. It could be all strangers stopping strangers, just to bump their elbows. Either way, if past is prelude, the amphitheater will be something of a heart-of-gold land.
The CDC’s new study on dining out and mask mandates is a sham. On its face, the effects reported are small. And while it’s true most of the reported effects are statistically significant, the CDC acknowledges a number of factors that might well have confounded the results. This study should remind us of the infinite number of spurious and “significant” correlations in the world. Here, the timing of the mandates (or their removal) relative to purported effects and seasonal waves is highly suspicious, and as always, attributing causality on the basis of correlation is problematic.
On one hand, the CDC’s results are contrary to plentiful evidence that mandates are ineffective; on the other hand, the results are contrary to earlier CDC “guidance” that masks and limits on indoor dining are “highly effective”. Nevertheless, the latest report has massive propaganda value to the CDC. The media lapped up the story and provided cover for Democrats eager to pass the COVID (C19) relief package. Likewise, the Biden Administration is apparently committed to the narrative of an ongoing crisis as cover for continued attempts to shame political opponents in states that have elected to “reopen” or remain open.
Right off the bat, the study’s authors assert that the primary mode of transmission of C19 is from respiratory droplets. This is false. We know that aerosols are the main culprit in transmission, against which cloth masks are largely ineffective.
Be that as it may, let’s first consider the findings on dining. There was no statistically significant effect on the growth rate of cases or deaths up to 40 days after restrictions were lifted, according to the report. In fact, case growth declined slightly. There was, however, a small but statistically significant increase after 40 days. The fact that deaths seemed to “respond” faster and with greater magnitude than cases makes no sense and suggests that the results might be spurious.
The CDC offers possible explanations the long delay in the purported impact, such as the time required by restaurants to resume operations and early caution on the part of diners. These are speculative, of course. More pertinent is the fact that the data did not distinguish between indoor and outdoor dining, nor did it account for other differences in regulation such as rules on physical distancing, intra-county variation in local government mandates, and compliance levels.
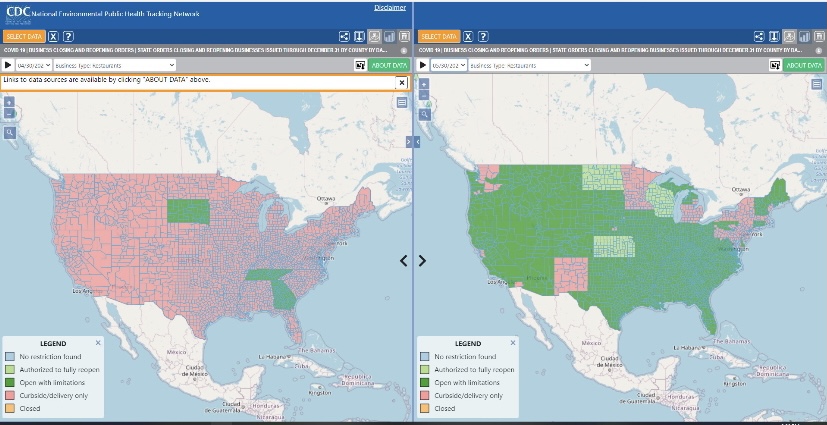
Finally, the measurement of effects covered 100 days after the policy change, but this window spans different stages of the pandemic. There were three waves of infections during 2020, which correspond to the classic Hope-Simpson pattern of virus seasonality. One was near year-end, but as each of the first two waves tapered (April-May, August-September), it should be no surprise that many restrictions were lifted. Within two months, however, new waves had begun. Karl Dierenbach notes that most of the reopenings occurred in May. Here’s how he explains the pattern:
“The map on the left shows counties where there was no on-premises dining (pink) in restaurants as of the beginning of May (4/30). … The map on the right shows that by the end of May, almost the entire country moved to allow some on-premises dining (green).”
