The policies foisted upon the country by the Left always hurt those constituencies they think they’ll help, and they backfire in very predictable ways. There are too many instances of that truism to recount, but just a couple of examples follow.
Economic Perils of Precaution
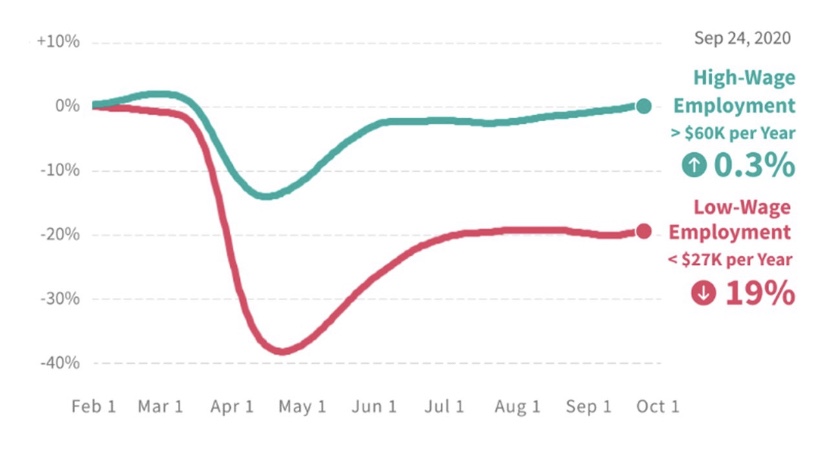
We can start with the interminable non-pharmaceutical interventions (NPIs) imposed in many states during the pandemic. These included shelter-at-home orders, limits on public gatherings, school closures, and the like. These lockdown measures were more severe in so-called blue states controlled by the Democrat Party. But NPIs were a policy failure and did little to stem the pandemic or excess deaths. Moreover, they resulted in the closure of many businesses and massive job losses. The economic burden fell especially hard on low wage earners, as the following chart shows:
For high earners (the red line), the employment decline at the start of the pandemic was small and relatively brief. Less fortunate were those earning under $27,000 annually (the blue line). They suffered a much larger initial decline in employment and had a continuing loss of almost 24% of jobs. While those who lost jobs ultimately received enhanced unemployment compensation and other benefits, the idleness and loss of work experience inflicted long-term damage to health, psyches, and future prospects. Thus, the party with pretensions of championing the cause of the downtrodden was pleased to intervene with policies that undercut the working poor.
But Some Precautions Are “Racist”
Another prominent case in which leftists have harmed those for whom they claim to advocate is the effort to “defund the police”. Low income and minority populations do not favor such a policy because they understand the value of protection against criminal elements who victimize their communities. The residents of these communities are most at risk from gangland violence and homicide. Furthermore, nearly all “victims” of police homicides are armed, and police homicides are closely associated with crime. And again, the sad fact is that crime is heavily concentrated in minority neighborhoods. The statistics do not support assertions of bias in policing. Obviously, these citizens have taken notice that the riots cheered on by the Left have been destructive to their communities.
Crime has spiked in Minneapolisand elsewhere since last summer, when George Floyd’s death sparked interest in the “defund the police” mantra promoted by the Left. And there followed a reduction in police budgets of about 5.2% in aggregate in the 50 largest cities in the country (though not all of these cities made cuts). Moreover, the effectiveness of policing has been undercut more broadly by the substantial legal risk now facing officers who earnestly attempt to enforce the law, as well as more restrictive use-of-force policies.
These changes are an unambiguous disaster for so many good people having the misfortune to live in high-crime areas. And the political disaster is starting to sink in among Democrats, who are already attempting to change the narrative (and seehere). It’s pretty transparent that the “black lives matter” dialectic appeals to Democrats primarily as a selling point of convenience, and not so much when there’s actual blood in the streets.
