We have a false-positive problem and even the New York Times noticed! The number of active COVID cases has been vastly exaggerated and still is, but there is more than one fix.
COVID PCR tests, which are designed to detect coronavirus RNA from a nasal swab, have a “specificity” of about 97%, and perhaps much less in the field. That means at least 3% of tests on uninfected subjects are falsely positive. But the total number of false positive tests can be as large or larger than the total number of true positives identified. Let’s say 3% of the tested population is truly infected. Then out of every 100 individuals tested, three individuals are actively infected and 97 are not. Yet about 3 of those 97 will test positive anyway! So in this example, for every true infection identified, the test also falsely flags an uninfected individual. The number of active infections is exaggerated by 100%.
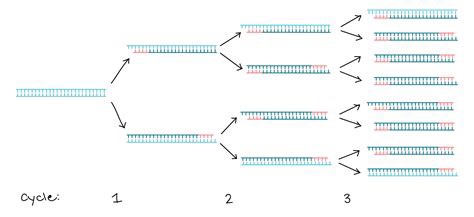
But again, it’s suspected to be much worse than that. The specificity of PCR tests depends on the number of DNA replications, or amplification cycles, to which a test sample is subjected. That process is illustrated through three cycles in the graphic above. It’s generally thought that 20 – 30 cycles is sufficient to pick-up DNA from a live virus infection. If a sample is subjected to more than 30 cycles, the likelihood that the test will detect insignificant dead fragments of the virus is increased. More than 35 cycles prompts real concern about the test’s reliability. But in the U.S., PCR tests are regularly subjected to upwards of 35 and even 40-plus cycles of amplification. This means the number of active cases is exaggerated, perhaps by several times. If you don’t believe me, just ask the great Dr. Anthony Fauci:
“It’s very frustrating for the patients as well as for the physicians … somebody comes in, and they repeat their PCR, and it’s like [a] 37 cycle threshold, but you almost never can culture virus from a 37 threshold cycle. So, I think if somebody does come in with 37, 38, even 36, you got to say, you know, it’s just dead nucleotides, period.“
Remember, the purpose of the test is to find active infections, but the window during which most COVID infections are active is fairly narrow, only for 10 – 15 days after the onset of symptoms, and often less; those individuals are infectious to others only up to about 10 days, and most tests lag behind the onset of symptoms. In fact, infected but asymptomatic individuals — a third or more of all those truly infected at any given time — are minimally infectious, if at all. So the window over which the test should be sensitive is fairly narrow, and many active infections are not infectious at all.
PCR tests are subject to a variety of other criticisms. Many of those are discussed in this external peer-review report on an early 2020 publication favorable to the tests. In addition to the many practical shortfalls of the test, the authors of the original paper are cited for conflicts of interest. And the original paper was accepted within 24 hours of submission to the journal Eurosurveillance (what a name!), which should raise eyebrows to anyone familiar with a typical journal review process.
The most obvious implication of all the false positives is that the COVID case numbers are exaggerated. The media and even public health officials have been very slow to catch onto this fact. As a result, their reaction has sown a panic among the public that active case numbers are spiraling out of control. In addition, false positives lead directly to mis-attribution of death: the CDC changed it’s guidelines in early April for attributing death to COVID (and only for COVID, not other causes of death). This, along with the vast increase in testing, means that false positives have led to an exaggeration of COVID as a cause of death. Even worse, false positives absorb scarce medical resources, as patients diagnosed with COVID require a high level of staffing and precaution, and the staff often requires isolation themselves.
Many have heard that Elon Musk tested positive twice in one day, and tested negative twice in the same day! The uncomfortable reality of a faulty test was recently recognized by an Appeals Court in Portugal, and we may see more litigation of this kind. The Court ruled in favor of four German tourists who were quarantined all summer after one of them tested positive. The Court said:
“In view of current scientific evidence, this test shows itself to be unable to determine beyond reasonable doubt that such positivity corresponds, in fact, to the infection of a person by the SARS-CoV-2 virus.”
I don’t believe testing is a bad thing. The existence of diagnostic tests cannot be a bad thing. In fact, I have advocated for fast, cheap tests, even at the sacrifice of accuracy, so that individuals can test themselves at home repeatedly, if necessary. And fast, cheap tests exist, if only they would be approved by the FDA. Positive tests should always be followed-up immediately by additional testing, whether those are additional PCR tests, other molecular tests, or antigen tests. And as Brown University epidemiologist Andrew Bostom says, you should always ask for the cycle threshold used when you receive a positive result on a PCR test. If it’s above 30 and you feel okay, the test is probably not meaningful.
PCR tests are not ideal because repeat testing is time consuming and expensive, but PCR tests could be much better if the number of replication cycles was reduced to somewhere between 20 and 30. Like most flu and SARS viruses, COVID-19 is very dangerous to the aged and sick, so our resources should be focused on their safety. However, exaggerated case counts are a cause of unnecessary hysteria and cost, especially for a virus that is rather benign to most people.
The other day a friend told me “your data points always seem to miss the people points.” He imagines a failure on my part to appreciate the human cost of the coronavirus. Evidently, he feels that I treat data on cases, hospitalizations, and deaths as mere accounting issues, all while emphasizing the negative aspects of government interventions.
This fellow reads my posts very selectively, hampered in part by his own mood affiliation. Indeed, he seems to lack an appreciation for the nuance and zeitgeist of my body of blogging on the topic… my oeuvre! This despite his past comments on the very things he claims I haven’t mentioned. His responses usually rely on anecdotes relayed to him by nurses or doctors he knows. Anecdotes can be important, of course. But I know nurses and doctors too, and they are not of the same mind as his nurses and doctors. Anecdotes! We’re talking about the determination of optimal policy here, and you know what Dr. Fauci says about relying on anecdotes!
Incremental Costs and Benefits
My friend must first understand that my views are based on an economic argument, one emphasizing the benefits and costs of particular actions, including human costs. COVID is dangerous, but primarily to the elderly, and no approach to managing the virus is free. Here are two rather disparate choices:
Mandated minimization of economic and social interactions throughout society over some time interval in the hope of reducing the spread of the virus;
Laissez faire for the general population while minimizing dangers to high-risk individuals, subject to free choice for mentally competent, high-risk individuals.
