The CDC choked on a new analysis estimating COVID-19’s impact on U.S. life expectancy as of year-end 2020: they reported a decline of a full year, which is ridiculous on its face! As explained by Peter B. Bach in STAT News, the agency assumed that excess deaths attributed to COVID in 2020 would continue as a permanentaddition to deaths going forward. Please forgive my skepticism, but isn’t this too basic to qualify as an analytical error by an agency that subjects its reports to thorough vetting? Or might this have been a deliberate manipulation intended to convince the public that COVID will be an ongoing public health crisis. Of course the media has picked it up; even Zero Hedgereported it uncritically!
Bach does a quick calculation based on 400,000 excess deaths attributed to COVID in 2020 and 12 life-years lost by the average victim. I believe the first assumption is on the high side, and I say “attributed to COVID” as a reminder that the CDC’s guidance for completing death certificates was altered in the spring of 2020 specifically for COVID and not other causes of death. Furthermore, if our objective is to assess the impact of the virus itself, under no circumstances should excess deaths induced by misguided lockdown policies enter the calculation (though Bach entertains the possibility). Bach arrives at a reduction in average life of 5.3 days! Of course, that’s not intended to be a projection, but it is a reasonable estimate of COVID’s impact on average lives in 2020.
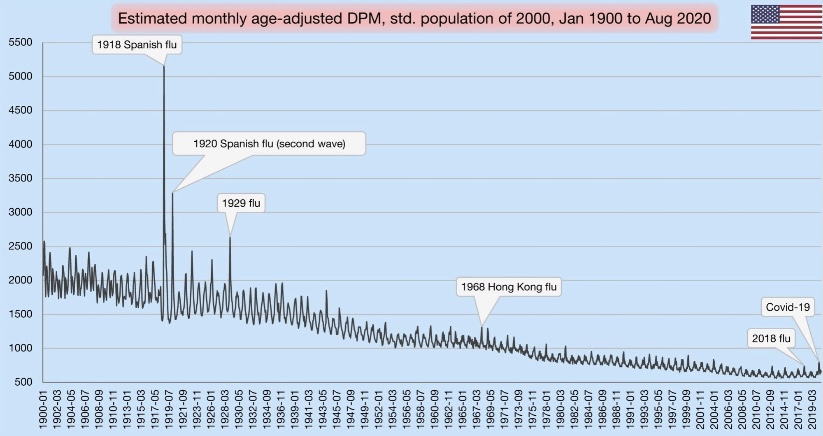
The CDC’s projection essentially freezes death rates at each age at their 2020 values. We will certainly see more COVID deaths in 2021, and the virus is likely to become endemic. Even with higher levels of acquired immunity and widespread vaccinations, there will almost certainly be some ongoing deaths attributable to COVID, but they are likely to be at levels that will blend into a resumption of the long decline in mortality rates, especially if COVID continues to displace the flu in its “ecological niche”. I include the chart at the top to emphasize the long-term improvement in mortality (though the chart shows only a partial year for 2020, and there has been some flattening or slight backsliding over the past five years or so). As Bach says:
“Researchers have regularly demonstrated that life expectancy projections are overly sensitive to evanescent events like pandemics and wars, resulting in considerably overestimated declines. … And yet the CDC published a result that, if anything, would convey to the public an exaggerated toll that Covid-19 took on longevity in 2020. That’s a problem.”
There were excess deaths from other causes in 2020, which Bach acknowledges. Perhaps 100,000 or more could be attributed to lockdowns and their consequences like economically-induced stress, depression, suicide, overdoses, and medical care deferred or never sought. The Zero Hedge article mentioned above discusses findings that lockdowns and their consequences, such as unemployment spells and lost education, will have ongoing negative effects on health and mortality for many years. The net effect on life expectancy might be as large as 11 to 12 days. Again, however, I draw a distinction between deaths caused by the disease and deaths caused by policy mistakes.