Only the Obvious Matters
Destructive lockdowns and efforts to “defund the police” are just two examples of a perverse phenomenon. It’s well known to keen observers of the history of Marxism in action that it usually victimizes its presumed beneficiaries. That dynamic is at play under school discipline policies that seek to avoid “disparate impacts” on minority students, leaving other minority school children in disruptive learning environments; gun control initiatives making it difficult for minority residents and businesses to protect themselves; rent controls leading to a deteriorating stock of low-cost housing; wage floors causing low-skilled workers to lose hours, benefits, and jobs; energy policies with regressive impacts on household budgets; tax policies destroying incentives for job creation; and a welfare state creating disincentives to work and promoting family instability. This list goes on and on.
The difficulty leftists have in coming to grips with these unintended consequences is that they can’t see past first-order effects. Like spoiled children, they grasp only the ostensible benefits of their demands. And like bad parents, they behave as if to seek approval of the most spoiled among their presumed charges.
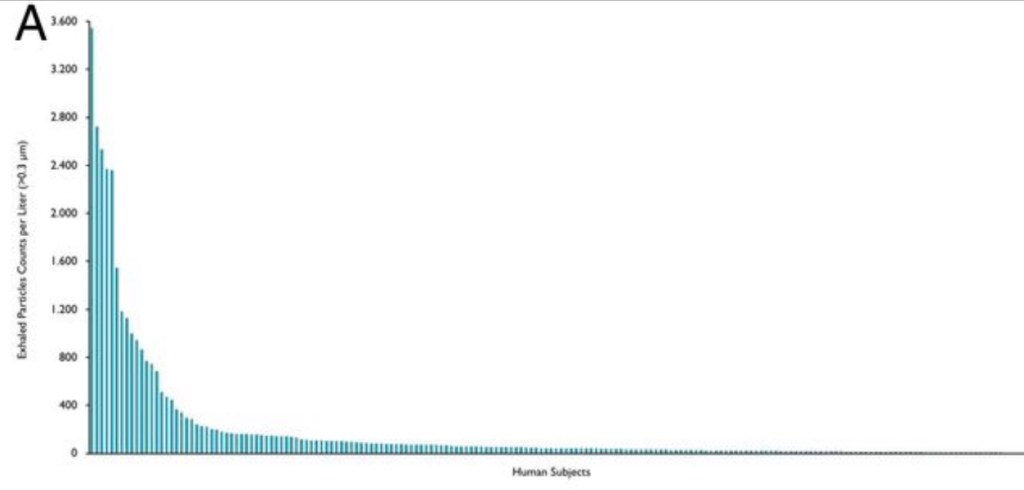
Super-spreading events are gatherings at which one or more attendees are already harboring an infection and manage to transmit it to a number of others. These people, in turn, spread it to their close contacts, possibly at the same event. Super-spreading has dominated the transmission of COVID-19. These transmissions have almost always taken place indoors in spaces with limited ventilation, and they have usually involved close or prolonged contact. In addition, super-spreading originates with a small subset of infected individuals. That’s essentially what the chart above shows. It ranks individual subjects by their exhaled quantity of aerosolized particles per liter of air.
For more than a year, we’ve also known that obesity and age are associated with more severe COVID infections. Now, it’s startling to learn that obese and/or older, infected individuals are more prone to transmitting virus: this study found that a high body mass index (BMI) is associated with significantly greater quantities of exhaled aerosol, and that age has a similarly strong association. So called BMI-years, or age x BMI, has an extremely powerful association with the exhalation of aerosol-borne particles. The authors, David A. Edwards, et al, believe this is a consequence of the properties of mucus produced by different individuals in response to infections and how their lungs and airways handle it. The authors say:
“Our findings indicate that the capacity of airway lining mucus to resist breakup on breathing varies significantly between individuals, with a trend to increasing with the advance of COVID-19 infection and body mass index multiplied by age (i.e., BMI-years). Understanding the source and variance of respiratory droplet generation, and controlling it via the stabilization of airway lining mucus surfaces, may lead to effective approaches to reducing COVID-19 infection and transmission. … ”
“Surfactant and mucin compositional and structural changes, driven, in part, by physiological alterations of the human condition—including diet (10), aging (11), and COVID-19 infection itself (12)—may therefore be anticipated to alter droplet generation and droplet size (7) during acts of breathing.”