To be clear, #2 entails all voluntary actions taken by individuals to mitigate risks. Therefore, #1 implies a set of incremental binding restrictions on behavior beyond those voluntary actions. However, I also include in #1 the behavioral effects of scare mongering by public officials, who regularly issue pronouncements having no empirical basis.
The first option above entails so-called non-pharmaceutical interventions (NPIs) by government. These are the elements of so-called lockdowns, such as quarantines and other restrictions on mobility, business and consumer activity, social activities, health care activities, school closures, and mask mandates. NPIs carry costs that are increasing in the severity of constraints they impose on society.
And before I proceed, remember this: tallying all fatal COVID cases is really irrelevant to the policy exercise. Nothing we do, or could have done, would save all those lives. We should compare what lives can be saved from COVID via lockdowns, if any, with the cost of those lockdowns in terms of human life and human misery, including economic costs.
Economic Losses
NPIs involve a loss of economic output that can never be recovered… it is gone forever, and a loss is likely to continue for some time to come. That sounds so very anodyne, despite the tremendous magnitude of the loss involved. But let’s stay with it for just a second. The loss of U.S. output in 2020 due to COVID has been estimated at $2.5 trillion. As Don Boudreaux and Tyler Cowen have noted, what we normally spend on safety and precautionary measures (willingness-to-pay), together with the probabilities of losses, implies that we value our lives at less than $4 million on average. Let’s say the COVID death toll reaches 300,000 by year-end (that’s incremental in this case— but it might be a bit high). That equates to a total loss of $1.2 trillion in life-value if we ignore distinctions in life-years lost. Now ask this: if our $2.5 trillion output loss could have saved every one of those 300,000 lives, would it have been worth it? Not even close, and the truth is that the sacrifice will not have saved even a small fraction of those lives. I grant, however, that the economic losses are partly attributable to voluntary decisions, but goaded to a great extent by the alarmist commentary of public health officials.
The full depth of losses is far worse than the dollars and cents comparison above might sound. Output losses are always matched by (and, in value, are exactly the same as) income losses. That involves lost jobs, lost hours, failed businesses, and destroyed careers. Ah, now we’re getting a bit more “human”, aren’t we! It’s nothing short of callous to discount these costs. Unfortunately, the burden falls disproportionately on low-income workers. Our elites can mostly stay home and do their jobs remotely, and earn handsome incomes. The working poor spend their time in line at food banks.
Yes, government checks can help those with a loss of income compete with elites for the available supply of goods, but of course that doesn’t replace the lost supply of goods! Government aid of this kind is a palliative measure; it doesn’t offset the real losses during a suspension of economic activity.
Decimated Public Health
The strain of the losses has been massive in the U.S. and nearly everywhere in the world. People are struggling financially, making do with less on the table, depleting their savings, and seeking forbearance on debts. The emotional strains are no less real. Anxiety is rampant, drug overdoses have increased, calls to suicide hotlines have exploded, and the permanence of the economic losses may add to suicide rates for some time to come. Dr. Robert Redfield of the CDC says more teenagers will commit suicide this year than will die from COVID (also see here). There’s also been a terrifying escalation in domestic abuse during the pandemic, including domestic homicide. The despair caused by economic losses is all too real and should be viewed as a multiplier on the total cost of severe NPIs.
More on human costs: a health care disaster has befallen locked-down populations, including avoidance of care on account of panic fomented by so-called public health experts, the media, and government. Some of the consequences are listed here. But to name just a few, we have huge numbers of delayed cancer diagnoses, which sharply decrease survival time; mass avoidance of emergency room visits, including undiagnosed heart attacks and strokes; and unacceptable delays in cardiac treatments. Moreover, lockdowns worldwide have severely damaged efforts to deal with scourges like HIV, tuberculosis, and malaria.
The CDC reports that excess mortality among 25-44 year-olds this year was up more than 26%, and the vast bulk of these were non-COVID deaths. A Lancet study indicates that a measles outbreak is likely in 2021 due to skipped vaccinations caused by lockdowns. The WHO estimates that 130,000,000 people are starving worldwide due to lockdowns. That is roughly the population of the U.S. east coast. Again, the callousness with which people willfully ignore these repercussions is stunning, selfish and inhumane, or just stupid.
Excess Deaths
Can we quantify all this? Yes we can, as a matter of fact. I’ve offered estimates in the past, and I already mentioned that excess deaths, COVID and non-COVID, are reported on the CDC’s web site. The Ethical Skeptic (TES) does a good job of summarizing these statistics, though the last full set of estimates was from October 31. Here is the graphic from the TES Twitter feed:
Note particularly the huge number of excess deaths attributable to SAAAD (Suicide, Addiction Abandonment, Abuse and Despair): over 50,000! The estimate of life-years lost due to non-COVID excess deaths is almost double that of COVID deaths because of the difference in the age distributions of those deaths.
Here are a few supporting charts on selected categories of excess deaths, though they are a week behind the counts from above. The first is all non-COVID, natural-cause excess deaths (the vertical gap between the two lines), followed by excess deaths from Alzheimer’s and dementia, other respiratory diseases, and malignant neoplasms (cancer):
The clearest visual gap in these charts is the excess Alzheimer’s and dementia deaths. Note the increase corresponding to the start of the pandemic, when these patients were suddenly shut off from loved ones and the company of other patients. I also believe some of these deaths were (and are) due to overwhelmed staff at care homes struck by COVID, but even discounting this category of excess deaths leaves us with a huge number of non-COVD deaths that could have been avoided without lockdowns. This represents a human cost over and above those tied to the economic losses discussed earlier.