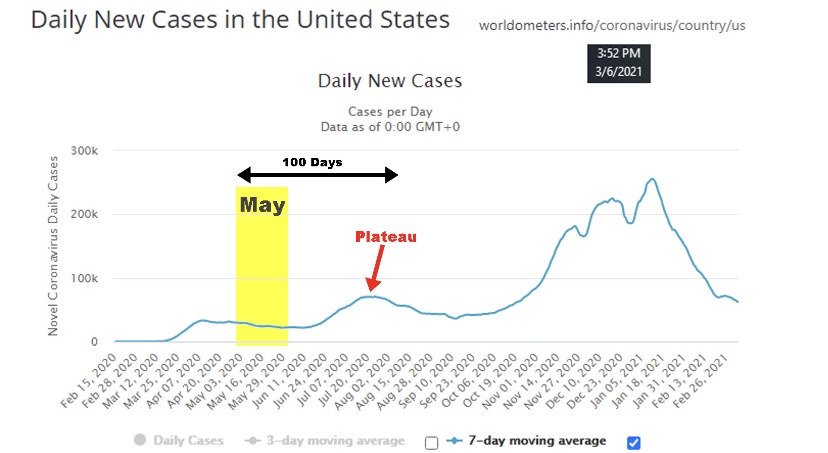
“In the 100 days after May 1, cases nationwide fell slightly, then began to rise, and then plateaued.”
“And what did the CDC find happened after restaurants were allowed (changing mostly in May) to have on-premises dining? … Surprise! The CDC found that cases fell slightly, then began to rise, and then plateaued.”
The summer “mini-wave” is typical of mid- and tropical-latitude seasonality. Thus, the CDC’s findings with respect to dining restrictions are likely an artifact of the strong seasonality of the virus, rather than having anything to do with the lifting of restrictions between waves.
What about the imposition of mask mandates? The CDC’s findings show a much faster response in this case, with statistically significant changes in growth during the first 20 days. Another indicator of spurious correlation is that the growth response of deaths did not lag that of cases, but in fact deaths have reliably lagged cases by over 18 days during the pandemic. Again, the CDC’s caveats apply equally to its findings on masks. A large share of individuals adopted mask use voluntarily before mandates were imposed, so it’s not even clear that the mandates contributed much to the practice.
It’s a stretch to believe that mask mandates would have had an immediate, incremental effect on the growth of cases and deaths, given probable lags in compliance, exposure, and onset of symptoms. Moreover, a number of mask mandates in 2020 were imposed near the very peak of the seasonal waves. Little wonder that the growth rates of cases and deaths declined shortly thereafter.
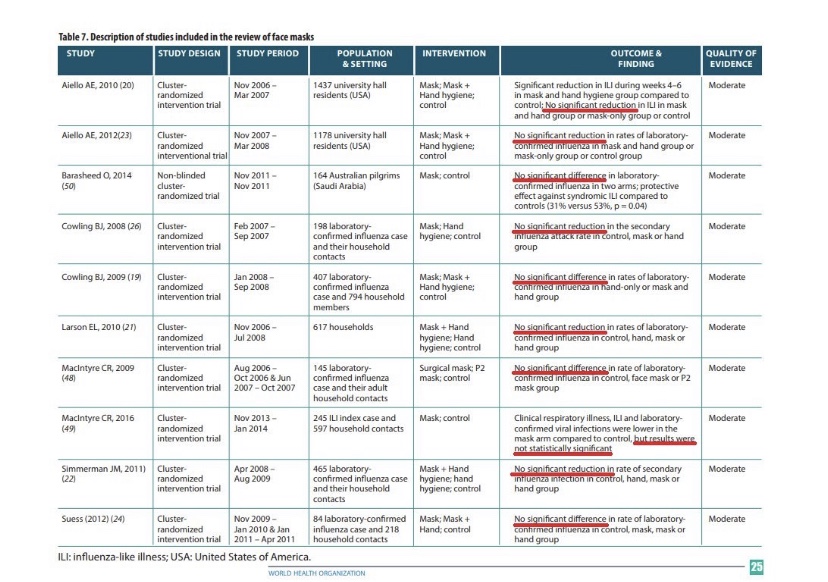
We’ve known for a long time that masks do little to stop the spread of viral particles. They become airborne as aerosols which easily penetrate the kind of cloth masks worn by most members of the public, to say nothing of making contact with their eyes. The table below contains citations to research over the past 10 years uniformly rejecting the hypothesis of a significant protective effect against influenza from masks. There is no reason to believe that they would be more effective in preventing C19 infections.
