Ah, so Mayor Pete Buttigieg of South Bend, Indiana, one of garbling Joe Biden’s campaign surrogates, says Biden will indeed consider a national lockdown if elected. Oh, fine. And Biden accused Trump of destroying the economy? These dumb-asses must think people have memory spans of about a second.
There are several gigantic problems with foggy Joe’s idea: first, it’s not within a president’s power to impose a nationwide lockdown, as the chorus of experts reminded us last spring when Trump mentioned it. Second, the evidence suggests that lockdowns don’t work to eliminate the virus; they delay its spread at best. Third, as we’ve witnessed, lockdowns themselves have enormous public health consequences, leading to a variety of severe maladies, despondency, and excess non-COVID deaths. That’s simply unacceptable. Finally, the economic damage imposed by lockdowns is horrific and often permanent. We’re talking about destroying the independent livelihoods of people. Permanently! Lockdowns are especially hard on those at the bottom of the economic ladder, who are disproportionately minorities. That’s so obvious, and yet very difficult for elites to gather in.
Here’s another one: today Biden said he would impose a “national mandate” on masks and social distancingon Day One of his presidency. Like lockdowns, evidence is accumulating that masks do not work to contain the virus, and in fact they might be counter-productive (also see here, here, here, and here). Biden’s people will probably also insist on a mandating a government-approved contact-tracing app on your cell phone. Not if I can help it! But don’t get me wrong… I wear a mask in public buildings as an act of voluntary cooperation and to be polite. I also hold out some hope that it will keep the viral load minimal should anything float my way, but whatever lands on the mask might stick with it … and me!
Measures like those Biden contemplates are major assaults on our liberty. And the thing is, if any of it comes to pass, the restrictions might never go away. We’ll be asked to do this every flu season, or perhaps permanently to protect each other from “germs”. This is an authoritarian move, one that we should all resist, even if you’re freaked out by the virus. The best way to resist right now is to vote for Donald Trump.
And please, don’t give me any bullshit about our “responsibility” to lock down, and how mandatory masks are necessary to protect the vulnerable. Is poverty now a “responsibility”? The most highly vulnerable can be protected without masks, and maybe better. Beyond that, people must be free to determine their own level of risk tolerance, just as they have for millennia with respect to a broad spectrum of serious risks, pathogens or otherwise. That’s a dimension of freedom about which no one should be so cavalier.
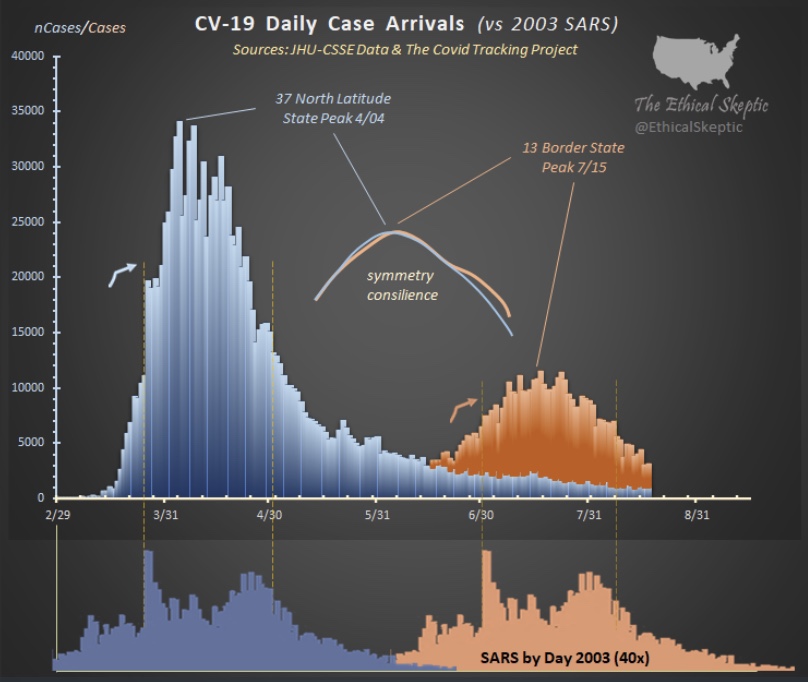
The coronavirus (C19), or SARS-CoV-2, has a strong seasonal component that appears to closely match that of earlier SARS viruses as well as seasonal influenza. This includes the two distinct caseloads we’ve experienced in the U.S. 1) in the late winter/early spring; and 2) the smaller bump we witnessed this summer in some southern states and tropics.