Degraded Education and Health
Lockdowns have also been destructive to the education of children. The United Nations has estimated that 24 million children may drop out of school permanently as a result of lockdowns and school closures. This a burden that falls disproportionately on impoverished children. This article in the Journal of the American Medical Association Network notes the destructive impact of primary school closures on educational attainment. Its conclusions should make advocates of school closures reconsider their position, but it won’t:
“… missed instruction during 2020 could be associated with an estimated 5.53 million years of life lost. This loss in life expectancy was likely to be greater than would have been observed if leaving primary schools open had led to an expansion of the first wave of the pandemic.“
Lockdown Inefficacy
Lockdowns just don’t work. There was never any scientific evidence that they did. For one thing, they are difficult to enforce and compliance is not a given. Of course, Sweden offers a prime example that draconian lockdowns are unnecessary, and deaths remain low there. This Lancet study, published in July, found no association between lockdowns and country mortality, though early border closures were associated with lower COVID caseloads. A French research paper concludes that public decisions had no impact on COVID mortality across 188 countries, U.S. states, and Chinese states. A paper by a group of Irish physicians and scientists stated the following:
“Lockdown has not previously been employed as a strategy in pandemic management, in fact it was ruled out in 2019 WHO and Irish pandemic guidelines, and as expected, it has proven a poor mitigator of morbidity and mortality.”
One of the chief arguments in favor of lockdowns is the fear that asymptomatic individuals circulating in the community (and there are many) would spread the virus. However, there is no evidence that they do. In part, that’s because the window during which an individual with the virus is infectious is narrow, but tests may detect tiny fragments of the virus over a much longer span of time. And there is even some evidence that lockdown measures may increase the spread of the virus!
Lockdown decisions are invariably arbitrary in their impact as well. The crackdown on gyms is one noteworthy example, but gyms are safe. Restaurants don’t turn up in many contact traces either, and yet restaurants have been repeatedly implicated as danger zones. And think of the many small retailers shut down by government, while giant competitors like Wal-Mart continue to operate with little restriction. This is manifest corporatism!
Then there is the matter of mask mandates. As readers of this blog know, I think masks probably help reduce transmission from droplets issued by a carrier, that is, at close range. However, this recent Danish study in the Annals of Internal Medicine found that cloth masks are ineffective in protecting the wearer. They do not stop aerosols, which seem to be the primary source of transmission. They might reduce viral loads, at least if worn properly and either cleaned often or replaced. Those are big “ifs”.
To the extent that masks offer any protection, I’m happy to wear them within indoor public accommodations, at least for the time being. To the extent that people are “scared”, I’m happy to observe the courtesy of wearing a mask, but not outside in uncrowded conditions. To the extent that masks are required under private “house rules”, of course I comply. Public mask mandates outside of government buildings are over the line, however. The evidence that those mandates work is too tenuous and our liberties are too precious too allow that kind of coercion. And private facilities should be subject to private rules only.
QED
So my poor friend is quite correct that COVID is especially deadly to certain cohorts and challenging for the health care community. But he must come to grips with a few realities:
The virus won’t be defeated with NPIs; they don’t work!
NPIs inflict massive harm to human well-being.
Lockdowns or NPIs are little or no gain, high-pain propositions.
The rejection of NPI’s, or lockdowns, is based on compelling “human” data points. As Don Boudreaux says:
“The lockdowns and other restrictions on economic and social activities are astronomically costly – in a direct economic sense, in an emotional and spiritual sense, and in a ‘what-the-hell-do-these-arbitrary-diktats-portend-for-our-freedom?’ sense.”
This doctor has a message for the those denizens of social media with an honest wish to dispense helpful public health advice:
“Americans have admitted that they will meet for Thanksgiving. Scolding and shaming them for wanting this is unlikely to slow the spread of SARS-CoV-2, though it may earn you likes and retweets. Starting with compassion, and thinking of ways they can meet, but as safely as possible, is the task of real public health. Now is the time to save public health from social media.”
The coronavirus (C19), or SARS-CoV-2, has a strong seasonal component that appears to closely match that of earlier SARS viruses as well as seasonal influenza. This includes the two distinct caseloads we’ve experienced in the U.S. 1) in the late winter/early spring; and 2) the smaller bump we witnessed this summer in some southern states and tropics.
COVID Seasonal Patterns and Latitude
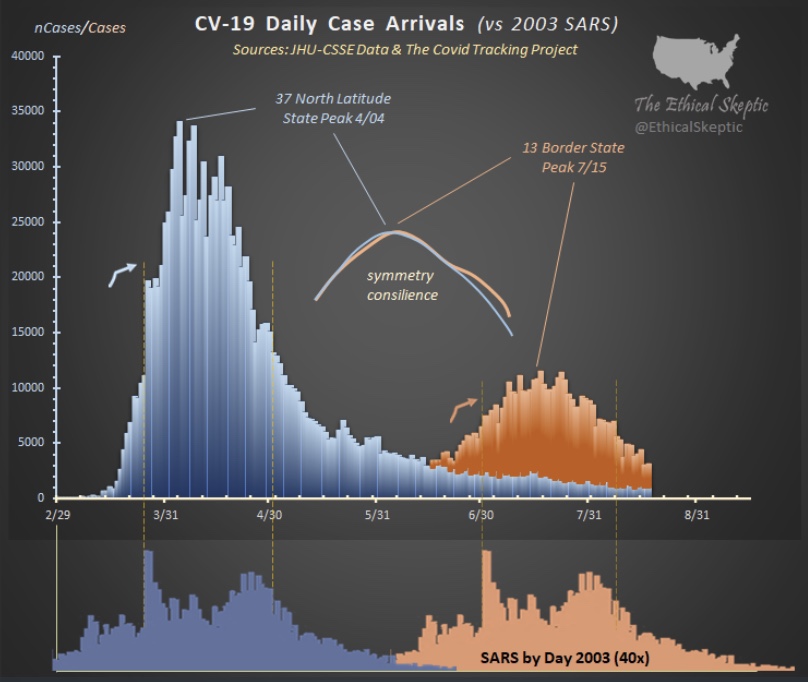
The Ethical Skeptic on Twitter recently featured the chart below. It shows the new case count of C19 in the U.S. in the upper panel, and the 2003 SARS virus in the lower panel. Both viruses had an initial phase at higher latitudes and a summer rebound at lower latitudes.