The CDC’s estimate should not be taken seriously when, as Kyle Smith says, there is every indication that the battle against COVID is coming to a successful conclusion. Public health experts have not acquitted themselves well during the pandemic, and the CDC’s life expectancy number only reinforces that impression. Here is Smith:
“We have learned a lot about how the virus works, and how it doesn’t: Outdoor transmission, for the most part, hardly ever happens. Kids are at very low risk, especially younger children. Baseball games, barbecues, and summer camps should be fine. Some pre-COVID activities now carry a different risk profile — notably anything that packs crowds together indoors, so Broadway theater, rock concerts, and the like will be just about the last category of activity to return to normal.”
But return to normal we should, and yet the CDC seems determined to poop on the victory party!
The other day a friend told me “your data points always seem to miss the people points.” He imagines a failure on my part to appreciate the human cost of the coronavirus. Evidently, he feels that I treat data on cases, hospitalizations, and deaths as mere accounting issues, all while emphasizing the negative aspects of government interventions.
This fellow reads my posts very selectively, hampered in part by his own mood affiliation. Indeed, he seems to lack an appreciation for the nuance and zeitgeist of my body of blogging on the topic… my oeuvre! This despite his past comments on the very things he claims I haven’t mentioned. His responses usually rely on anecdotes relayed to him by nurses or doctors he knows. Anecdotes can be important, of course. But I know nurses and doctors too, and they are not of the same mind as his nurses and doctors. Anecdotes! We’re talking about the determination of optimal policy here, and you know what Dr. Fauci says about relying on anecdotes!
Incremental Costs and Benefits
My friend must first understand that my views are based on an economic argument, one emphasizing the benefits and costs of particular actions, including human costs. COVID is dangerous, but primarily to the elderly, and no approach to managing the virus is free. Here are two rather disparate choices:
Mandated minimization of economic and social interactions throughout society over some time interval in the hope of reducing the spread of the virus;
Laissez faire for the general population while minimizing dangers to high-risk individuals, subject to free choice for mentally competent, high-risk individuals.
To be clear, #2 entails all voluntary actions taken by individuals to mitigate risks. Therefore, #1 implies a set of incremental binding restrictions on behavior beyond those voluntary actions. However, I also include in #1 the behavioral effects of scare mongering by public officials, who regularly issue pronouncements having no empirical basis.
The first option above entails so-called non-pharmaceutical interventions (NPIs) by government. These are the elements of so-called lockdowns, such as quarantines and other restrictions on mobility, business and consumer activity, social activities, health care activities, school closures, and mask mandates. NPIs carry costs that are increasing in the severity of constraints they impose on society.
And before I proceed, remember this: tallying all fatal COVID cases is really irrelevant to the policy exercise. Nothing we do, or could have done, would save all those lives. We should compare what lives can be saved from COVID via lockdowns, if any, with the cost of those lockdowns in terms of human life and human misery, including economic costs.
Economic Losses
NPIs involve a loss of economic output that can never be recovered… it is gone forever, and a loss is likely to continue for some time to come. That sounds so very anodyne, despite the tremendous magnitude of the loss involved. But let’s stay with it for just a second. The loss of U.S. output in 2020 due to COVID has been estimated at $2.5 trillion. As Don Boudreaux and Tyler Cowen have noted, what we normally spend on safety and precautionary measures (willingness-to-pay), together with the probabilities of losses, implies that we value our lives at less than $4 million on average. Let’s say the COVID death toll reaches 300,000 by year-end (that’s incremental in this case— but it might be a bit high). That equates to a total loss of $1.2 trillion in life-value if we ignore distinctions in life-years lost. Now ask this: if our $2.5 trillion output loss could have saved every one of those 300,000 lives, would it have been worth it? Not even close, and the truth is that the sacrifice will not have saved even a small fraction of those lives. I grant, however, that the economic losses are partly attributable to voluntary decisions, but goaded to a great extent by the alarmist commentary of public health officials.
