Tags
Alex Tabarrok, Case Fatality Rate, CDC, CLI, Convalescent Plasma, Covid-19, COVID-Like Illness, Date of Death, Herd Immunity, Herd Immunity Threshold, Infection Fatality Rate, Ivermectin, Johns Hopkins, Monoclonal Antibodies, Phil Kerpen, Provisional Deaths, South African Strain, UK Strain, Vaccinations, Youyang Gu
The pandemic outlook remains mixed, primarily due to the slow rollout of the vaccines and the appearance of new strains of the virus. Nationwide, cases and COVID deaths rose through December. Now, however, there are several good reasons for optimism.
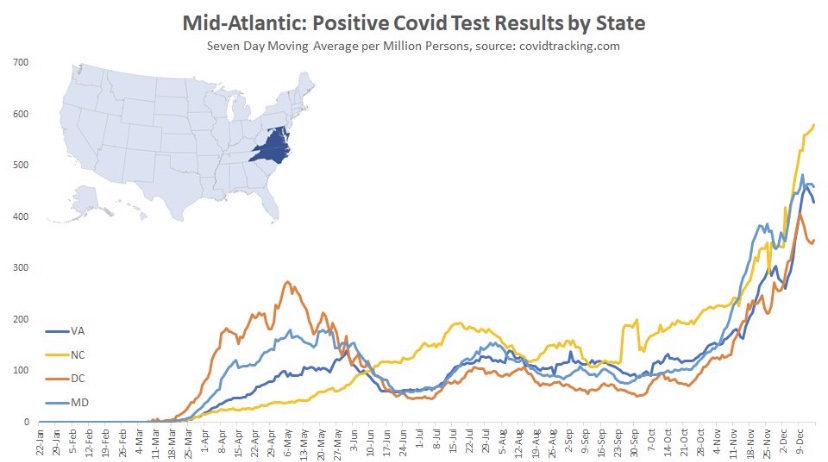
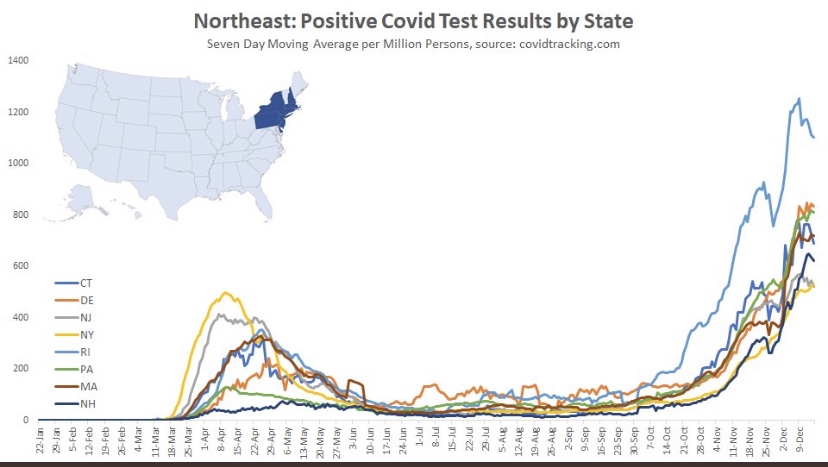
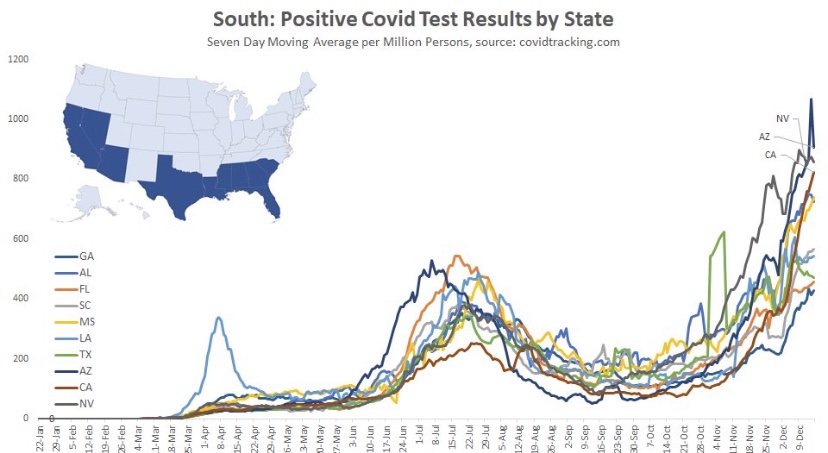
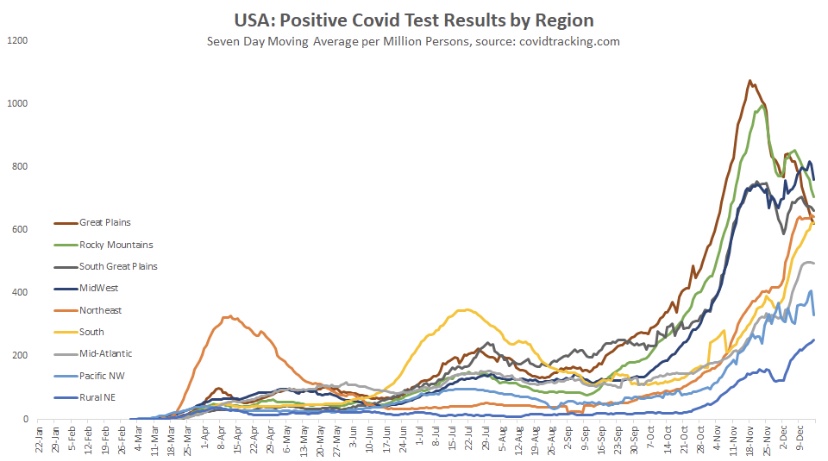