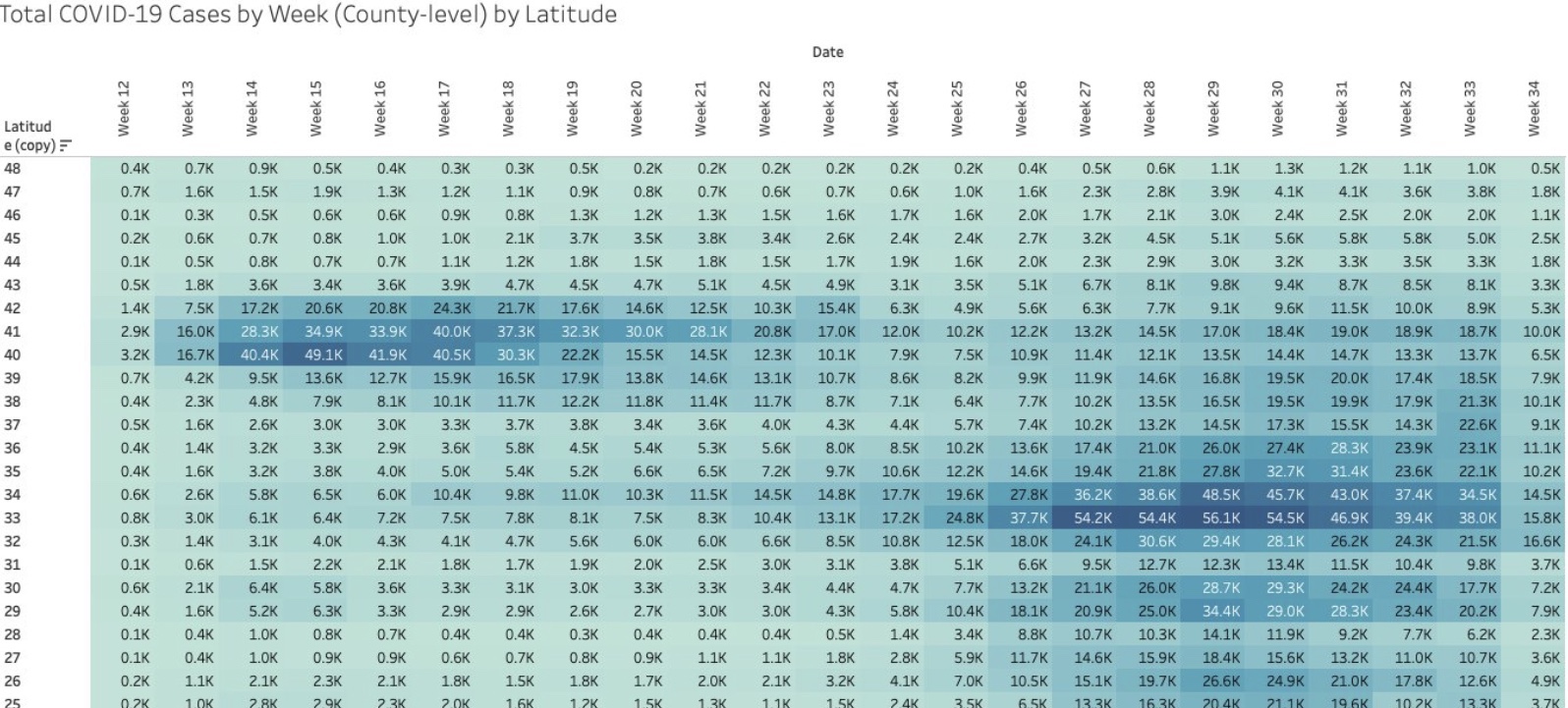
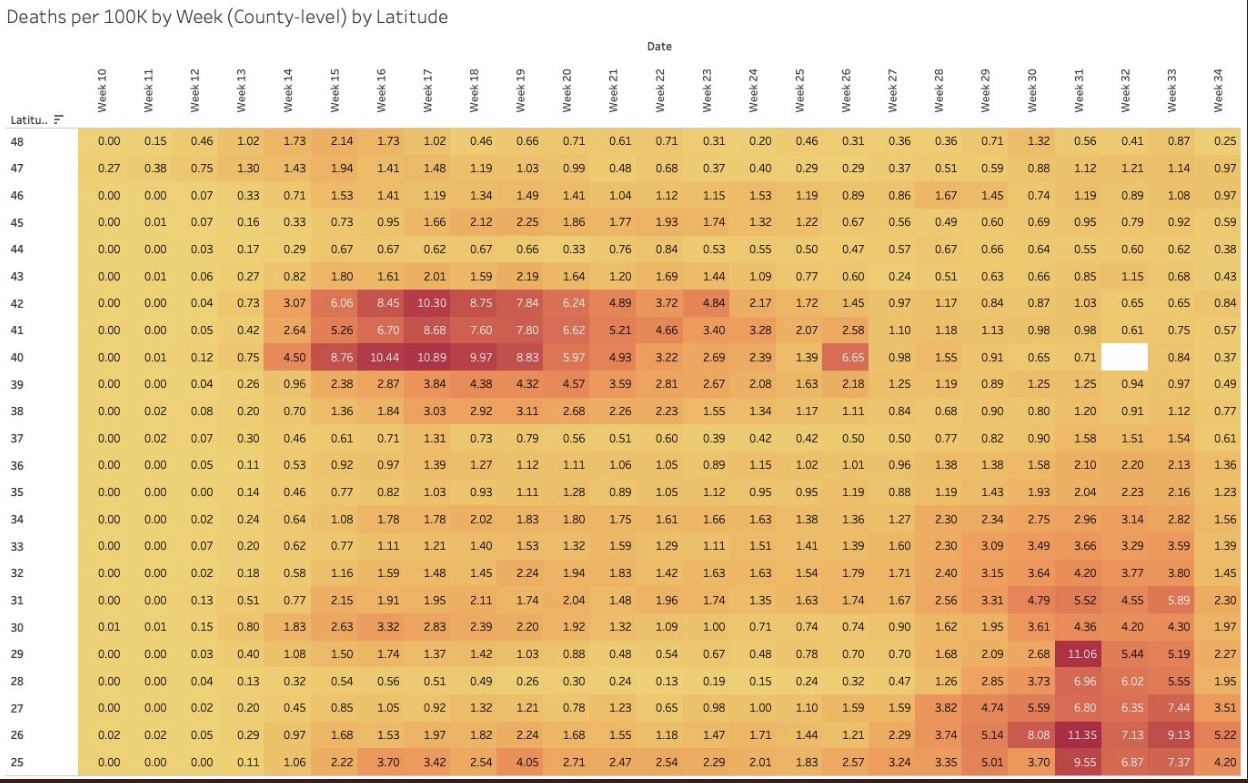
I particularly like the following visualizations from Justin Hart demonstrating the pandemic’s pattern at different latitudes (shown in the leftmost column). The first table shows total cases by week of 2020. The second shows deaths per 100,000 of population by week. Again, notice that lower latitudes have had a crest in the contagion this summer, while higher latitudes suffered the worst of their contagion in the spring. Based on deaths in the second table, the infections at lower latitudes have been less severe.