COVID Seasonal Patterns and Latitude
The Ethical Skeptic on Twitter recently featured the chart below. It shows the new case count of C19 in the U.S. in the upper panel, and the 2003 SARS virus in the lower panel. Both viruses had an initial phase at higher latitudes and a summer rebound at lower latitudes.
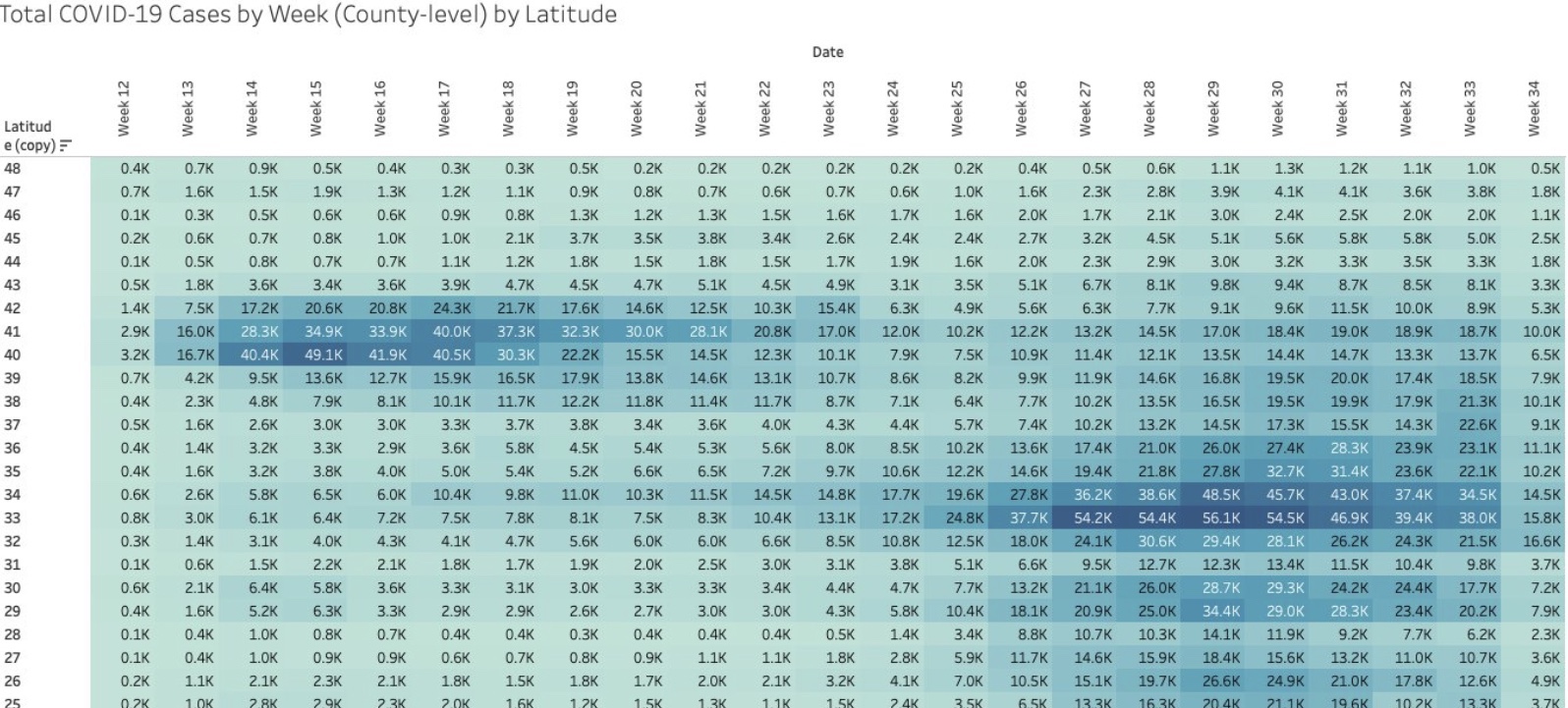
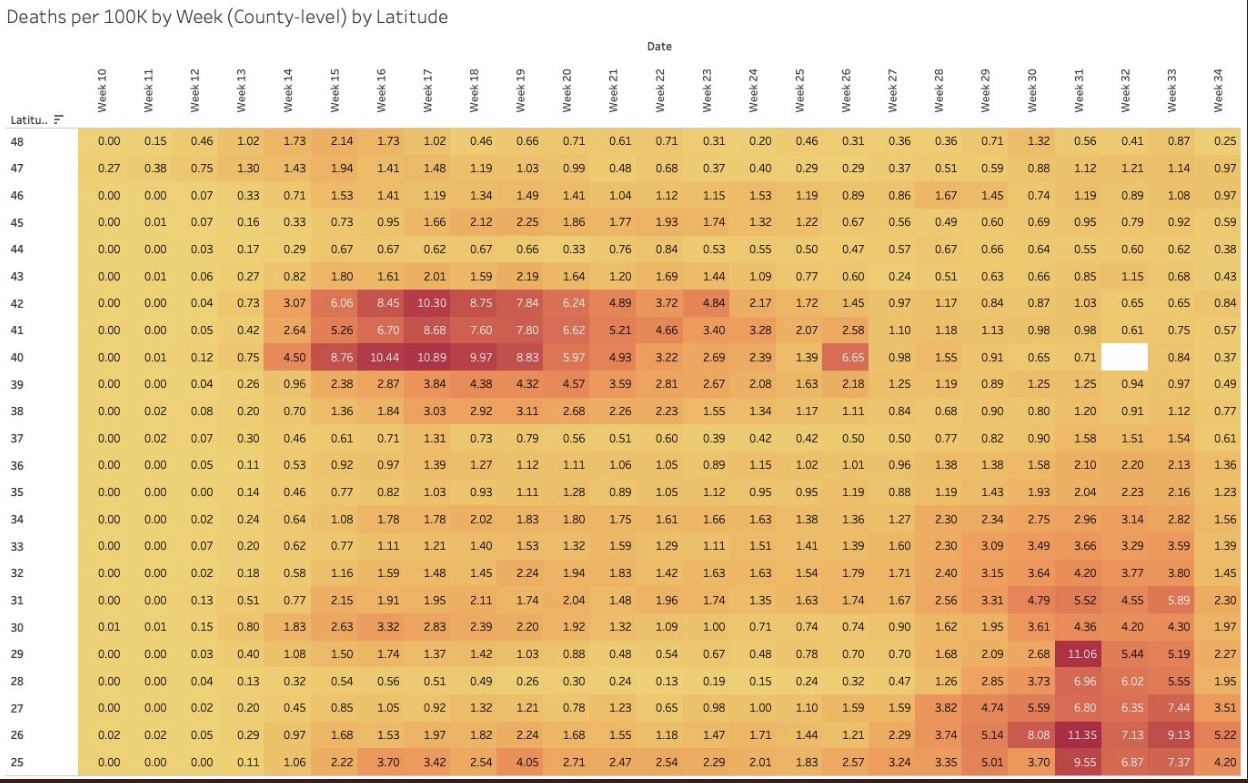
I particularly like the following visualizations from Justin Hart demonstrating the pandemic’s pattern at different latitudes (shown in the leftmost column). The first table shows total cases by week of 2020. The second shows deaths per 100,000 of population by week. Again, notice that lower latitudes have had a crest in the contagion this summer, while higher latitudes suffered the worst of their contagion in the spring. Based on deaths in the second table, the infections at lower latitudes have been less severe.