The full depth of losses is far worse than the dollars and cents comparison above might sound. Output losses are always matched by (and, in value, are exactly the same as) income losses. That involves lost jobs, lost hours, failed businesses, and destroyed careers. Ah, now we’re getting a bit more “human”, aren’t we! It’s nothing short of callous to discount these costs. Unfortunately, the burden falls disproportionately on low-income workers. Our elites can mostly stay home and do their jobs remotely, and earn handsome incomes. The working poor spend their time in line at food banks.
Yes, government checks can help those with a loss of income compete with elites for the available supply of goods, but of course that doesn’t replace the lost supply of goods! Government aid of this kind is a palliative measure; it doesn’t offset the real losses during a suspension of economic activity.
Decimated Public Health
The strain of the losses has been massive in the U.S. and nearly everywhere in the world. People are struggling financially, making do with less on the table, depleting their savings, and seeking forbearance on debts. The emotional strains are no less real. Anxiety is rampant, drug overdoses have increased, calls to suicide hotlines have exploded, and the permanence of the economic losses may add to suicide rates for some time to come. Dr. Robert Redfield of the CDC says more teenagers will commit suicide this year than will die from COVID (also see here). There’s also been a terrifying escalation in domestic abuse during the pandemic, including domestic homicide. The despair caused by economic losses is all too real and should be viewed as a multiplier on the total cost of severe NPIs.
More on human costs: a health care disaster has befallen locked-down populations, including avoidance of care on account of panic fomented by so-called public health experts, the media, and government. Some of the consequences are listed here. But to name just a few, we have huge numbers of delayed cancer diagnoses, which sharply decrease survival time; mass avoidance of emergency room visits, including undiagnosed heart attacks and strokes; and unacceptable delays in cardiac treatments. Moreover, lockdowns worldwide have severely damaged efforts to deal with scourges like HIV, tuberculosis, and malaria.
The CDC reports that excess mortality among 25-44 year-olds this year was up more than 26%, and the vast bulk of these were non-COVID deaths. A Lancet study indicates that a measles outbreak is likely in 2021 due to skipped vaccinations caused by lockdowns. The WHO estimates that 130,000,000 people are starving worldwide due to lockdowns. That is roughly the population of the U.S. east coast. Again, the callousness with which people willfully ignore these repercussions is stunning, selfish and inhumane, or just stupid.
Excess Deaths
Can we quantify all this? Yes we can, as a matter of fact. I’ve offered estimates in the past, and I already mentioned that excess deaths, COVID and non-COVID, are reported on the CDC’s web site. The Ethical Skeptic (TES) does a good job of summarizing these statistics, though the last full set of estimates was from October 31. Here is the graphic from the TES Twitter feed:
Note particularly the huge number of excess deaths attributable to SAAAD (Suicide, Addiction Abandonment, Abuse and Despair): over 50,000! The estimate of life-years lost due to non-COVID excess deaths is almost double that of COVID deaths because of the difference in the age distributions of those deaths.
Here are a few supporting charts on selected categories of excess deaths, though they are a week behind the counts from above. The first is all non-COVID, natural-cause excess deaths (the vertical gap between the two lines), followed by excess deaths from Alzheimer’s and dementia, other respiratory diseases, and malignant neoplasms (cancer):
The clearest visual gap in these charts is the excess Alzheimer’s and dementia deaths. Note the increase corresponding to the start of the pandemic, when these patients were suddenly shut off from loved ones and the company of other patients. I also believe some of these deaths were (and are) due to overwhelmed staff at care homes struck by COVID, but even discounting this category of excess deaths leaves us with a huge number of non-COVD deaths that could have been avoided without lockdowns. This represents a human cost over and above those tied to the economic losses discussed earlier.