Viral Patterns in the South
Many expected the pandemic to abate this summer, including me, as it is well known that viruses don’t thrive in higher temperatures and humidity levels, and in more direct sunlight. So it is a puzzle that southern latitudes experienced a surge in the virus during the warmest months of the year. True, the cases were less severe on average, and sunlight and humidity likely played a role in that, along with the marked reduction in the age distribution of cases. However, the SARS pandemic of 2003 followed the same pattern, and the summer surge of C19 at southern latitudes was quite typical of viruses historically.
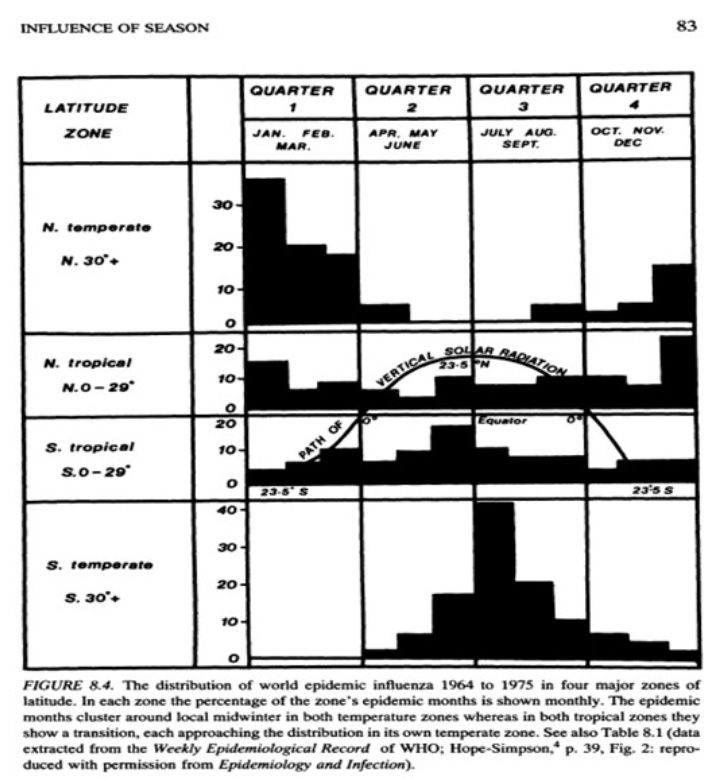
A classic study of the seasonality of viruses was published in 1981 by Robert Edgar Hope-Simpson. The next chart summarized his findings on influenza, seasonality, and latitude based on four groups of latitudes. Northern and southern latitudes above 30° are shown in the top and bottom panels, respectively. Both show wintertime contagions with few infections during the summer months. Tropical regions are different, however. The second and third panels of the chart show flu infections at latitudes less than 30°. Influenza seems to lurk at relatively low levels through most of the year in the tropics, but the respective patterns above and below the equator look almost like very muted versions of activity further to the north and south. However, some researchers describe the tropical pattern as bimodal, meaning that there are two peaks over the course of a year.
So the “puzzle” of the summer surge at low latitudes appears to be more of an empirical regularity. But what gives rise to this pattern in the tropics, given that direct sunlight, temperature, and humidity subdue viral activity?
There are several possible explanations. One is that the summer rainy season in the tropics leads to less sunlight as well as changes in behavior: more time spent indoors and even less exposure to sunlight. In fact, today, in tropical areas where air conditioning is more widespread, it doesn’t have to be rainy to bring people indoors, just hot. Unfortunately, air conditioning dries the air and creates a more hospitable environment for viruses. Moreover, low latitudes are populated by a larger share of dark-skinned peoples, who generally are more deficient in vitamin D. That might magnify the virulence associated with the flight indoors brought on by hot and or rainy weather.
Mutations and Seasonal Patterns
What makes the seasonal patterns noted above so reliable in the face of successful immune responses by recovered individuals? And shouldn’t herd immunity end these seasonal repetitions? The problem is the flu is highly prone to viral mutation, having segments of genes that are highly interchangeable (prompting so-called “antigenic drift“). That’s why flu vaccines are usually different each year: they are customized to prompt an immune response to the latest strains of the virus. Still, the power of these new viral strains are sufficient to propagate the kinds of annual flu cycles documented by Hope-Simpson.
With C19, we know there have been up to 100 mutations, mostly quite minor. Two major strains have been dominant. The first was more common in Southeast Asia near the beginning of the pandemic. It was less virulent and deadly than the strain that hit much of Europe and the U.S. Of course, in July the media misrepresented this strain as “new”, when in fact it had become the most dominant strain back in March and April.
What Lies Ahead
By now, it’s possible that the herd immunity threshold has been surpassed in many areas, which means that a surge this coming fall or winter would be limited to a smaller subset of still-susceptible individuals. The key question is whether C19 will be prone to mutations that pose new danger. If so, it’s possible that the fall and winter will bring an upsurge in cases in northern latitudes both among those still susceptible to existing strains, and to the larger population without immune defenses against new strains.
Fortunately, less dangerous variants are more more likely to be in the interest of the virus’ survival. And thus far, despite the number of minor mutations, it appears that C19 is relatively stable as viruses go. This article quotes Dr. Heidi J. Zapata, an infectious disease specialist and immunologist at Yale, who says that C19:
“… has shown to be a bit slow when it comes to accumulating mutations … Coronaviruses are interesting in that they carry a protein that ‘proofreads’ [their] genetic code, thus making mutations less likely compared to viruses that do not carry these proofreading proteins.”
The flu, however, does not have such a proofreading enzyme, so there is little to check its prodigious tendency to mutate. Ironically, C19’s greater reliability in producing faithful copies of itself should help ensure more durable immunity among those already having acquired defenses against C19.