The CDC’s report on dining restrictions and mask mandates is a weak analysis. They wish to emphasize their faith in non-pharmaceutical interventions (NPIs) to minimize risks. They do so at a time when the vaccinated share of the most vulnerable population, the elderly, has climbed above 50% and is increasing steadily. Thus, risks are falling dramatically, so it’s past time to weigh the costs and benefits of NPIs more realistically. The timing of the report also seemed suspicious, coming as it did in the heat of the battle over the $1.9 trillion COVID relief bill, which subsequently passed.
It’s also a good time to note that zero risk, including “Zero COVID”, is not a realistic or worthwhile goal under any reasonable comparison of costs and benefits. Furthermore, NPIs have proven weak generally (also see here); claims to the contrary should always make us wary.
Anthony Fauci has repeatedly increased his estimate of how much of the population must be vaccinated to achieve what he calls herd immunity, and he did it again in late December. This series of changes, and other mixed messages he’s delivered in the past, reveal Fauci to be a “public servant” who feels no obligation to level with the public. Instead, he crafts messages based on what he believes the public will accept, or on his sense of how the public must be manipulated. For example, by his own admission, his estimates of herd immunity have been sensitive to polling data! He reasoned that if more people reported a willingness to take a vaccine, he’d have flexibility to increase his “public” estimate of the percentage that must be vaccinated for herd immunity. Even worse, Fauci appears to lack a solid understanding of the very concept of herd immunity.
Manipulation
There is so much wrong with his reasoning on this point that it’s hard to know where to start. In the first place, why in the world would anyone think that if more people willingly vaccinate it would imply that even more must vaccinate? And if he felt that way all along it demonstrates an earlier willingness to be dishonest with the public. Of course, there was nothing scientific about it: the series of estimates was purely manipulative. It’s almost painful to consider the sort of public servant who’d engage in such mental machinations.
Immunity Is Multi-Faceted
Second, Fauci seemingly wants to convince us that herd immunity is solely dependent on vaccination. Far from it, and I’m sure he knows that, so perhaps this too was manipulative. Fauci intimates that COVID herd immunity must look something like herd immunity to the measles, which is laughable. Measles is a viral infection primarily in children, among whom there is little if any pre-immunity. The measles vaccine (MMR) is administered to young children along with occasional boosters for some individuals. Believe it or not, Fauci claims that he rationalized a requirement of 85% vaccination for COVID by discounting a 90% requirement for the measles! Really???
In fact, there is substantial acquired pre-immunity to COVID. A meaningful share of the population has long-memory, cross-reactive T-cells from earlier exposure to coronaviruses such as the common cold. Estimates range from 10% to as much as 50%. So if we stick with Fauci’s 85% herd immunity “guesstimate”, 25% pre-immunity implies that vaccinating only 60% of the population would get us to Fauci’s herd immunity goal. (Two qualifications: 1) the vaccines aren’t 100% effective, so it would take more than 60% vaccinated to offset the failure rate; 2) the pre-immune might not be identifiable at low cost, so there might be significant overlap between the pre-immune and those vaccinated.)
Conceptual Confusion
Vaccinations approaching 85% would be an extremely ambitious goal, especially if it is recommended annually or semi-annually. It would be virtually impossible without coercion. While more than 91% of children are vaccinated for measles in the U.S., it is not annual. Thus, measles does not offer an appropriate model for thinking about herd immunity to COVID. Less than half of adults get a flu shot each year, and somewhat more children.
Fauci’s reference to 85% – 90% total immunity is different from the concept of the herd immunity threshold (HIT) in standard epidemiological models. The HIT, often placed in the range of 60% – 70%, is the point at which new infections begin to decline. More infections occur above the HIT but at a diminishing rate. In the end, the total share of individuals who become immune due to exposure, pre-immunity or vaccination will be greater than the HIT. The point is, however, that reaching the HIT is a sufficient condition for cases to taper and an end to a contagion. If we use 65% as the HIT and pre-immunity of 25%, only 40% must be vaccinated to reach the HIT.