Degraded Education and Health
Lockdowns have also been destructive to the education of children. The United Nations has estimated that 24 million children may drop out of school permanently as a result of lockdowns and school closures. This a burden that falls disproportionately on impoverished children. This article in the Journal of the American Medical Association Network notes the destructive impact of primary school closures on educational attainment. Its conclusions should make advocates of school closures reconsider their position, but it won’t:
“… missed instruction during 2020 could be associated with an estimated 5.53 million years of life lost. This loss in life expectancy was likely to be greater than would have been observed if leaving primary schools open had led to an expansion of the first wave of the pandemic.“
Lockdown Inefficacy
Lockdowns just don’t work. There was never any scientific evidence that they did. For one thing, they are difficult to enforce and compliance is not a given. Of course, Sweden offers a prime example that draconian lockdowns are unnecessary, and deaths remain low there. This Lancet study, published in July, found no association between lockdowns and country mortality, though early border closures were associated with lower COVID caseloads. A French research paper concludes that public decisions had no impact on COVID mortality across 188 countries, U.S. states, and Chinese states. A paper by a group of Irish physicians and scientists stated the following:
“Lockdown has not previously been employed as a strategy in pandemic management, in fact it was ruled out in 2019 WHO and Irish pandemic guidelines, and as expected, it has proven a poor mitigator of morbidity and mortality.”
One of the chief arguments in favor of lockdowns is the fear that asymptomatic individuals circulating in the community (and there are many) would spread the virus. However, there is no evidence that they do. In part, that’s because the window during which an individual with the virus is infectious is narrow, but tests may detect tiny fragments of the virus over a much longer span of time. And there is even some evidence that lockdown measures may increase the spread of the virus!
Lockdown decisions are invariably arbitrary in their impact as well. The crackdown on gyms is one noteworthy example, but gyms are safe. Restaurants don’t turn up in many contact traces either, and yet restaurants have been repeatedly implicated as danger zones. And think of the many small retailers shut down by government, while giant competitors like Wal-Mart continue to operate with little restriction. This is manifest corporatism!
Then there is the matter of mask mandates. As readers of this blog know, I think masks probably help reduce transmission from droplets issued by a carrier, that is, at close range. However, this recent Danish study in the Annals of Internal Medicine found that cloth masks are ineffective in protecting the wearer. They do not stop aerosols, which seem to be the primary source of transmission. They might reduce viral loads, at least if worn properly and either cleaned often or replaced. Those are big “ifs”.
To the extent that masks offer any protection, I’m happy to wear them within indoor public accommodations, at least for the time being. To the extent that people are “scared”, I’m happy to observe the courtesy of wearing a mask, but not outside in uncrowded conditions. To the extent that masks are required under private “house rules”, of course I comply. Public mask mandates outside of government buildings are over the line, however. The evidence that those mandates work is too tenuous and our liberties are too precious too allow that kind of coercion. And private facilities should be subject to private rules only.
QED
So my poor friend is quite correct that COVID is especially deadly to certain cohorts and challenging for the health care community. But he must come to grips with a few realities:
The virus won’t be defeated with NPIs; they don’t work!
NPIs inflict massive harm to human well-being.
Lockdowns or NPIs are little or no gain, high-pain propositions.
The rejection of NPI’s, or lockdowns, is based on compelling “human” data points. As Don Boudreaux says:
“The lockdowns and other restrictions on economic and social activities are astronomically costly – in a direct economic sense, in an emotional and spiritual sense, and in a ‘what-the-hell-do-these-arbitrary-diktats-portend-for-our-freedom?’ sense.”
This doctor has a message for the those denizens of social media with an honest wish to dispense helpful public health advice:
“Americans have admitted that they will meet for Thanksgiving. Scolding and shaming them for wanting this is unlikely to slow the spread of SARS-CoV-2, though it may earn you likes and retweets. Starting with compassion, and thinking of ways they can meet, but as safely as possible, is the task of real public health. Now is the time to save public health from social media.”
Acceptance of risk is a necessary part of a good life, and extreme efforts to avoid it are your own business. Government has no power to guarantee absolute safety, nor should we presume to have such a right. Ongoing COVID lockdowns are an implicit assertion of exactly that kind of government power, despite the impotence of those efforts, and they constitute a rejection of more fundamental rights.