This means that C19 might not have a strong seasonal resurgence in the fall and winter. Exceptions could include: 1) the remaining susceptible population, should they be exposed to a sufficient viral load; 2) regions that have not yet reached the herd immunity threshold; and 3) the advent of a dangerous new mutation, though existing T-cell immunity may effectively cross-react to defend against such a mutation in many individuals.
Here’s a short list of new or newish research developments, some related to the quest to find COVID treatments. Most of it is good news; some of it is very exciting!
Long-lasting T-cell immunity: this paper in Nature shows that prior exposure to coronaviruses like severe acute respiratory syndrome (SARS) and even the common cold prompt an immune reaction via so-called T-cells that have long memories and are reactive to certain proteins in COVID-19 (SARS-CoV-2). The T-cells were detected in both C19-infected and uninfected patients. This comes after discouraging reports that anti-body responses to C19 are short-lived, but T-cells are a different form of acquired immunity. Derek Lowe says the following:
“This makes one think, as many have been wondering, that T-cell driven immunity is perhaps the way to reconcile the apparent paradox between (1) antibody responses that seem to be dropping week by week in convalescent patients but (2) few (if any) reliable reports of actual re-infection. That would be good news indeed.”
The herd immunity threshold (HIT) is much lower than you think: I’ve written about the effect of heterogeneity on the HIT before, here and here. This new paper, by three Oxford zoologists, shows that the existence of a cohort having some form of prior immunity, innate or acquired, reduces the number of infections required to achieve the HIT. For example, if initial transmissibility (R0) is 2.5 and 40% of the population has prior immunity (both reasonable assumptions for many areas), the HIT is as low as 20%, according to the authors’ calculations. That’s when the contagion begins to recede, though the final infected share of the population would be higher. This might explain why new cases and deaths have already plunged in places like Italy, Sweden, and New York, and why protests in NYC did not lead to a new wave of infections, while those in the south appear to have done so.
Seasonal effects: viral loads might be decreasing. From the abstract:
“Severity of COVID-19 in Europe decreased significantly between March and May and the seasonality of COVID-19 is the most likely explanation. Mucosal barrier and mucociliary clearance can significantly decrease viral load and disease progression, and their inactivation by low relative humidity of indoor air might significantly contribute to severity of the disease.”
The BCG vaccine appears to be protective: this is the bacillus Calmette-Guérin tuberculosis vaccine administered in some countries, This finding is not based on clinical trials, so more work is needed.
Is there no margin in plasma? No subsidy? This is the only “bad news” item on my list. It’s widely agreed that blood plasma from recovered C19 patients can be incorporated into an immune globulin drug to inoculate people against the virus. It’s proven safe, but for various reasons no one seems interested. Not the government. Not private companies. Did Trump happen to mention it or something?
C19 doesn’t spread in schools: this German study demonstrates that there is little risk in reopening schools. One of the researchers says:
“Children act more as a brake on infection. Not every infection that reaches them is passed on…. This means that the degree of immunization in the group of study participants is well below 1 per cent and much lower then we expected. This suggests schools have not developed into hotspots.”
Also worth emphasis is that remote learning leaves much to be desired, as acknowledged by the National Academies of Science, Engineering and Medicine, which has recommended that schools reopen for younger children and those with special needs.
Can angiotensin drugs (ACE Inhibitors/ARBs) reduce mortality? This meta-analysis of nine studies finds that these drugs reduce C19 mortality among patients with hypertension. The drugs were also associated with a reduction in severity but not with statistical significance. These results run contrary to initial suspicions, because ACEI/ARB drugs actually “up-regulate” ACE-2 receptors, to which C19 binds. Researchers say the drugs might be working through some other protective channel. This is not a treatment per se, but this should be reassuring if you already take one of these medications.
Tricor appears to clear lung tissue of C19: this research focused on C19’s preference for an environment rich in cholesterol and other fatty acids:
“What they found is that the novel coronavirus prevents the routine burning of carbohydrates, which results in large amounts of fat accumulating inside lung cells – a condition the virus needs to reproduce.”
Tricor reduces those fats, and the researchers claim it is capable of clearing lung tissue of C19 in a matter of days. This was not a clinical trial, however, so more work is needed. Tricor is an FDA approved drug, so it is safe and could be administered “off label” immediately. Tricor is a fibrate; the news with respect to statins and C19 severity is pretty good too! These are not treatments per se, but this should be reassuring if you already take one of these medications.
Hydroxychloroquine works: despite months of carping from media and leftist know-it-all’s dismissing the mere possibility of HCQ as a potential C19 treatment, evidence is accumulating that it is effective in treating early-stage infections after all. The large study conducted by the Henry Ford Health System found that treatment with HCQ early after hospitalization, and with careful monitoring of heart function, cut the death rate in half relative to a control group. Here’s another: an Indian study found that four-plus maintenance doses of HCQ acted as a prophylactic against C19 infection among health care workers, reducing the odds of infection by more than half. An additional piece of evidence is provided by this analysis of a 14-day Swiss ban on the use of HCQ in late May and early June. The ban was associated with a huge leap in the C19 deaths after a lag of less than two weeks. Resumption of HCQ treatment brought C19 deaths down sharply after a similar lag.
Meanwhile, a study in Lancet purporting to show that HCQ was ineffective and posed significant risks to heart health was retracted based on the poor quality of the data.
Pet ownership might confer some immunity: this one is a little off-beat, and perhaps the research is under-developed, but it is interesting nonetheless!