Heterogeneity
A recent innovation in epidemiological models is the recognition that there are tremendous differences between individuals in terms of transmissibility, pre-immunity, and other factors that influence the spread of a particular virus, including social and business arrangements. This kind of heterogeneity tends to reduce the effective HIT. We’ve already discussed the effect of pre-immunity. Suppose that certain individuals are much more likely to transmit the virus than others, like so-called super-spreaders. They spur the initial exponential growth of a contagion, but there are only so many of them. Once infected, no one else among the still-susceptible can spread the virus with the same force.
Researchers at the Max Planck Institute (and a number of others) have gauged the effect of introducing heterogeneity to standard epidemiological models. It is dramatic, as the following chart shows. The curves simulate a pandemic under different assumptions about the degree of heterogeneity. The peak of these curves correspond to the HIT under each assumption (R0 refers to the initial reproduction number from infected individuals to others).
Moderate heterogeneity implies a HIT of only 37%. Given pre-immunity of 25%, only an additional 12% of the population would have to be infected or vaccinated to prevent a contagion from gaining a foothold for the initial exponential stage of growth. Fauci’s herd immunity figure obviously fails to consider the effect of heterogeneity.
How Close To the HIT?
We’re not as far from HITs as Fauci might think, and a vaccination goal of 85% is absurd and unnecessary. The seasonal COVID waves we’ve experienced thus far have faded over a period of 10-12 weeks. Estimates of seroprevalence in many localities reached a range of 15% – 25% after those episodes, which probably includes some share of those with pre-immunity. To reach the likely range of a HIT, either some additional pre-immunity must have existed or the degree of heterogeneity must have been large in these populations.
But if that’s true, why did secondary waves occur in the fall? There are a few possibilities. Of course, some areas like the upper Midwest did not experience the springtime wave. But in areas that suffered a recurrance, perhaps the antibodies acquired from infections did not remain active for as long as six months. However, other immune cells have longer memories, and re-infections have been fairly rare. Another possibility is that those having some level of pre-immunity were still able to pass live virus along to new hosts. But this vector of transmission would probably have been quite limited. Pre-immunity almost surely varies from region to region, so some areas were not as firmly above their HITs as others. It’s also possible that infections from super-spreaders were concentrated within subsets of the population even within a given region, in certain neighborhoods or among some, but not all, social or business circles. Therefore, some subsets or “sub-herds” achieved a HIT in the first wave, but it was unnecessary for other groups. In other words, sub-herds spared in the first wave might have suffered a contagion in a subsequent wave. And again, reinfections seem to have been rare. Finally, there is the possibility of a reset in the HIT in the presence of a new, more transmissible variant of the virus, as has become prevalent in the UK, but that was not the case in the fall.
Fragility
Tyler Cowen has mentioned another possible explanation: so-called “fragile” herd immunity. The idea is that any particular HIT is dependent on the structure of social relations. When social distancing is widely practiced, for example, the HIT will be lower. But if, after a contagion recedes, social distancing is relaxed, it’s possible that the HIT will take a higher value at the onset of the next seasonal wave. Perhaps this played a role in the resurgence in infections in the fall, but the HIT can be reduced via voluntary distancing. Eventually, acquired immunity and vaccinations will achieve a HIT under which distancing should be unnecessary, and heterogeneity suggests that shouldn’t be far out of reach.
Conclusion
Anthony Fauci has too often changed his public pronouncements on critical issues related to management of the COVID pandemic. Last February he said cruises were fine for the healthy and that most people should live their lives normally. Oops! Then came his opinion on the limited effectiveness of masks, then a shift to their necessity. His first position on masks has been called a “noble lie” intended to preserve supplies for health care workers. However, Fauci was probably repeating the standing consensus at that point (and still the truth) that masks are of limited value in containing airborne pathogens.
This time, Fauci admitted to changing his estimate of “herd immunity” in response to public opinion, a pathetic approach to matters of public health. What he called herd immunity was really an opinion about adequate levels of vaccination. Furthermore, he neglected to consider other forms of immunity: pre-existing and already acquired. He did not distinguish between total immunity and the herd immunity threshold that should guide any discussion of pandemic management. He also neglected the significant advances in epidemiological modeling that recognize the reality of heterogeneity in reducing the herd immunity threshold. The upshot is that far fewer vaccinations are needed to contain future waves of the pandemic than Fauci suggests.