So there is substantial variation in the exhalation of aerosol-borne particles across individuals. In the study, less than 20% of healthy subjects produced more than 156 particles per liter of air, accounting for 80% of the exhaled particles. This defined their so-called “super-spreader” cohort. The association of BMI-years and exhaled particles was less pronounced but still positive within the “low-spreader” cohort.
Edwards, et al speculate that these fine droplets might help explain the greater severity of COVID infections among the elderly and obese. Not only does the breakup of mucus into tiny droplets cause these individuals to exhale aerosols more profusely, it probably also leads to deep penetration into their lung tissue.
This knowledge might be broadly applicable to infectious diseases, and SARS viruses in particular. The elderly know they are vulnerable. It’s not clear that the obese have viewed themselves as vulnerable, but they should, even in the age of “body positivity“. And not only are they vulnerable: they appear to pose an elevated hazard to others. I came across a couple of sardonic comments that got right to the apparent elephant in the room: “Instead of a mask mandate, how about a push-up mandate?”; and “Instead of a vaccine passport, how about a BMI passport?”
The debate about how to care for the most vulnerable is ongoing, but the mere mention of regularities like those identified by the study might lead to proposals for coercive policies. But first, a few practical points to bear in mind: 1) while the study identifies a major risk factor for transmission, it must be replicated by others, and there must be research into the underlying reasons for the phenomenon; 2) while the obese and seniors may be more likely to super-spread, not all of them are super-spreaders; and 3) as a matter of policy, how would “super-spreaders” be defined? What would be the cutoff BMIs at various ages? No matter what was decided, restrictive policies predicated on mere statistical associations would involve gross injustices to a large number of individuals.
With the degree of acquired immunity already in the population and fairly widespread voluntary vaccination (since alarmists have scared the bejeezus out of everyone), the whole issue might seem moot. It’s not, however, because COVID-19 is likely to become endemic, the immunities of some individuals might erode more quickly than expected, new and more dangerous variants might arise, and new SARS viruses are likely to emerge with time.
In a pandemic, however, and even without knowing who is infected, it is ethically barbaric to probabilistically isolate classes of individuals, whether based on age, BMI, or anything other than contagious status. The social cost is simply unacceptable. Instead, public health authorities should provide information to those at high risk, facilitate vaccination for those who desire it, and promote rapid, at-home tests. This is essentially a deregulatory agenda relative to the mindless lockdown approaches favored by so many public health experts.
Everyone must balance their own personal risks and rewards. Based on the study of exhaled particles discussed above, some might shun the obese and seniors until the threat has passed. Some of the obese and elderly might shun each other. That might be another regrettable dimension of the costs of a pandemic. On the other hand, perhaps more of us will respond to the unquestionably positive incentives for weight loss, of which we’re almost all aware.
For clarity, start with this charming interpretive one-act on public health policy in 2020. You might find it a little sardonic, but that’s the point. It was one of the more entertaining tweets of the day, from @boriquagato.
A growing body of research shows that stringent non-pharmaceutical interventions (NPIs) — “lockdowns” is an often-used shorthand — are not effective in stemming the transmission and spread of COVID-19. A compendium of articles and preprints on the topic was just published by the American Institute for Economic Research (AEIR): “Lockdowns Do Not Control the Coronavirus: The Evidence”. The list was compiled originally by Ivor Cummins, and he has added a few more articles and other relevant materials to the list. The links span research on lockdowns across the globe. It covers transmission, mortality, and other health outcomes, as well as the economic effects of lockdowns. AIER states the following:
“Perhaps this is a shocking revelation, given that universal social and economic controls are becoming the new orthodoxy. In a saner world, the burden of proof really should belong to the lockdowners, since it is they who overthrew 100 years of public-health wisdom and replaced it with an untested, top-down imposition on freedom and human rights. They never accepted that burden. They took it as axiomatic that a virus could be intimidated and frightened by credentials, edicts, speeches, and masked gendarmes.