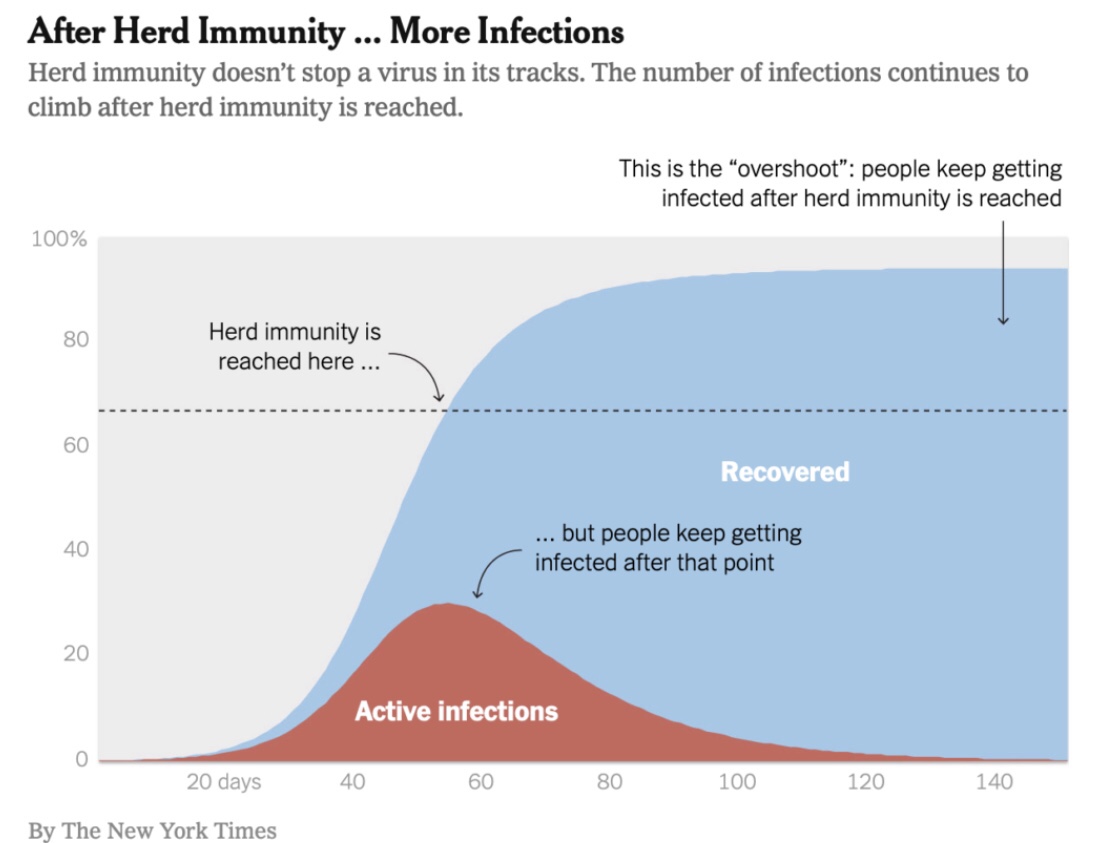
Immunity doesn’t mean you won’t catch the virus. It means you aren’t terribly susceptible to its effects if you do catch it. There is great variation in the population with respect to susceptibility. This simple point may help to sweep away confusion over the meaning of “herd immunity” and what share of the population must be infected to achieve it.
Herd immunity, as defined by Bergstrom and Dean, occurs when there are sufficiently few susceptible individuals remaining in the population to whom the actively-infected can pass the virus. The number of susceptible individuals shrinks over time as more individuals are infected. The chart indicates that new infections will continue after herd immunity is achieved, but the contagion recedes because fewer additional infections are possible.
We tend to think of the immune population as those having already been exposed to the virus, and who have recovered. Those individuals have antibodies specifically targeted at the antigens produced by the virus. But many others have a natural immunity. That is, their immune systems have a natural ability to adapt to the virus.
Heterogeneity
At any point in a pandemic, the uninfected population covers a spectrum of individuals ranging from the highly susceptible to the hardly and non-susceptible. Immunity, in that sense, is a matter of degree. The point is that the number of susceptible individuals doesn’t start at 100%, as most discussions of herd immunity imply, but something much smaller. If a relatively high share of the population has low susceptibility, the virus won’t have to infect such a large share of the population to achieve effective herd immunity.
The apparent differences in susceptibility across segments of the population may be the key to early herd immunity. We’ve known for a while that the elderly and those with pre-existing conditions are highly vulnerable. Otherwise, youth and good health are associated with low vulnerability.
Lemoinereferences a paper written by several epidemiologists showing that “variation in susceptibility” to Covid-19 “lowers the herd immunity threshold”:
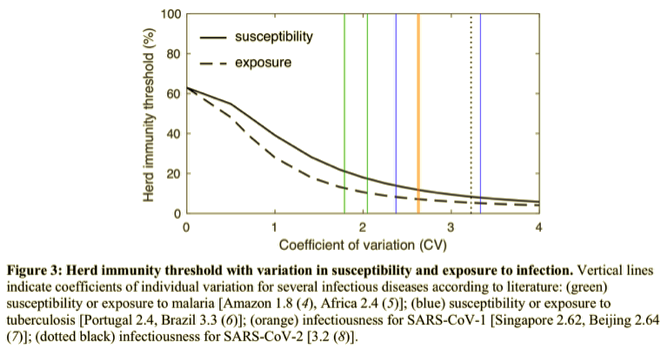
“Although estimates vary, it is currently believed that herd immunity to SARS-CoV-2 requires 60-70% of the population to be immune. Here we show that variation in susceptibility or exposure to infection can reduce these estimates. Achieving accurate estimates of heterogeneity for SARS-CoV-2 is therefore of paramount importance in controlling the COVID-19 pandemic.”
Thechart below is from that paper. It shows a measure of this variation on the horizontal axis. The colored, vertical lines show estimates of historical variation in susceptibility to historical viral episodes. The dashed line shows the required exposure for herd immunity as a function of this measure of heterogeneity.
Their models show that under reasonable assumptions about heterogeneity, the reduction in the herd immunity threshold (in terms of the percent infected) may be dramatic, to perhaps less than 20%.
“As an illustration we show that if R0=2.5 in an age-structured community with mixing rates fitted to social activity studies, and also categorizing individuals into three categories: low active, average active and high active, and where preventive measures affect all mixing rates proportionally, then the disease-induced herd immunity level is hD=43% rather than hC=1−1/2.5=60%.”
Even the celebrated Dr. Bergstrom now admits, somewhat grudgingly, that hereogeniety reduces the herd immunity threshold, though he doesn’t think the difference is large enough to change the policy conversation. Lipsitch also is cautious about the implications.
Augmented Heterogeneity
Theoretically, social distancing reduces the herd immunity threshold. That’s because infected but “distanced” people are less likely to come into close contact with the susceptible. However, that holds only so long as distancing lasts. John Cochrane discusses this at length here. Social distancing compounds the mitigating effect of heterogeneity, reducing the infected share of the population required for herd immunity.