Viral Patterns in the South
Many expected the pandemic to abate this summer, including me, as it is well known that viruses don’t thrive in higher temperatures and humidity levels, and in more direct sunlight. So it is a puzzle that southern latitudes experienced a surge in the virus during the warmest months of the year. True, the cases were less severe on average, and sunlight and humidity likely played a role in that, along with the marked reduction in the age distribution of cases. However, the SARS pandemic of 2003 followed the same pattern, and the summer surge of C19 at southern latitudes was quite typical of viruses historically.
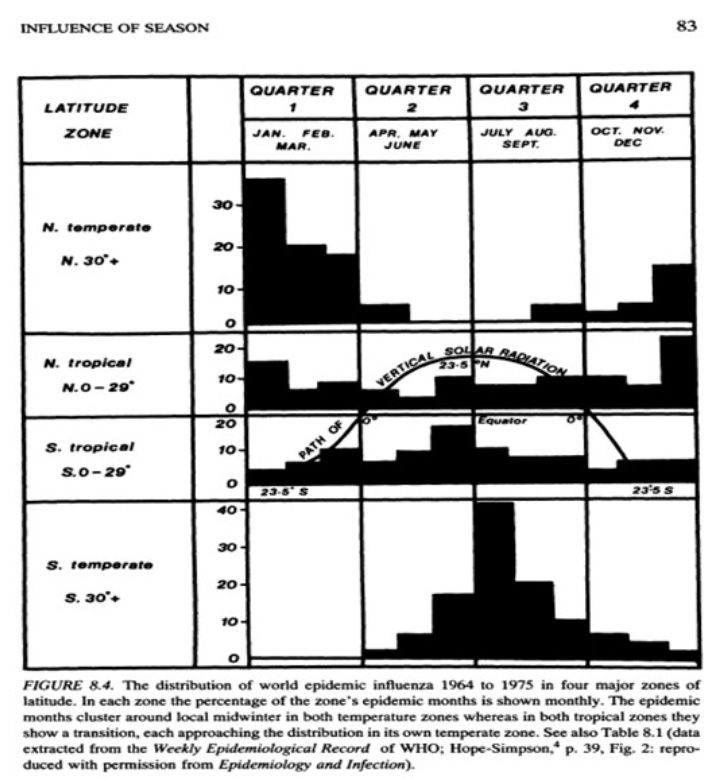
A classic study of the seasonality of viruses was published in 1981 by Robert Edgar Hope-Simpson. The next chart summarized his findings on influenza, seasonality, and latitude based on four groups of latitudes. Northern and southern latitudes above 30° are shown in the top and bottom panels, respectively. Both show wintertime contagions with few infections during the summer months. Tropical regions are different, however. The second and third panels of the chart show flu infections at latitudes less than 30°. Influenza seems to lurk at relatively low levels through most of the year in the tropics, but the respective patterns above and below the equator look almost like very muted versions of activity further to the north and south. However, some researchers describe the tropical pattern as bimodal, meaning that there are two peaks over the course of a year.
So the “puzzle” of the summer surge at low latitudes appears to be more of an empirical regularity. But what gives rise to this pattern in the tropics, given that direct sunlight, temperature, and humidity subdue viral activity?
There are several possible explanations. One is that the summer rainy season in the tropics leads to less sunlight as well as changes in behavior: more time spent indoors and even less exposure to sunlight. In fact, today, in tropical areas where air conditioning is more widespread, it doesn’t have to be rainy to bring people indoors, just hot. Unfortunately, air conditioning dries the air and creates a more hospitable environment for viruses. Moreover, low latitudes are populated by a larger share of dark-skinned peoples, who generally are more deficient in vitamin D. That might magnify the virulence associated with the flight indoors brought on by hot and or rainy weather.