The other day a friend told me “your data points always seem to miss the people points.” He imagines a failure on my part to appreciate the human cost of the coronavirus. Evidently, he feels that I treat data on cases, hospitalizations, and deaths as mere accounting issues, all while emphasizing the negative aspects of government interventions.
This fellow reads my posts very selectively, hampered in part by his own mood affiliation. Indeed, he seems to lack an appreciation for the nuance and zeitgeist of my body of blogging on the topic… my oeuvre! This despite his past comments on the very things he claims I haven’t mentioned. His responses usually rely on anecdotes relayed to him by nurses or doctors he knows. Anecdotes can be important, of course. But I know nurses and doctors too, and they are not of the same mind as his nurses and doctors. Anecdotes! We’re talking about the determination of optimal policy here, and you know what Dr. Fauci says about relying on anecdotes!
Incremental Costs and Benefits
My friend must first understand that my views are based on an economic argument, one emphasizing the benefits and costs of particular actions, including human costs. COVID is dangerous, but primarily to the elderly, and no approach to managing the virus is free. Here are two rather disparate choices:
Mandated minimization of economic and social interactions throughout society over some time interval in the hope of reducing the spread of the virus;
Laissez faire for the general population while minimizing dangers to high-risk individuals, subject to free choice for mentally competent, high-risk individuals.
To be clear, #2 entails all voluntary actions taken by individuals to mitigate risks. Therefore, #1 implies a set of incremental binding restrictions on behavior beyond those voluntary actions. However, I also include in #1 the behavioral effects of scare mongering by public officials, who regularly issue pronouncements having no empirical basis.
The first option above entails so-called non-pharmaceutical interventions (NPIs) by government. These are the elements of so-called lockdowns, such as quarantines and other restrictions on mobility, business and consumer activity, social activities, health care activities, school closures, and mask mandates. NPIs carry costs that are increasing in the severity of constraints they impose on society.
And before I proceed, remember this: tallying all fatal COVID cases is really irrelevant to the policy exercise. Nothing we do, or could have done, would save all those lives. We should compare what lives can be saved from COVID via lockdowns, if any, with the cost of those lockdowns in terms of human life and human misery, including economic costs.
Economic Losses
NPIs involve a loss of economic output that can never be recovered… it is gone forever, and a loss is likely to continue for some time to come. That sounds so very anodyne, despite the tremendous magnitude of the loss involved. But let’s stay with it for just a second. The loss of U.S. output in 2020 due to COVID has been estimated at $2.5 trillion. As Don Boudreaux and Tyler Cowen have noted, what we normally spend on safety and precautionary measures (willingness-to-pay), together with the probabilities of losses, implies that we value our lives at less than $4 million on average. Let’s say the COVID death toll reaches 300,000 by year-end (that’s incremental in this case— but it might be a bit high). That equates to a total loss of $1.2 trillion in life-value if we ignore distinctions in life-years lost. Now ask this: if our $2.5 trillion output loss could have saved every one of those 300,000 lives, would it have been worth it? Not even close, and the truth is that the sacrifice will not have saved even a small fraction of those lives. I grant, however, that the economic losses are partly attributable to voluntary decisions, but goaded to a great extent by the alarmist commentary of public health officials.
The full depth of losses is far worse than the dollars and cents comparison above might sound. Output losses are always matched by (and, in value, are exactly the same as) income losses. That involves lost jobs, lost hours, failed businesses, and destroyed careers. Ah, now we’re getting a bit more “human”, aren’t we! It’s nothing short of callous to discount these costs. Unfortunately, the burden falls disproportionately on low-income workers. Our elites can mostly stay home and do their jobs remotely, and earn handsome incomes. The working poor spend their time in line at food banks.
Yes, government checks can help those with a loss of income compete with elites for the available supply of goods, but of course that doesn’t replace the lost supply of goods! Government aid of this kind is a palliative measure; it doesn’t offset the real losses during a suspension of economic activity.