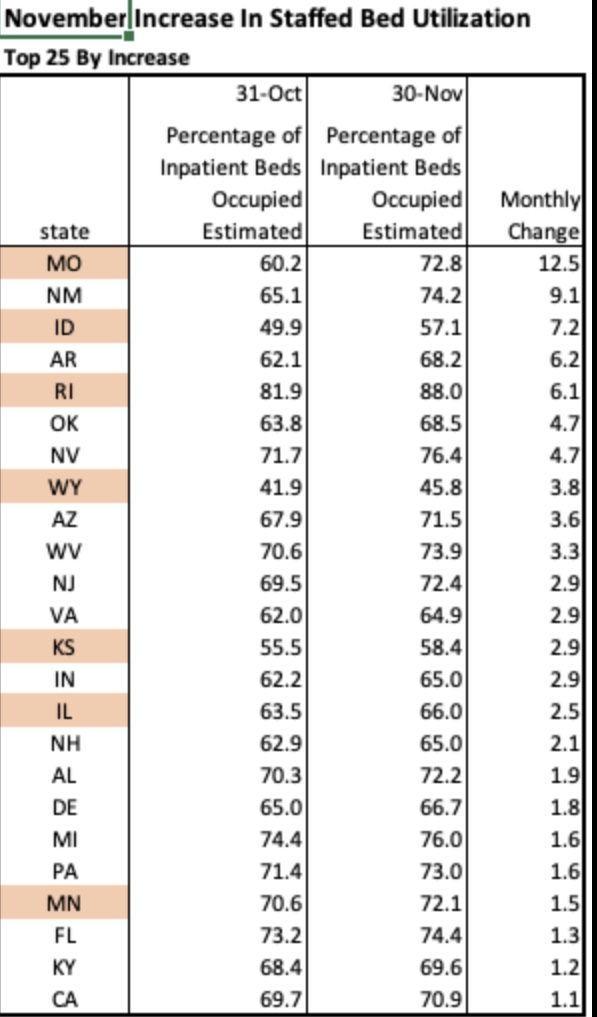
The fall wave of the coronavirus receded in many states beginning in November, but the wave started a bit later in the eastern states, in the southern tier of states, and in California. It appears to have crested in many of those states in January, even after a post-holiday bump in new diagnoses. As of today, Johns Hopkins reports only two states with increasing trends of new cases over the past two weeks: NH and VA, while CT and WY were flat. States shaded darker green have had larger declines in new cases.

A more detailed look at WY shows something like a blip in January after the large decline that began in November. Trends in new cases have clearly improved across the nation, though somewhat later than hoped.