Mutations and Seasonal Patterns
What makes the seasonal patterns noted above so reliable in the face of successful immune responses by recovered individuals? And shouldn’t herd immunity end these seasonal repetitions? The problem is the flu is highly prone to viral mutation, having segments of genes that are highly interchangeable (prompting so-called “antigenic drift“). That’s why flu vaccines are usually different each year: they are customized to prompt an immune response to the latest strains of the virus. Still, the power of these new viral strains are sufficient to propagate the kinds of annual flu cycles documented by Hope-Simpson.
With C19, we know there have been up to 100 mutations, mostly quite minor. Two major strains have been dominant. The first was more common in Southeast Asia near the beginning of the pandemic. It was less virulent and deadly than the strain that hit much of Europe and the U.S. Of course, in July the media misrepresented this strain as “new”, when in fact it had become the most dominant strain back in March and April.
What Lies Ahead
By now, it’s possible that the herd immunity threshold has been surpassed in many areas, which means that a surge this coming fall or winter would be limited to a smaller subset of still-susceptible individuals. The key question is whether C19 will be prone to mutations that pose new danger. If so, it’s possible that the fall and winter will bring an upsurge in cases in northern latitudes both among those still susceptible to existing strains, and to the larger population without immune defenses against new strains.
Fortunately, less dangerous variants are more more likely to be in the interest of the virus’ survival. And thus far, despite the number of minor mutations, it appears that C19 is relatively stable as viruses go. This article quotes Dr. Heidi J. Zapata, an infectious disease specialist and immunologist at Yale, who says that C19:
“… has shown to be a bit slow when it comes to accumulating mutations … Coronaviruses are interesting in that they carry a protein that ‘proofreads’ [their] genetic code, thus making mutations less likely compared to viruses that do not carry these proofreading proteins.”
The flu, however, does not have such a proofreading enzyme, so there is little to check its prodigious tendency to mutate. Ironically, C19’s greater reliability in producing faithful copies of itself should help ensure more durable immunity among those already having acquired defenses against C19.
This means that C19 might not have a strong seasonal resurgence in the fall and winter. Exceptions could include: 1) the remaining susceptible population, should they be exposed to a sufficient viral load; 2) regions that have not yet reached the herd immunity threshold; and 3) the advent of a dangerous new mutation, though existing T-cell immunity may effectively cross-react to defend against such a mutation in many individuals.
Here’s a short list of new or newish research developments, some related to the quest to find COVID treatments. Most of it is good news; some of it is very exciting!
Long-lasting T-cell immunity: this paper in Nature shows that prior exposure to coronaviruses like severe acute respiratory syndrome (SARS) and even the common cold prompt an immune reaction via so-called T-cells that have long memories and are reactive to certain proteins in COVID-19 (SARS-CoV-2). The T-cells were detected in both C19-infected and uninfected patients. This comes after discouraging reports that anti-body responses to C19 are short-lived, but T-cells are a different form of acquired immunity. Derek Lowe says the following:
“This makes one think, as many have been wondering, that T-cell driven immunity is perhaps the way to reconcile the apparent paradox between (1) antibody responses that seem to be dropping week by week in convalescent patients but (2) few (if any) reliable reports of actual re-infection. That would be good news indeed.”
The herd immunity threshold (HIT) is much lower than you think: I’ve written about the effect of heterogeneity on the HIT before, here and here. This new paper, by three Oxford zoologists, shows that the existence of a cohort having some form of prior immunity, innate or acquired, reduces the number of infections required to achieve the HIT. For example, if initial transmissibility (R0) is 2.5 and 40% of the population has prior immunity (both reasonable assumptions for many areas), the HIT is as low as 20%, according to the authors’ calculations. That’s when the contagion begins to recede, though the final infected share of the population would be higher. This might explain why new cases and deaths have already plunged in places like Italy, Sweden, and New York, and why protests in NYC did not lead to a new wave of infections, while those in the south appear to have done so.