Decimated Public Health
The strain of the losses has been massive in the U.S. and nearly everywhere in the world. People are struggling financially, making do with less on the table, depleting their savings, and seeking forbearance on debts. The emotional strains are no less real. Anxiety is rampant, drug overdoses have increased, calls to suicide hotlines have exploded, and the permanence of the economic losses may add to suicide rates for some time to come. Dr. Robert Redfield of the CDC says more teenagers will commit suicide this year than will die from COVID (also see here). There’s also been a terrifying escalation in domestic abuse during the pandemic, including domestic homicide. The despair caused by economic losses is all too real and should be viewed as a multiplier on the total cost of severe NPIs.
More on human costs: a health care disaster has befallen locked-down populations, including avoidance of care on account of panic fomented by so-called public health experts, the media, and government. Some of the consequences are listed here. But to name just a few, we have huge numbers of delayed cancer diagnoses, which sharply decrease survival time; mass avoidance of emergency room visits, including undiagnosed heart attacks and strokes; and unacceptable delays in cardiac treatments. Moreover, lockdowns worldwide have severely damaged efforts to deal with scourges like HIV, tuberculosis, and malaria.
The CDC reports that excess mortality among 25-44 year-olds this year was up more than 26%, and the vast bulk of these were non-COVID deaths. A Lancet study indicates that a measles outbreak is likely in 2021 due to skipped vaccinations caused by lockdowns. The WHO estimates that 130,000,000 people are starving worldwide due to lockdowns. That is roughly the population of the U.S. east coast. Again, the callousness with which people willfully ignore these repercussions is stunning, selfish and inhumane, or just stupid.
Excess Deaths
Can we quantify all this? Yes we can, as a matter of fact. I’ve offered estimates in the past, and I already mentioned that excess deaths, COVID and non-COVID, are reported on the CDC’s web site. The Ethical Skeptic (TES) does a good job of summarizing these statistics, though the last full set of estimates was from October 31. Here is the graphic from the TES Twitter feed:
Note particularly the huge number of excess deaths attributable to SAAAD (Suicide, Addiction Abandonment, Abuse and Despair): over 50,000! The estimate of life-years lost due to non-COVID excess deaths is almost double that of COVID deaths because of the difference in the age distributions of those deaths.
Here are a few supporting charts on selected categories of excess deaths, though they are a week behind the counts from above. The first is all non-COVID, natural-cause excess deaths (the vertical gap between the two lines), followed by excess deaths from Alzheimer’s and dementia, other respiratory diseases, and malignant neoplasms (cancer):
The clearest visual gap in these charts is the excess Alzheimer’s and dementia deaths. Note the increase corresponding to the start of the pandemic, when these patients were suddenly shut off from loved ones and the company of other patients. I also believe some of these deaths were (and are) due to overwhelmed staff at care homes struck by COVID, but even discounting this category of excess deaths leaves us with a huge number of non-COVD deaths that could have been avoided without lockdowns. This represents a human cost over and above those tied to the economic losses discussed earlier.
Degraded Education and Health
Lockdowns have also been destructive to the education of children. The United Nations has estimated that 24 million children may drop out of school permanently as a result of lockdowns and school closures. This a burden that falls disproportionately on impoverished children. This article in the Journal of the American Medical Association Network notes the destructive impact of primary school closures on educational attainment. Its conclusions should make advocates of school closures reconsider their position, but it won’t:
“… missed instruction during 2020 could be associated with an estimated 5.53 million years of life lost. This loss in life expectancy was likely to be greater than would have been observed if leaving primary schools open had led to an expansion of the first wave of the pandemic.“
Lockdown Inefficacy
Lockdowns just don’t work. There was never any scientific evidence that they did. For one thing, they are difficult to enforce and compliance is not a given. Of course, Sweden offers a prime example that draconian lockdowns are unnecessary, and deaths remain low there. This Lancet study, published in July, found no association between lockdowns and country mortality, though early border closures were associated with lower COVID caseloads. A French research paper concludes that public decisions had no impact on COVID mortality across 188 countries, U.S. states, and Chinese states. A paper by a group of Irish physicians and scientists stated the following:
“Lockdown has not previously been employed as a strategy in pandemic management, in fact it was ruled out in 2019 WHO and Irish pandemic guidelines, and as expected, it has proven a poor mitigator of morbidity and mortality.”