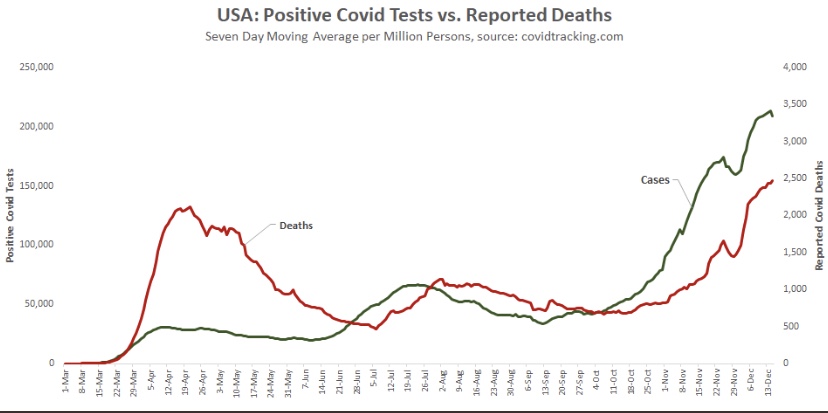
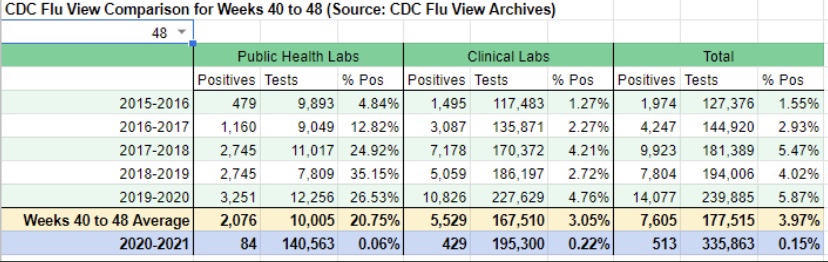
While the fall wave has taken many lives, we can take some solace in the continuing decline in the case fatality rate. (This is not the same as the infection mortality rate (IFR), which has also declined. The IFR is much lower, but more difficult to measure). The CFR fell by more than half from its level in the late summer. In other words, without that decline, deaths today would be running twice as high.
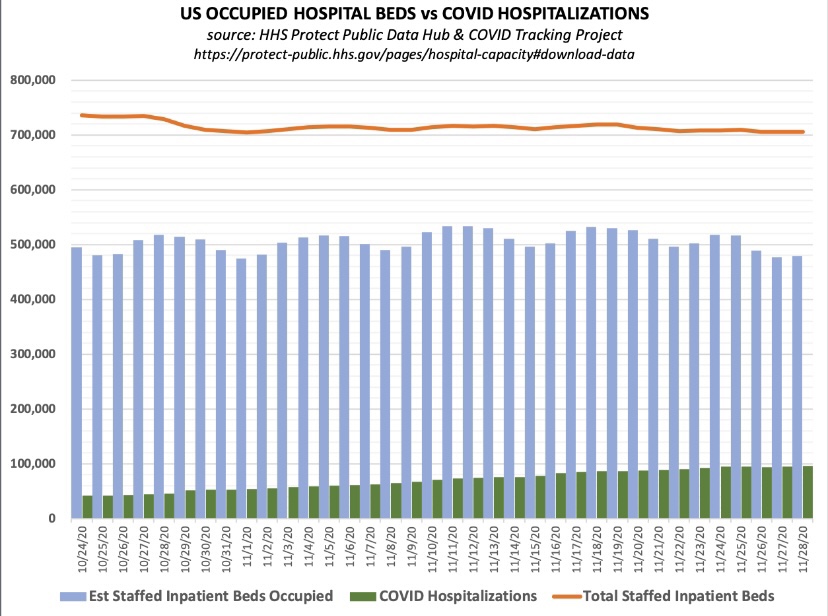
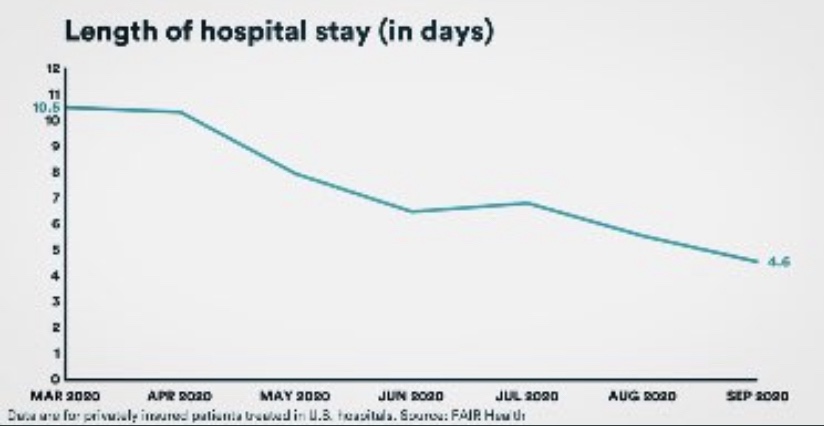
Some of the CFR’s decline was surely due to higher testing levels. However, better treatments are reducing the length of hospital stays for many patients, as well as ICU admittance and deaths relative to cases. Monoclonal antibodies and convalescent plasma have been effective for many patients, and now Ivermectin is showing great promise as a treatment, with a 75% reduction in mortality according to the meta-analysis at the link.

