Tags
@tlowdon, Antibodies, CDC, COVID Deaths, Covid Tracking Project, COVID-Like Illness, ER Patient Symptoms, FiveThirtyEight, Flu Season, Herd Immunity, Humidity, Influenza-Type Illness, Iowa State, MIT, Predictive Models, Provisional Deaths, Seroprevalence, UCLA, University of Texas, Vitamin D
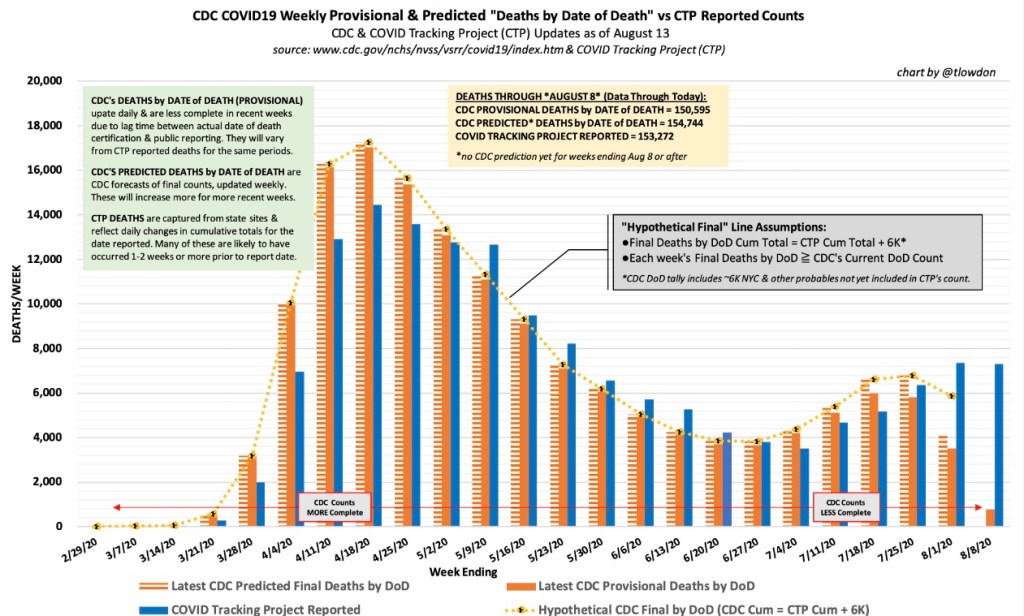
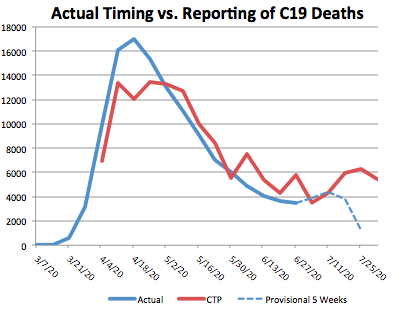
Reported COVID deaths do not reflect deaths that actually occurred in the reporting day or week, as I’ve noted several times. Here is a nice chart from @tlowdon on Twitter showing the difference between reported deaths and actual deaths for corresponding weeks. The blue bars are weekly deaths reported by the COVID Tracking Project. The solid orange bars are the CDC’s “provisional” deaths by actual week of death, which is less than complete for recent weeks because of lags in reporting. Still, it’s easy to see that reported deaths have overstated actual deaths each week since late August.

I should note that the orange bars represent deaths that involved COVID-19, though a COVID infection might not have actually killed them. This CDC report, updated on November 4th, shows the importance of co-morbidities, which in many cases are the actual cause of death according to pre-COVID, CDC guidance on death certificates.