One of the chief arguments in favor of lockdowns is the fear that asymptomatic individuals circulating in the community (and there are many) would spread the virus. However, there is no evidence that they do. In part, that’s because the window during which an individual with the virus is infectious is narrow, but tests may detect tiny fragments of the virus over a much longer span of time. And there is even some evidence that lockdown measures may increase the spread of the virus!
Lockdown decisions are invariably arbitrary in their impact as well. The crackdown on gyms is one noteworthy example, but gyms are safe. Restaurants don’t turn up in many contact traces either, and yet restaurants have been repeatedly implicated as danger zones. And think of the many small retailers shut down by government, while giant competitors like Wal-Mart continue to operate with little restriction. This is manifest corporatism!
Then there is the matter of mask mandates. As readers of this blog know, I think masks probably help reduce transmission from droplets issued by a carrier, that is, at close range. However, this recent Danish study in the Annals of Internal Medicine found that cloth masks are ineffective in protecting the wearer. They do not stop aerosols, which seem to be the primary source of transmission. They might reduce viral loads, at least if worn properly and either cleaned often or replaced. Those are big “ifs”.
To the extent that masks offer any protection, I’m happy to wear them within indoor public accommodations, at least for the time being. To the extent that people are “scared”, I’m happy to observe the courtesy of wearing a mask, but not outside in uncrowded conditions. To the extent that masks are required under private “house rules”, of course I comply. Public mask mandates outside of government buildings are over the line, however. The evidence that those mandates work is too tenuous and our liberties are too precious too allow that kind of coercion. And private facilities should be subject to private rules only.
QED
So my poor friend is quite correct that COVID is especially deadly to certain cohorts and challenging for the health care community. But he must come to grips with a few realities:
The virus won’t be defeated with NPIs; they don’t work!
NPIs inflict massive harm to human well-being.
Lockdowns or NPIs are little or no gain, high-pain propositions.
The rejection of NPI’s, or lockdowns, is based on compelling “human” data points. As Don Boudreaux says:
“The lockdowns and other restrictions on economic and social activities are astronomically costly – in a direct economic sense, in an emotional and spiritual sense, and in a ‘what-the-hell-do-these-arbitrary-diktats-portend-for-our-freedom?’ sense.”
This doctor has a message for the those denizens of social media with an honest wish to dispense helpful public health advice:
“Americans have admitted that they will meet for Thanksgiving. Scolding and shaming them for wanting this is unlikely to slow the spread of SARS-CoV-2, though it may earn you likes and retweets. Starting with compassion, and thinking of ways they can meet, but as safely as possible, is the task of real public health. Now is the time to save public health from social media.”
This post is devoted to a few coronavirus policies and positions that trouble me.
Counting Deaths: People have the general impression that counting COVID-19 cases and deaths is straightforward. The facts are more reminiscent of the following exchange in the film Arsenic and Old Lace, when Jonathan Brewster angrily insists he has offed more souls than his sweet little aunties have poisoned with elderberry wine:
Dr. Einstein: You cannot count the one in South Bend. He died of pneumonia! Jonathan Brewster: He wouldn’t have died of pneumonia if I hadn’t shot him!
Here, Dr. Einstein wears the shoes of public health authorities who claim that C19 deaths are undercounted. But lives counted as lost from C19, in many cases, are individuals who also had the flu, pneumonia, stroke, kidney failure, and a variety of other co-morbidities. Yes, other causes of death might be induced by the coronavirus, but like Johnny’s victim in South Bend, many would not have died from C19 if they hadn’t had a prior health event. In addition, otherwise unexplained deaths are often attributed to C19 with little justification.
In fact, the C19 death toll has been distorted by a perverse federal hospital reimbursement policy that rewards hospitals for COVID patients. Death certificates seem to list C19 as the cause for almost anyone who dies in or out of a hospital during the pandemic, whether they’ve been tested or not. In fact, deaths have been attributed to C19 despite negative test results when officials decided, for one reason or another, that the test must have been unreliable!