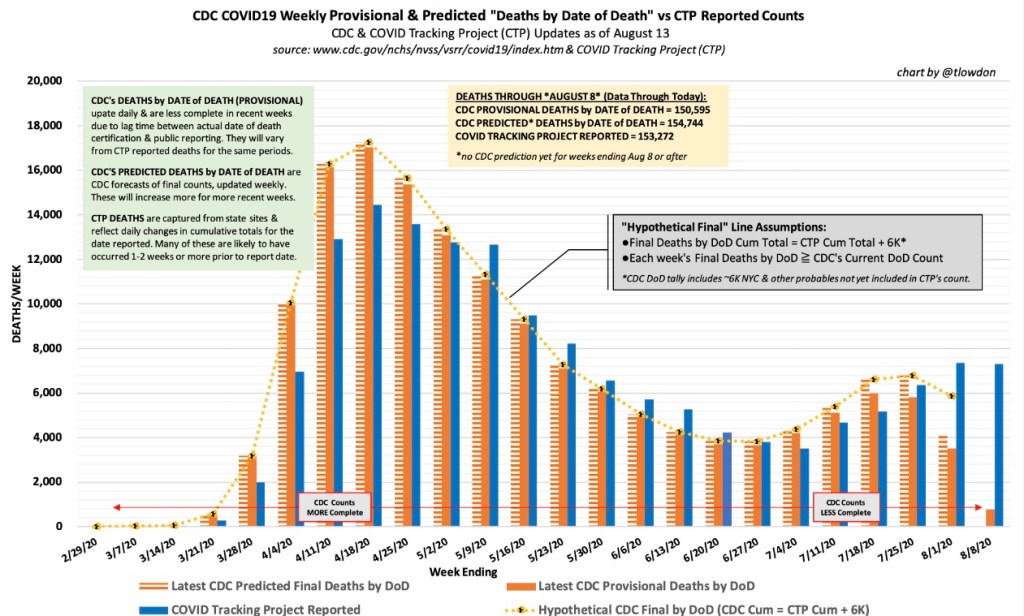
Reported or “announced” deaths remain high, but those reports are not an accurate guide to the level or trend in actual deaths as they occur. The CDC’s provisional death reports give the count of deaths by date of death (DOD), shown below. The most recent three to four weeks are very incomplete, but it appears that actual deaths by DOD may have peaked as early as mid-December, as I speculated they might last month. Another noteworthy point: by the totals we have thus far, actual deaths peaked at about 17,000 a week, or just over 2,400 a day. This is substantially less than the “announced” deaths of 4,000 or more a day we keep hearing. The key distinction is that those announced deaths were actually spread out over many prior weeks.