Lockdowns have had destructive effects on health and economic well being while conferring little if any benefit in mitigating harm from the virus. The lockdowns were originally sold as a way to “flatten the curve”, that is, to avoid a spike in cases and an overburdened health care system. However, this arguably well-qualified rationale later expanded in scope to encompass the mitigation of smaller and much less deadly outbreaks among younger cohorts, and then to the very idea of extinguishing the virus altogether. It’s become painfully obvious that such measures are not capable of achieving those goals.
In the U.S., the ongoing lockdowns have been a cause célèbre largely on the interventionist Left, and they have been prolonged mainly by Democrats at various levels of government. In a way, this is not unlike many other policies championed by the Left, often ostensibly designed to help members of the underclasses: instead, those policies often destroy or wrongly obviate incentives and promote dependency on the state. In this case, the plunge into dependency is a reality the Left would very much like to ignore, or to blame on someone else. You know who.
The lockdowns have been largely unsuccessful in mitigating the spread of the virus. At the same time, they have been used as a pretext to deny constitutional rights such as the free practice of religion, assembly, and a broad range of unenumerated rights under the “penumbra” of the Bill of Rights and the Ninth Amendment. What’s more, the severity of the economic blow caused by lockdowns has been borne disproportionately by the working poor and the small businesses who employ so many of them.
Lockdowns are deadly. It’s not clear that they’ve saved any lives, but they have massively disrupted the operation of the health care system with major consequences for those with chronic and undiagnosed conditions. The lockdowns have also led to spikes in mental health issues, alcoholism, drug abuse, and deaths of despair. A recent study found that over 26% of the excess deaths during the pandemic were non-COVID deaths. Those deaths were avoidable or accelerated, whereas the lockdowns have failed to meaningfully curtail COVID deaths. Don’t tell me about reduced traffic fatalities: that reduction is relatively small relative to the increase in non-COVID excess deaths (see below).
What proof do we have that lockdowns cause excess deaths? See this study in The Lancet on cancer deaths due to lockdown-induced delays in diagnoses. See this study on UK school closures. See this Oxfam Internationalreport on lockdown-induced starvation. Other reports from the UK suggests that lockdown deaths are widespread, having taken nearly 2,800 per week early in the pandemic, and many other deaths yet to occur have been made inevitable by lockdowns. Doctors in the U.S. have warned that lockdowns are a “mass casualty incident”, and a German government study warned of the same.
The Ethical Skeptic (TES) on Twitter has been tracking a measure of lockdown deaths for some time now. The following graphic provides a breakdown of excess non-COVID deaths since the start of the pandemic. The total “pie” shows almost 320,000 excess deaths through September 26th (avoiding less complete counts in recent weeks), as reported by the CDC. COVID accounted for 202,000 of those deaths, based on state-level reporting. Of the remaining 117,000 excess deaths, TES uses CDC data to allocate roughly 85,000 to various causes, the largest (more than half) being “Suicide, Addiction, Abandonment, and Abuse”. Other large categories include Cardio/Diabetes, Stroke, premature Alzheimers/Dementia death, and Cancer Access. Nearly 32,000 excess deaths remain as a “backlog”, not yet reported with a cause by states.
Also of interest in the graphic are estimates of life-years lost. The vast bulk of COVID victims are elderly, of course, which means that any estimate of lost years per victim must be relatively low. On the other hand, most non-COVID, lockdown-related deaths are among younger victims, with correspondingly greater life-years lost. TES’s aggregate estimate is that lockdown-related excess deaths involve double the life-years lost of COVID deaths. Of course, that is an estimate, but even granting some latitude for error, the reality is horrifying!