Lockdowns: almost all of the “curve flattening” in late March and April was accomplished by voluntary action, which I’ve covered beforehere. The lockdowns imposed by state and local governments were highly arbitrary and tragic for many workers and business owners who could have continued to operate as safely as many so-called “essential” businesses. Lockdowns in certain areas were also blatant violations of religious rights. There is little to no evidence that lockdowns themselves led to any actual abatement of the virus. And of course, people are fed up!
The Beach: Right now I’m at a wonderful beach condo in Florida for a week. There are other people on the beach, mostly families and a few groups of friends, but there is plenty of open space. You will not catch the coronavirus on a beach like this. And there is almost zero chance you’ll catch it on any beach. In fact, the chance you’ll catch it anywhere outside is minuscule unless you’re jammed so tightly among hundreds of protesters that you can’t even turn around. Yet government officials have closed beaches in many parts of the country while allowing the protests to go on. Oh sure, they think people will CROWD onto beaches as if they’re at a BLM protest… except they’re not. Ah, then it must be banned! That takes a special kind of dumbass.
Waiting for Results: How could we have spent trillions of dollars as a nation on economic stimulus, much of it skimmed off by grifters, but we can’t seem to get sufficient resources to make calls to those awaiting test results? This is a case of misplaced priorities. Even now, people are waiting more than a week for their results, and many are wandering around in the community without knowing their status. Wouldn’t you think we’d get that done? We can conduct well over a half million tests a day, but can’t we find a few bucks to deliver results via phone, email, or text within 24 hours of processing results. This is truly absurd.
Vaccine Candidates: A similar point can be made about vaccine development: We are spending $5 billion on Operation Warp Speed to build capacity in advance for five promising vaccine candidates. These will be identified over the next few months, and it looks as if all five will come from established pharmaceutical majors. There are many more vaccine candidates, however, some being developed by smaller players using inventive new techniques. The OWS expenditure looks pretty meager when you compare it to the trillions in funds the federal government is spending on economic stimulus, especially when finding an effective vaccine would obviate much of the stimulus.
Treatment: Hydroxycloroquine has been found to lower the death rate from COVID-19 in a large controlled trial. Congratulations, morons, for trashing HCQ as a potential treatment, solely because Trump mentioned it. Way to go, dumbasses, for banning the use of a potential treatment that could have saved many thousands of lives.
Air Conditioning: I’m shocked that public health experts haven’t been more vocal about the potentially dangerous effects of running air conditioners at high levels in public buildings. The virus is known to thrive in cool, dry environments, which is exactly what AC creates, yet this seems to have been almost completely ignored.
Vitamin D: Likewise, I think public health experts have been far too reticent about the connection between Vitamin D deficiencies and the severity of C19 (also see here and here). The accumulating evidence about this association offers an explanation for the disturbingly high severity of cases among Black, Asian and Minority Ethnics (BAME), not to mention a possible role in C19 deaths among the generally D-deficient nursing home population. For the love of God, get the word out to the community that Vitamin D supplements might help, and they won’t hurt, and otherwise, tell people to get some sun!
Masks: I’m not in favor of strict mask mandates, but I have trouble understanding the aversion to masks among certain friends. Of course, there’s been way too much mixed messaging on the benefits of masks, and it didn’t all come from politicians! Scientists, the CDC, and the World Health Organization seemingly did everything possible to squander their credibility on this and other issues. However, a consensus now seems to have developed that masks protect others from the wearer and seem to protect the wearer from others as well. It should be obvious that masks offer a middle ground on which the economy can be restarted while mitigating the risks of further contagion. But even if you don’t believe masks protect the wearer, but only protect others from an infected wearer, donning a mask inside buildings, and when social distancing is impossible, still qualifies as a mannerly thing to do.
In advanced civilizations the period loosely called Alexandrian is usually associated with flexible morals, perfunctory religion, populist standards and cosmopolitan tastes, feminism, exotic cults, and the rapid turnover of high and low fads---in short, a falling away (which is all that decadence means) from the strictness of traditional rules, embodied in character and inforced from within. -- Jacques Barzun