Seasonal effects: viral loads might be decreasing. From the abstract:
“Severity of COVID-19 in Europe decreased significantly between March and May and the seasonality of COVID-19 is the most likely explanation. Mucosal barrier and mucociliary clearance can significantly decrease viral load and disease progression, and their inactivation by low relative humidity of indoor air might significantly contribute to severity of the disease.”
The BCG vaccine appears to be protective: this is the bacillus Calmette-Guérin tuberculosis vaccine administered in some countries, This finding is not based on clinical trials, so more work is needed.
Is there no margin in plasma? No subsidy? This is the only “bad news” item on my list. It’s widely agreed that blood plasma from recovered C19 patients can be incorporated into an immune globulin drug to inoculate people against the virus. It’s proven safe, but for various reasons no one seems interested. Not the government. Not private companies. Did Trump happen to mention it or something?
C19 doesn’t spread in schools: this German study demonstrates that there is little risk in reopening schools. One of the researchers says:
“Children act more as a brake on infection. Not every infection that reaches them is passed on…. This means that the degree of immunization in the group of study participants is well below 1 per cent and much lower then we expected. This suggests schools have not developed into hotspots.”
Also worth emphasis is that remote learning leaves much to be desired, as acknowledged by the National Academies of Science, Engineering and Medicine, which has recommended that schools reopen for younger children and those with special needs.
Can angiotensin drugs (ACE Inhibitors/ARBs) reduce mortality? This meta-analysis of nine studies finds that these drugs reduce C19 mortality among patients with hypertension. The drugs were also associated with a reduction in severity but not with statistical significance. These results run contrary to initial suspicions, because ACEI/ARB drugs actually “up-regulate” ACE-2 receptors, to which C19 binds. Researchers say the drugs might be working through some other protective channel. This is not a treatment per se, but this should be reassuring if you already take one of these medications.
Tricor appears to clear lung tissue of C19: this research focused on C19’s preference for an environment rich in cholesterol and other fatty acids:
“What they found is that the novel coronavirus prevents the routine burning of carbohydrates, which results in large amounts of fat accumulating inside lung cells – a condition the virus needs to reproduce.”
Tricor reduces those fats, and the researchers claim it is capable of clearing lung tissue of C19 in a matter of days. This was not a clinical trial, however, so more work is needed. Tricor is an FDA approved drug, so it is safe and could be administered “off label” immediately. Tricor is a fibrate; the news with respect to statins and C19 severity is pretty good too! These are not treatments per se, but this should be reassuring if you already take one of these medications.
Hydroxychloroquine works: despite months of carping from media and leftist know-it-all’s dismissing the mere possibility of HCQ as a potential C19 treatment, evidence is accumulating that it is effective in treating early-stage infections after all. The large study conducted by the Henry Ford Health System found that treatment with HCQ early after hospitalization, and with careful monitoring of heart function, cut the death rate in half relative to a control group. Here’s another: an Indian study found that four-plus maintenance doses of HCQ acted as a prophylactic against C19 infection among health care workers, reducing the odds of infection by more than half. An additional piece of evidence is provided by this analysis of a 14-day Swiss ban on the use of HCQ in late May and early June. The ban was associated with a huge leap in the C19 deaths after a lag of less than two weeks. Resumption of HCQ treatment brought C19 deaths down sharply after a similar lag.
Meanwhile, a study in Lancet purporting to show that HCQ was ineffective and posed significant risks to heart health was retracted based on the poor quality of the data.
Pet ownership might confer some immunity: this one is a little off-beat, and perhaps the research is under-developed, but it is interesting nonetheless!
In advanced civilizations the period loosely called Alexandrian is usually associated with flexible morals, perfunctory religion, populist standards and cosmopolitan tastes, feminism, exotic cults, and the rapid turnover of high and low fads---in short, a falling away (which is all that decadence means) from the strictness of traditional rules, embodied in character and inforced from within. -- Jacques Barzun