Leading Indicators
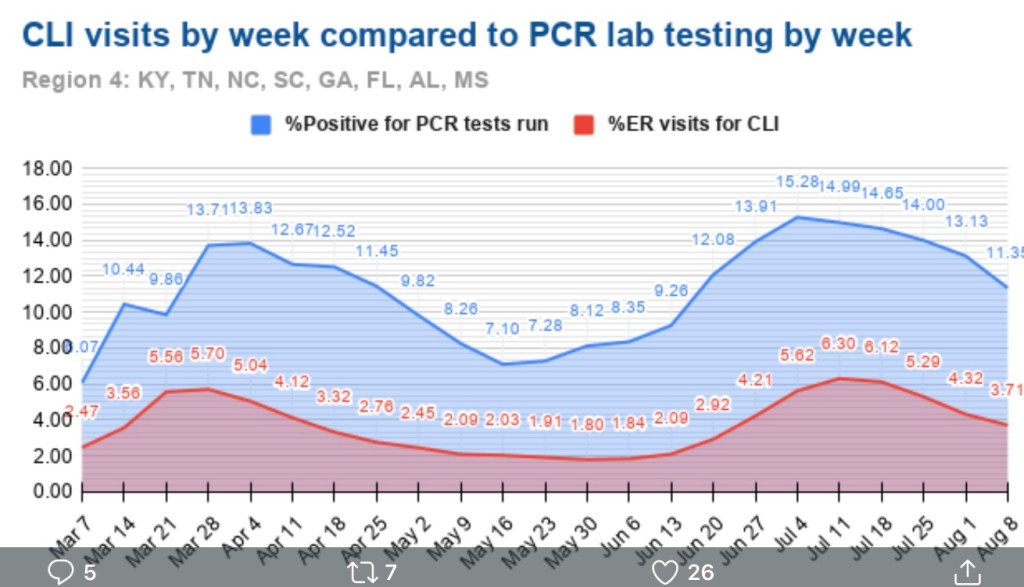
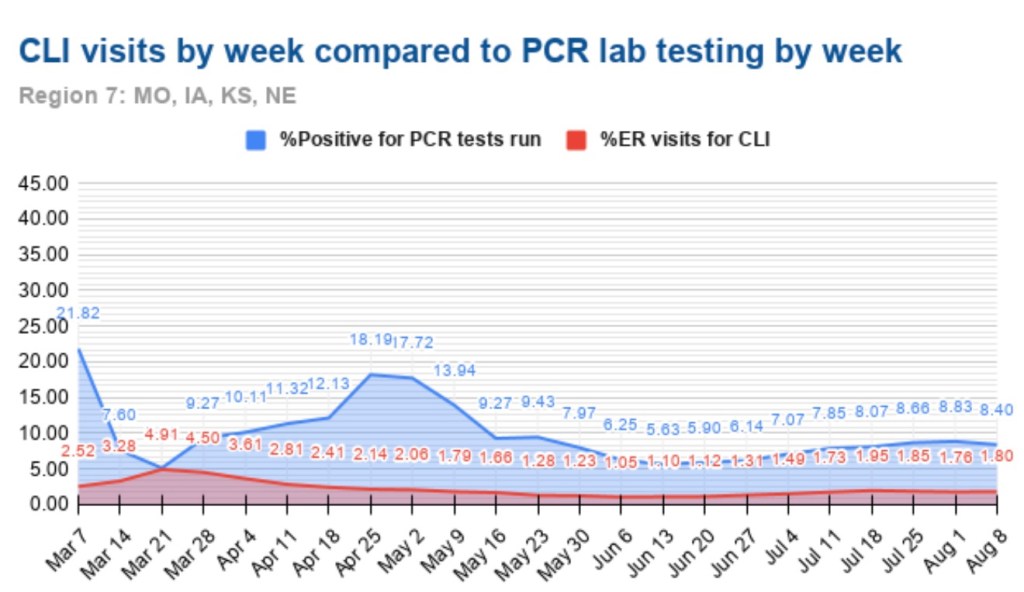
Researchers have studied several measures in an effort to find leading indicators of COVID deaths. The list includes new cases diagnosed (PCR positivity) and the percentage of emergency room visits presenting symptoms of COVID-like illness (%CLI). These indicators are usually evaluated after shifting them in time by a few weeks in order to observe correlations with COVID deaths a few weeks later. Interestingly, @tlowdon reports that the best single predictor of actual COVID deaths over the course of a few weeks is the sum of the %CLI and the percentage of ER patients presenting symptoms of influenza-like illness (%ILI). Perhaps adding %ILI to %CLI strengthens the correlation because the symptoms of the flu and COVID are often mistaken for one another.
The chart below reproduces the orange bars from above representing deaths at actual dates of death. Also plotted are the %Positivity from COVID tests (shifted forward 2 weeks), %CLI (3 weeks), the %ILI (3 weeks), and the sum of %CLI and %ILI (3 weeks, the solid blue line). My guess is that %ILI contributes to the correlation with deaths mainly because %ILI’s early peak (which occurred in March) led the peak in deaths in April. Otherwise, there is very little variation in %ILI. That might change with the current onset of the flu season, but as I noted in my last post, the flu has been very subdued since last winter.

What About November?