Another compounding effect on heterogeneity arises from the variability of initial viral load on infection (IVL), basically the amount of the virus transmitted to a new host. Zvi Mowshowitz discusses its potential importance and what it might imply about distancing, lockdowns, and the course of the pandemic. In any particular case, a weak IVL can turn into a severe infection and vice versa. In large numbers, however, IVL is likely to bear a positive relationship to severity. Mowshowitz explains that a low IVL can give one’s immune system a head start on the virus. Nursing home infections, taking place in enclosed, relatively cold and dry environments, are likely to involve heavy IVLs. In fact, so-called household infections tend to involve heavier IVLs than infections contracted outside of households. And, of course, you are very unlikely to catch Covid outdoors at all.
Further Discussion
How close are we to herd immunity? Perhaps much closer than we thought, but maybe not close enough to let down our guard. Almost 80% of the population is less than 60 years of age. However, according to this analysis, about 45% of the adult population (excluding nursing home residents) have any of six conditions indicating elevated risk of susceptibility to Covid-19 relative to young individuals with no co-morbidities. The absolute level of risk might not be “high” in many of those cases, but it is elevated. Again, children have extremely low susceptibility based on what we’ve seen so far.
“In summary: While the infectious inoculum required for infection is unknown, these studies indicate that close & prolonged contact is required for #COVID19 transmission. The risk is highest in enclosed environments; household, long-term care facilities and public transport. …
Although limited, these studies so far indicate that susceptibility to infection increases with age (highest >60y) and growing evidence suggests children are less susceptible, are infrequently responsible for household transmission, are not the main drivers of this epidemic.”
Targeted isolation of the highly susceptible in nursing homes, as well as various forms of public “distancing aid” to the independent elderly or those with co-morbidities, is likely to achieve large reductions in the effective herd immunity ratio at low cost relative to general lockdowns.
The existence of so-called super-spreaders is another source of heterogeneity, and one that lends itself to targeting with limitations or cancellations of public events and large gatherings. What’s amazing about this is how the super-spreader phenomenon can lead to the combustion of large “hot spots” in infections even when the average reproduction rate of the virus is low (R0 < 1). This is nicely illustrated by Christopher Moore of the Santa Fe Institute. Super-spreading also implies, however, that while herd immunity signals a reduction in new infections and declines in the actively infected population, “hot spots” may continue to flare up in a seemingly random fashion. The consequences will depend on how susceptible individuals are protected, or on how they choose to mitigate risks themselves.
Conclusion
I’ve heard too many casual references to herd immunity requiring something like 70% of the population to be infected. It’s not that high. Many individuals already have a sort of natural immunity. Recognition of this heterogeneity has driven a shift in the emphasis of policy discussions to the idea of targeted lockdowns, rather than the kind of indiscriminate “dumb” lockdowns we’ve seen. The economic consequences of shifting from broad to targeted lockdowns would be massive. And why not? The health care system has loads of excess capacity, and Covid infection fatality risk (IFR) is turning out to be much lower than the early, naive estimates we were told to expect, which were based on confirmed case fatality rates (CFRs).
I’m often inspired by social media because that’s where the sacred cows graze. Today I saw a juicy one… but actually, the linked article was not surprising: the headline claimed that Jacksonville, Florida residents were flocking to local beaches after they’d been reopened. What grabbed me were the half-witted condemnations made by the poster and his friends. One individual, a Jacksonville resident, claimed that the article was incorrect, that this was “not happening in Jax”. But many of the commenters were horrified by the accompanying photo, a view down the beach showing a number of walkers. If you’ve ever been to a beach, you probably know that such a visual perspective can exaggerate crowd conditions. They looked adequately distanced to me, and I’d bet most of the people or small groups in the photo were a good 20+ feet apart.
The comments on the post were a display of unbridled anger: those people on the beach would be sorry when they caused a second spike in coronavirus cases. How monstrous were these Jaxers to chance infecting others! A few expressed hope that the beachgoers would get sick, as if they’d learn their lesson. And in a delicious case of projection by the uninformed, the hashtag #FloridaMorons was trending on social media. These ugly, nitwitted nannies just can’t get over their need to control their fellow man, while lacking the knowledge to do so sensibly.
Not only did the people on the beach look adequately distanced to the rational eye, but unless you’re an unreformed hugger or “close talker”, the chance of contracting coronavirus outdoors is slim to none! That’s especially true on a beach, where there is typically a decent breeze.
“We all occupy an area in three dimensional space, and as we move away from one another, the volume of air space on which we have an impact expands enormously. ‘If you go from a 10-ft. sphere to a 20-ft. sphere you dilute the concentration [of contaminated air] eight-fold,’ says Dr. Christopher Gill, associate professor of global health at Boston University School of Public Health.”
“‘Within seconds [a virus] can be blown away,’ […] Sunlight may also act as a sterilizer, Gill says. Ultraviolet wavelengths can be murder—literally—on bacteria and viruses, though there hasn’t yet been enough research to establish what exactly the impact of sun exposure is on SARS-CoV-2, the virus responsible for COVID-19.”
There is evidence, however, that high temperatures and humidity reduce the spread of the virus (and see here). That sounds like the beach to me! Whether by droplets or aerosols, confined spaces are where transmission happens. It is almost exclusively an indoors phenomenon, aggravated by HVAC air flows that create dry conditions.
Social distancing is still important at the moment, but keeping people indoors is not conducive to public health. Most of the country (well, outside of downstate New York) is on a path to stanching the contagion. Under these circumstances, you can expect people to push back against unreasonable demands to stay off the beach, stay off an outdoor job, or even stay off their indoor job where there is good ventilation with fresh air, and where distance can be maintained. These little social-media tyrants should pry off their jack-boots and get some sand between their toes!
In advanced civilizations the period loosely called Alexandrian is usually associated with flexible morals, perfunctory religion, populist standards and cosmopolitan tastes, feminism, exotic cults, and the rapid turnover of high and low fads---in short, a falling away (which is all that decadence means) from the strictness of traditional rules, embodied in character and inforced from within. -- Jacques Barzun