John Tierney in City Journal cites several recent studies concluding that lockdowns have been largely ineffective in Europe and in the U.S. While Tierney doesn’t rule out the possibility that lockdowns have produced some benefits, they have carried excessive costs and risks to public health going forward, such as lingering issues for those having deferred important health care decisions as well as disruption in future economic prospects. Ultimately, lockdowns don’t accomplish anything:
“While the economic and social costs have been enormous, it’s not clear that the lockdowns have brought significant health benefits beyond what was achieved by people’s voluntary social distancing and other actions.”
Tierney also discusses the costs and benefits of lockdowns in terms of life years: quality-adjusted life-years (QALY), which is a widely-used measure for evaluating of the use of health care resources:
“By the QALY measure, the lockdowns must be the most costly—and cost-ineffective—medical intervention in history because most of the beneficiaries are so near the end of life. Covid-19 disproportionately affects people over 65, who have accounted for nearly 80 percent of the deaths in the United States. The vast majority suffered from other ailments, and more than 40 percent of the victims were living in nursing homes, where the median life expectancy after admission is just five months. In Britain, a study led by the Imperial College economist David Miles concluded that even if you gave the lockdown full credit for averting the most unrealistic worst-case scenario (the projection of 500,000 British deaths, more than ten times the current toll), it would still flunk even the most lenient QALY cost-benefit test.”
We can now count the World Health Organizationamong the detractors of lockdowns. According to WHO’s Dr. David Nabarro:
“Lockdowns just have one consequence that you must never ever belittle, and that is making poor people an awful lot poorer…. Look what’s happened to smallholder farmers all over the world. … Look what’s happening to poverty levels. It seems that we may well have a doubling of world poverty by next year. We may well have at least a doubling of child malnutrition.”
In another condemnation of the public health consequences of lockdowns, number of distinguished epidemiologists have signed off on a statement known as The Great Barrington Declaration. The declaration advocates a focused approach of protecting the most vulnerable from the virus, while allowing those at low risk to proceed with their lives in whatever way they deem acceptable. Those at low risk of severe disease can acquire immunity, which ultimately inures to the benefit of the most vulnerable. With few, brief, and local exceptions, this is how we have always dealt with pandemics in the past. That’s real life!
People talk about the transmission rate or reproduction rate (R0) of Covid-19 as if it’s a single number that applies to the entire population. John Cochrane emphasizes the huge implications of this misperception for how best to prevent the spread of the virus, and at lower cost, and for how best to “restart” the economy.
First, however, lets dispense with the absolutist position that there can be no compromise on virus mitigation in favor of economic activity. I am not opposed to the “lockdown” we are now living, but it will have significant and unnecessary costs if it goes on too long: the lost output is a huge blow not only to our current lifestyles but to our ability to grow in the future, or even to afford better health care in the future. Beyond that, the lockdown has immediate negative impacts of its own on public health: economic stress leads to all kinds of terrible health outcomes like heart disease and even suicide. About the latter, the President is absolutely correct: if you need research to prove it, see here, here, here, and here, all respected journals (the links all courtesy of The Federalist.) Economic stress and isolation is quite likely to promote poor dietary habits, lethargy, and possibly family dysfunction as well. Don’t pretend there aren’t real tradeoffs between the economy, virus interventions, and public health. The trick is to improve those tradeoffs. A balance can and must be struck, and depending on policy actions, the tradeoff can be made better or worse.
Back to the virus reproduction rate: the R0 values we see quoted are estimates of the average number of other people infected by each infected person. A value of three means that each person infected with the virus passes it on to three others, on average. If R0 is greater than one, an epidemic grows. If R0 is less than one, a contagion recedes. It becomes a “non-epidemic” if R0 remains less than one. It does not have to be zero (and probably cannot be zero).
But not everyone is the same: my R0 is different from your R0 if only because we have different occupational exposure to others and different levels of social engagement. We also differ physiologically, which probably leads to differences in our “personal” R0 values. And an individual’s R0 will differ by time and place, depending on random circumstances like which way the wind is blowing. But here is where it gets interesting. Cochrane describes an extreme version of the skewed distribution shown at the top of this post:
“Suppose there are 100 people with a 0.5 reproduction rate, and 1 super-spreader with a 100 replication rate. The average reproduction rate is 1.5. Clearly, locking everyone down is wildly inefficient. It’s much more important to find the 1 super-spreader and lock him or her down, or change the business or behavior that’s causing the super-spreading.