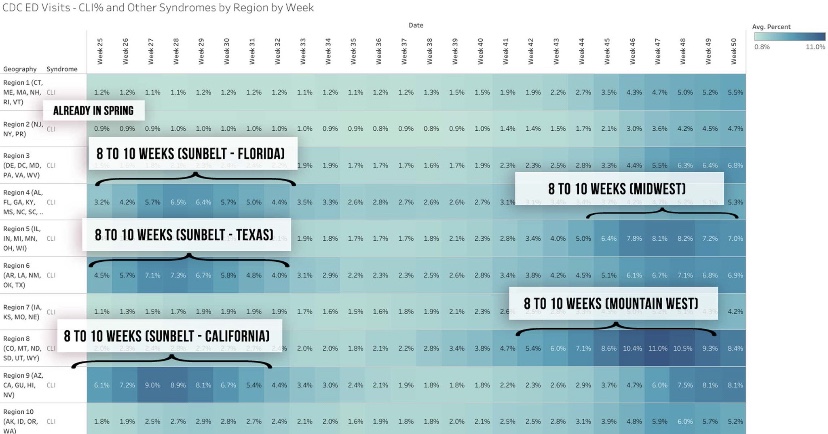
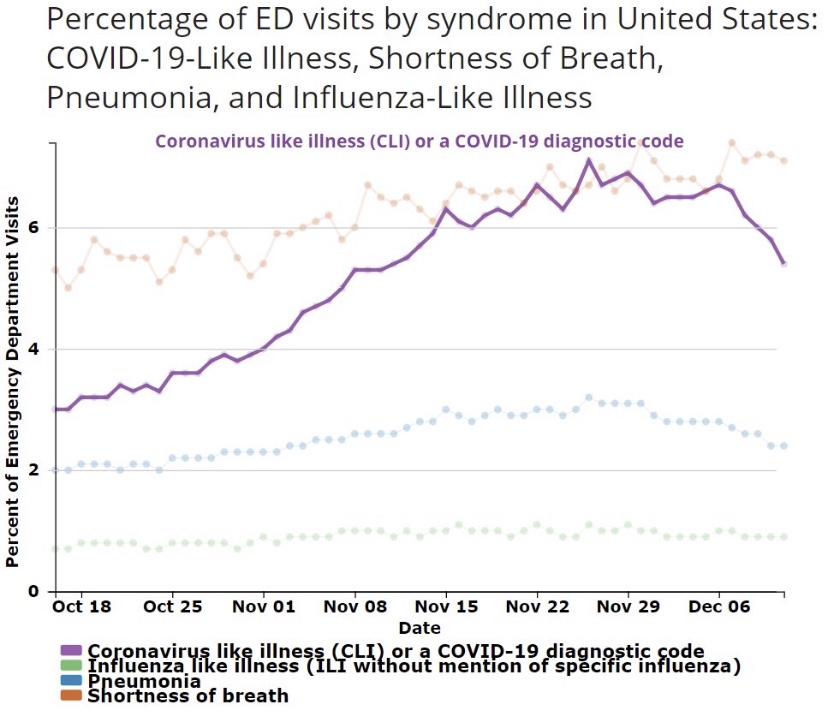
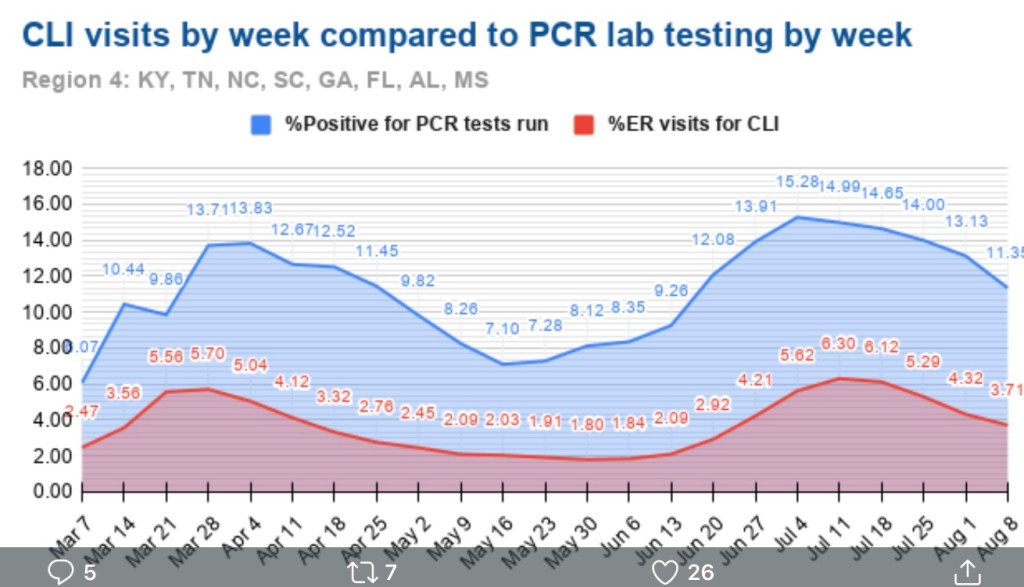
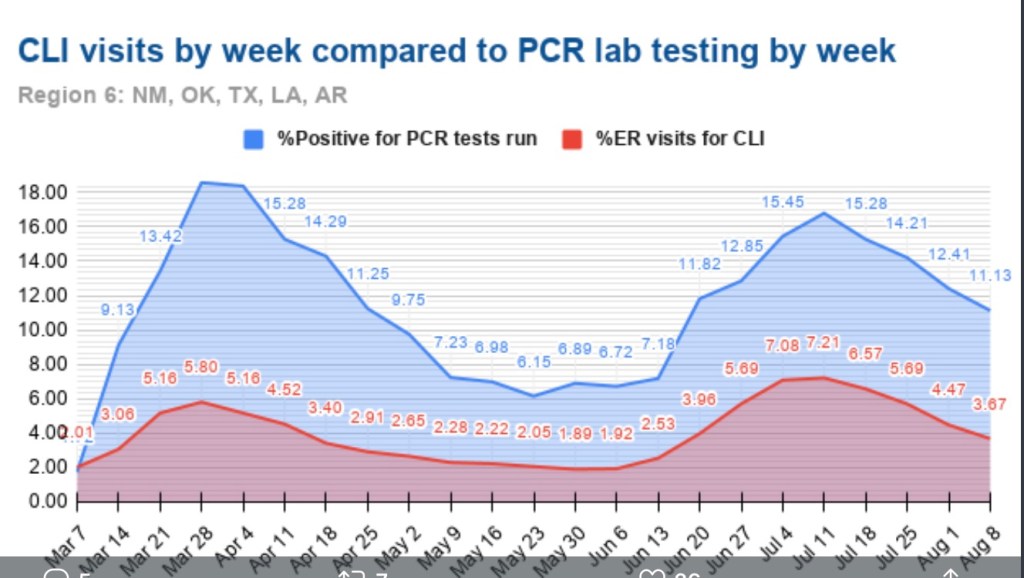
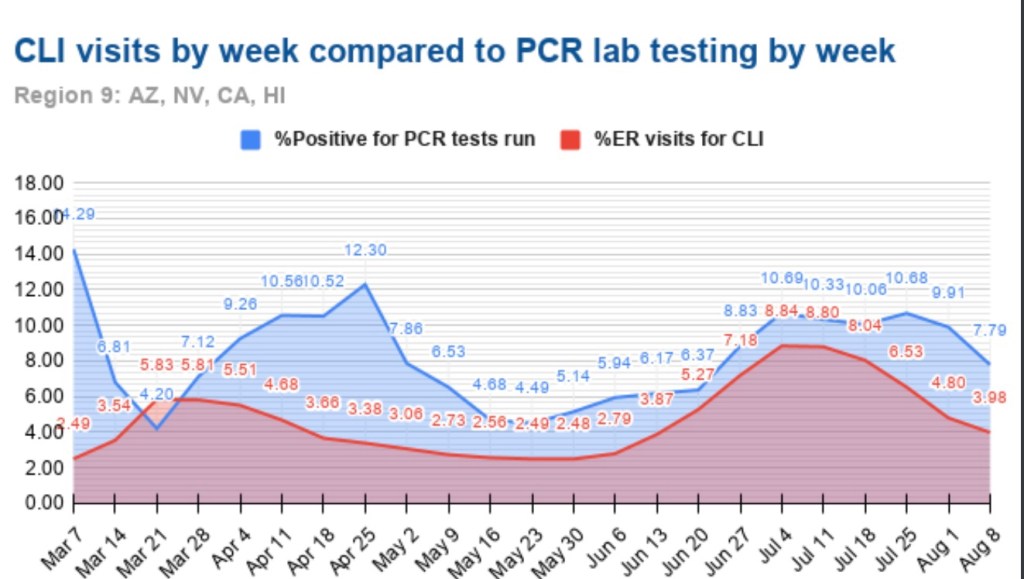
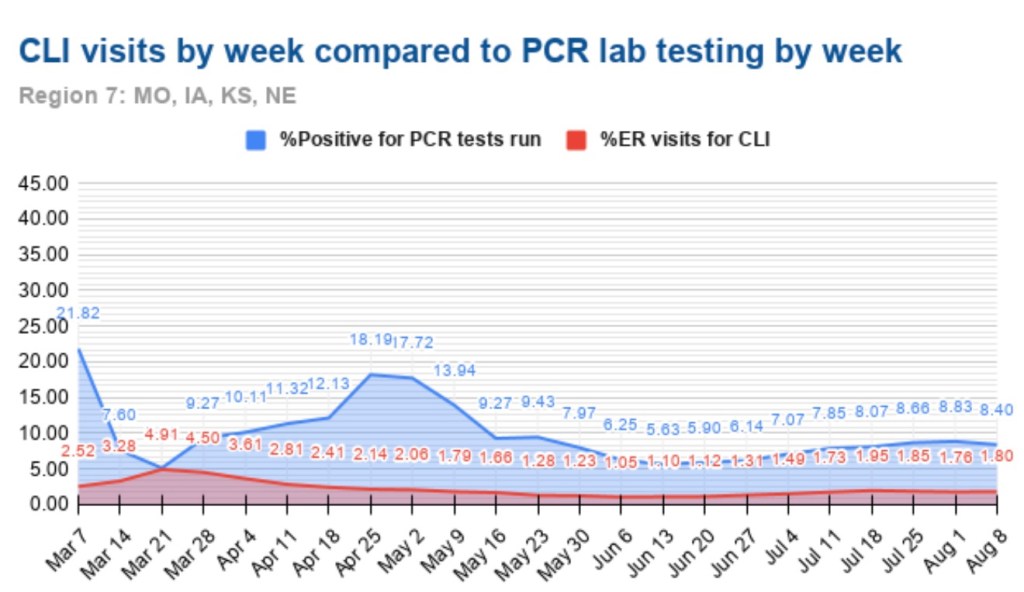
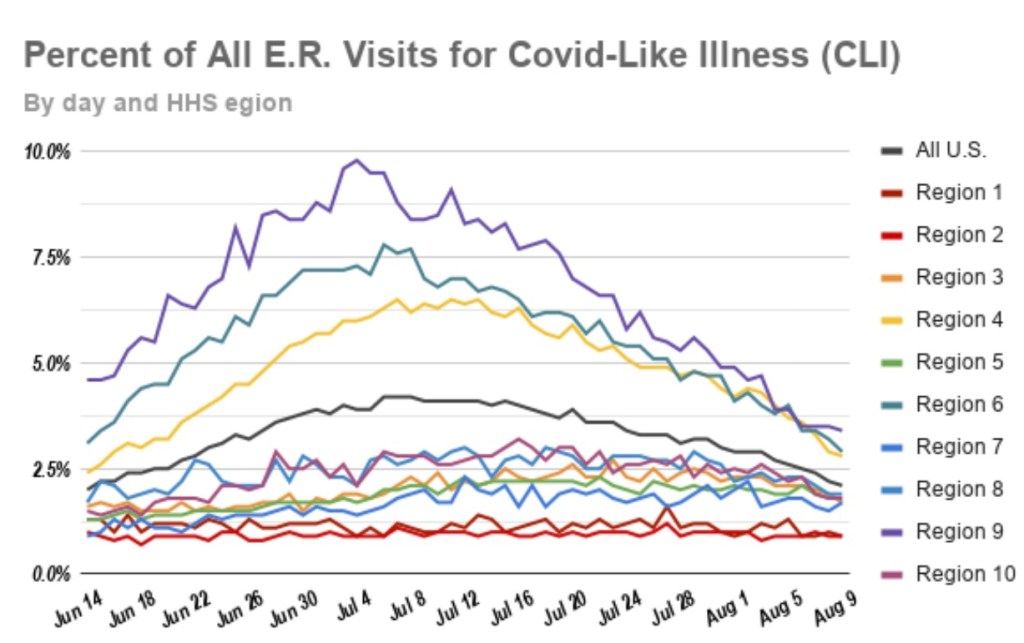
A useful leading indicator of actual deaths has been the percentage of ER patients presenting COVID-like illness (CLI). The purple dots in the next CDC chart show a pronounced decline in CLI over the past three weeks. This series has been subject to revisions, which makes it much less trustworthy. A less striking decline in late November subsequently disappeared. At the time, however, it seemed to foretell a decline in actual deaths by mid-December. That might actually have been the case. We shall see, but if so, it’s possible that better therapeutics are causing the apparent CLI-deaths linkage to break down.

A more recent concern is the appearance of several new virus strains around the world, particularly in the UK and South Africa. The UK strain has reached other countries and is now said to have made appearances in the U.S. The bad news is that these strains seem to be more highly transmissible. In fact, there are some predictions that they’ll account for 30% of new cases by the beginning of March. The South African strain is said to be fairly resistant to antibodies from prior infections. Thus, there is a strong possibility that these cases will be additive, and they might or might not speedily replace the established strains. The good news is that the new strains do not appear to be more lethal. The vaccines are expected to be effective against the UK strain. It’s not yet clear whether new versions of the vaccines will be required against the South African strain by next fall.
Vaccinations have been underway now for just over a month. I had hoped that by now they’d start to make a dent in the death counts, and maybe they have, but the truth is the rollout has been frustratingly slow. The first two weeks were awful, but as of today, the number of doses administered was over 14 million, or almost 46% of the doses that have been delivered. Believe it or not, that’s an huge improvement!