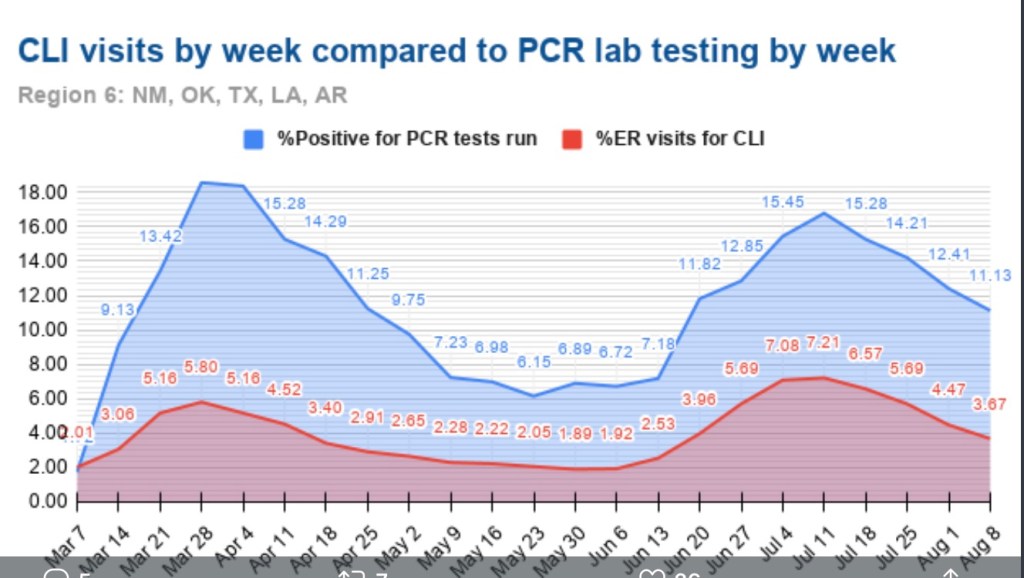
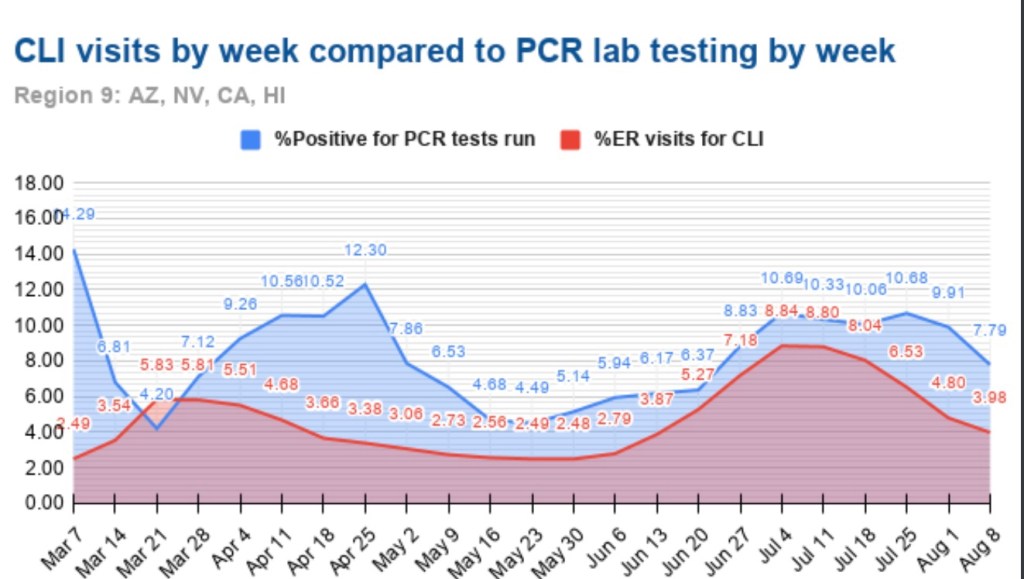
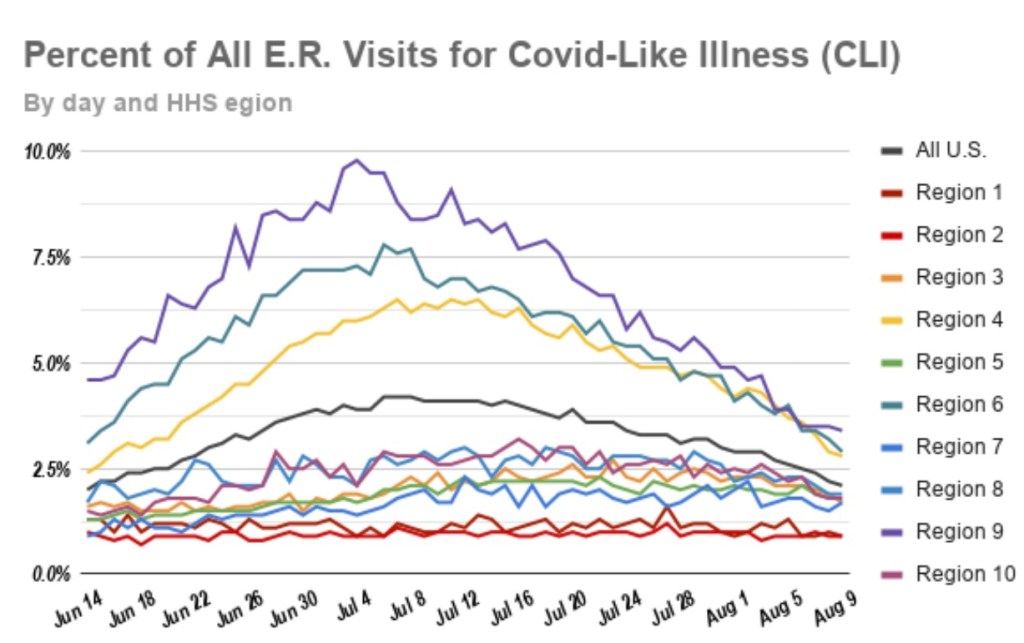
So where does that leave us? The chart above ends with our leading indicator, CLI + ILI, brought forward from the first half of October. What’s happened to CLI + ILI since then? And what does that tell us to expect in November? The chart below is from the CDC’s web site. The red line is %CLI and the yellow line is %ILI. The sum of the two isn’t shown. However, there is no denying the upward trend in CLI, though the slope of CLI + ILI would be more moderate.

As of 10/31, CLI + ILI has increased by almost 40% since it’s low in early October. If the previous relationship holds up, that implies an increase of almost 40% in actual weekly COVID deaths from about 4,000 per week to about 5,500 per week by November 21 (a little less than 800 per day).
FiveThirtyEight has a compilation of 13 different forecast models with projections of deaths by the end of November. The estimate of 5,500 per week by November 21, or perhaps slightly less per week over the full month of November, would put total COVID deaths at the top of the range of the MIT, UCLA, Iowa State, and University of Texas models, but below or near the low end of ranges for eight other models. However, those models are based on reported deaths, so the comparison is not strictly valid. Reported deaths are still likely to exceed actual deaths by the end of November, and the actual death prediction would be squarely in the range of multiple reported death predictions. That reinforces the expectation an upward trend in actual deaths.
Third Wave States
States in the upper Midwest and upper Mountain regions have had the largest increases in cases per capita over the past few weeks. Using state abbreviations, the top ten are ND, SD, WI, IA, MT, NE, WY, UT, IL, and MN, with ID at #11 (according to the CDC’s COVID Data Tracker). One factor that might mediate the increase in cases, and ultimately deaths, is the possibility of early herd immunity: in the earlier COVID waves, the increase in infections abated once seroprevalence (the share of the population with antibodies from exposure) reached a level of 15% to 25%.