This is exaggerated, but not far off the mark. I have not seen numbers on the distribution of reproduction rates across people, but it is a fair bet that it has an extremely fat tail. Most of us are washing our hands, social distancing, work in businesses that are shut down or are taking great steps to limit contact. And a few people and activities contribute to most of the spread.
This wide and fat-tailed dispersion is ignored in a lot of simulations I’ve seen. They take the average reproduction rate as the same for everyone. That’s a big mistake.
The danger: we waste a huge amount of time and money moving you and me from a 0.5 reproduction rate to an 0.4 reproduction rate. … The opportunity: focus on the super-spreaders, and the super-spreading activities, and you bring down the reproduction rate at much lower cost. “
There are many ways to reduce R0. Cochrane gets a little more specific about this and the policy implications of the skewed R0 distribution across individuals:
“All we need is to get the transmission rate under one. Activities with possible but very low transmission rates, and high economic benefits should go on. Don’t separate to ‘essential’ and ‘non-essential.’ Separate into ‘high likelihood of transmission’ and ‘low likelihood of transmission.’
Why are we not using masks everywhere? Sure, they’re not perfect. Sure, an old hankerchief might only cut the chance of transmission by half. We’re not all surgeons. Cutting by half is enough to stop the virus.
Conversely, why did they close the state parks? Really? Just how dangerous is it to drive the dog to a hiking trail and stay 6 feet away from other people? Parks, ski areas, golf courses, all sorts of businesses that surely can be run with a reproduction rate far less than one are just shut down. I met a realtor on our dog walk yesterday. They’re totally shut down. Just how hard is it to run a realty business with a 0.5 reproduction rate? One family in the house at a time, don’t touch anything, an hour between showings, stay 6 feet from the realtor… But instead the whole business is just shut down.”
The beginning of that last paragraph echoes a point I made in my last post about public park closures and the health benefits of getting outside generally.
Cochrane goes on to discuss several other policy options, including the potential benefits of simple kinds of testing and the overemphasis on false negatives and positives in policy discussions. Imperfect tests should not be discouraged by these concerns. If you’re worried about that, you shouldn’t use a thermometer either!
“Stay-at-home” or “shelter-in-place” orders will increasingly be tested by private parties if they remain in effect too long. That will be encouraged by the seemingly arbitrary distinctions some orders make between “essential” and “non-essential” activities. If workers or small businessmen judge themselves to be at low risk, they will take matters into their own hands to the extent they can. I believe that’s already happening where the specifics of “lockdown” orders have gone too far. Workers at the low end of the income spectrum are especially hard hit by these orders. One can hardly blame them for trying to earn what they can if they believe, and their customers believe, their activities and interactions are of low risk.
Ultimately, the entire distribution of R0s will slide to the left. That will occur even at low levels of “herd immunity” and anything that offers at least weak prophylaxis. Broadly speaking, the latter includes maintaining distance, refusing admittance to venues with a fever, avoiding handshakes, wearing masks, and potentially chloroquine, which is already in widespread use by physicians treating coronavirus patients. Ultimately, a vaccine will slide the distribution far to the left, but the economy need not be held hostage until that time. To paraphrase Cochrane, we can get the transmission rate below one and keep it there without stopping the world permanently. There are many options, and now is the time for business and government to start planning for that.
In advanced civilizations the period loosely called Alexandrian is usually associated with flexible morals, perfunctory religion, populist standards and cosmopolitan tastes, feminism, exotic cults, and the rapid turnover of high and low fads---in short, a falling away (which is all that decadence means) from the strictness of traditional rules, embodied in character and inforced from within. -- Jacques Barzun