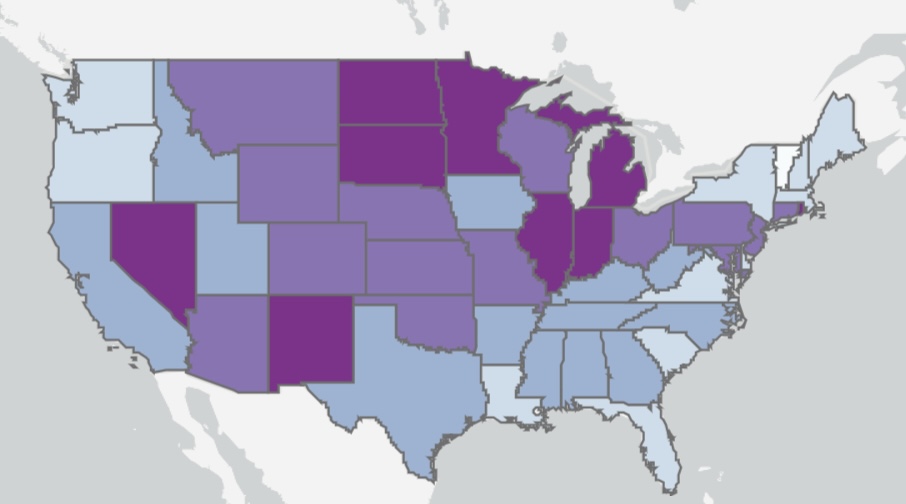
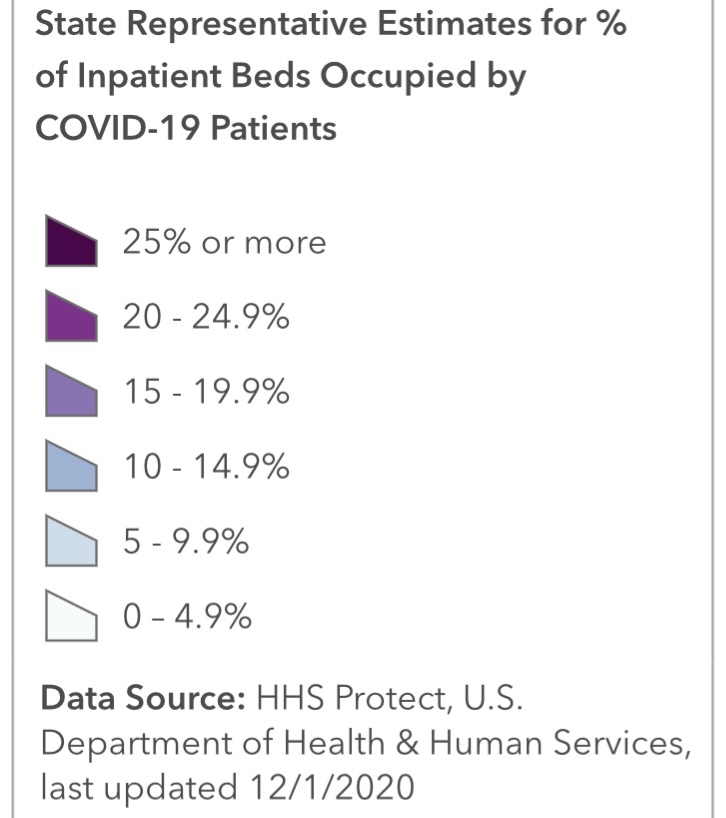
About 4.3% of the population had received at least one dose as of today, according to the CDC. I have no doubt that heavier reliance on the private sector will speed the “jab rate”, but rollouts in many states have been a study in ineptitude. Even worse, now a month after vaccinations began, the most vulnerable segment of the population, the elderly, has received far less than half of the doses in most states. The following table is from Phil Kerpen. Not all states are reporting vaccinations by age group, which might indicate a failure to prioritize those at the greatest risk.

It might not be fair to draw strong conclusions, but it appears WV, FL, IN, AK, and MS are performing well relative to other states in getting doses to those most at risk.
Even with the recent increase in volume, the U.S. is running far behind the usual pace of annual flu vaccinations. Each fall, those average about 50 million doses administered per month, according to Alex Tabarrok. He quotes Youyang Gu, an AI forecaster with a pretty good track record thus far, on the prospects for herd immunity and an end to the pandemic. However, he uses the term “herd immunity” as the ending share of post-infected plus vaccinated individuals in the population, which is different than the herd immunity threshold at which new cases begin to decline. Nevertheless, in Tabarrok’s words:
“… the United States will have reached herd immunity by July, with about half of the immunity coming from vaccinations and half from infections. Long before we reach herd immunity, however, the infection and death rates will fall. Gu is projecting that by March infections will be half what they are now and by May about one-tenth the current rate. The drop will catch people by surprise just like the increase. We are not good at exponentials. The economy will boom in Q2 as infections decline.”
That sounds good, but Tabarrok also quotes a CDC projection of another 100,000 deaths by February. That’s on top of the provisional death count of 340,000 thus far, which runs 3-4 weeks behind. If we have six weeks of provisionals to go before February, with actual deaths at their peak of about 17,000 per week, we’ll get to 100,000 more actual deaths by then. For what it’s worth, I think that’s pessimistic. The favorable turns already seen in cases and actual deaths, which I believe are likely to persist, should hold fatalities below that level, and the vaccinations we’ve seen thus far will help somewhat.