Unfortunately, estimates of seroprevalence by state are very imprecise. Thus far, reliable samples have been limited to states and metro areas that had heavy infections in the first and second waves. One rule of thumb, however, is that seroprevalence is probably less than 10x the cumulative share of a population having tested positive. To be very conservative, let’s assume a seroprevalence of four times cumulative cases. On that basis, half the states in the “top ten” listed above would already have seroprevalence above 15%. Those states are ND, SD, WI, IA, and NE. The others are mostly in a range of 12% to 15%, with MI coming in the lowest at about 9%.
This gives some cause for optimism that the wave in these states and others will abate fairly soon, but there are a number of uncertainties: first, the estimates of seroprevalence above, while conservative, are very imprecise, as noted above; second, the point at which herd immunity might cause the increase in new cases to begin declining is real guesswork (though we might have confirmation in a few states before long); third, we are now well into the fall season, with lower temperatures, lower humidity, less direct sunlight, and diminishing vitamin D levels. We do not have experience with COVID at this time of year, so we don’t know whether the patterns observed earlier in the year will be repeated. If so, new cases might begin to abate in some areas in November, but that probably wouldn’t be reflected in deaths until sometime in December. And if the flu comes back with a corresponding increase in CLI + ILI, then we’d expect further increases in actual deaths attributed to COVID. That is only a possibility given the weakness in flu numbers in 2020, however.
Closing Thoughts
I was excessively optimistic about the course of the pandemic in the U.S. in the spring. While this post has been moderately pessimistic, I believe there are reasons to expect fewer deaths than previous relationships would predict. We are far better at treating COVID now, and the vulnerable are taking precautions that have reduced their incidence of infections relative to younger and healthier cohorts. So if anything, I think the forecasts above will err on the high side.