The pro-lockdown evidence is shockingly thin, and based largely on comparing real-world outcomes against dire computer-generated forecasts derived from empirically untested models, and then merely positing that stringencies and “nonpharmaceutical interventions” account for the difference between the fictionalized vs. the real outcome. The anti-lockdown studies, on the other hand, are evidence-based, robust, and thorough, grappling with the data we have (with all its flaws) and looking at the results in light of controls on the population.”
We are constantly told that public intervention constitutes “leadership”, as if our well being depends upon behavioral control by the state. Unfortunately, it’s all too typical of research on phenomena deemed ripe for intervention that computer models are employed to “prove” the case. A common practice is to calibrate such models so that the outputs mimic certain historical outcomes. Unfortunately, a wide range of model specifications can be compatible with an historical record. This practice is also a far cry from empirically testing well-defined hypotheses against alternatives. And it is a practice that usually does poorly when the model is tested outside the period to which it is calibrated. Yet that is the kind of evidence that proponents of intervention are fond of using to support their policy prescriptions.
In this case, it’s even worse, with some of the alleged positive effects of NPI’s wholly made-up, with no empirical support whatsoever! So-called public health experts have misled themselves, and the public, with this kind of fake evidence, when they aren’t too busy talking out of both sides of their mouths.
What does it take to shake people out of their statist stupor? Evidently, the sweet “logic” of universal confinement is very appealing to the prescriptive mindset of busybodies everywhere, who anxiously wag their fingers at those whom they view as insufficiently frightened. As difficult as it is for these shrieking, authoritarian curs to fathom, measures like lockdowns, restrictions on business activity, school closures, and mandates on behavior have at besta limited impact on the spread of the coronavirus, and they are enormously costly in terms of economic well-being and many dimensions of public health. Yet the storm of propaganda to the contrary continues. Media outlets routinely run scare stories, dwelling on rising case numbers but ignoring them when they fall; they emphasize inflated measures of pandemic severity; certain researchers and so-called health experts can’t learn the lessons that are plain in the data; and too many public officials feel compelled to assert presumed but unconstitutional powers. At least the World Health Organization has managed to see things clearly, but many don’t want to listen.
I’ll be the first to say I thought the federalist approach to COVID policy was commendable: allow states and local governments to craft policies appropriate to local conditions and political preferences, rather than have the federal government dictate a one-size-fits-all policy. I haven’t wavered in that assessment, but let’s just say I expected more variety. What I failed to appreciate was the extent to which state and local leaders are captive to provincial busybodies, mavens of precautionary excess, and fraudulent claims to scientific wisdom.
Of course, it should be obvious that the “knowledge problem” articulated by Friedrich Hayek is just as dangerous at low-levels of government as it is in a central Leviathan. And it’s not just a knowledge problem, but a political problem: officials become panicked because they fear bad outcomes will spell doom for their careers. Politicians are particularly prone to the hazards of “do-somethingism”, especially if they have willing, status-seeking “experts” to back them up. But as Scott Sumner says:
“When issues strongly impact society, the science no longer ‘speaks for itself’.
Well, the science is not quite as clear as the “follow-the-science” crowd would have you believe. And unfortunately, public officials have little interest in sober assessments of the unintended effects of lockdown policy.
In my last post, I presented a simple framework for thinking about the benefits and costs of lockdown measures, or non-pharmaceutical interventions (NPIs). I also emphasized the knowledge problem: even if there is some point at which NPI stringencies are “optimized”, government does not possess the knowledge to find that point. It lacks detailed information on both the costs and benefits of NPIs, but individual actors know their own tolerance for risk, and they surely have some sense of the risks they pose to others in their normal course of affairs. While voluntary precautions might be imperfect, they accomplish much of what interventionists hope will be gained via coercion. But, in an effort to “sell” NPIs to constituents and assert their authority, officials vastly over-estimate benefits of NPIs and under-estimate the costs.
NPI Stringency and COVID Outcomes
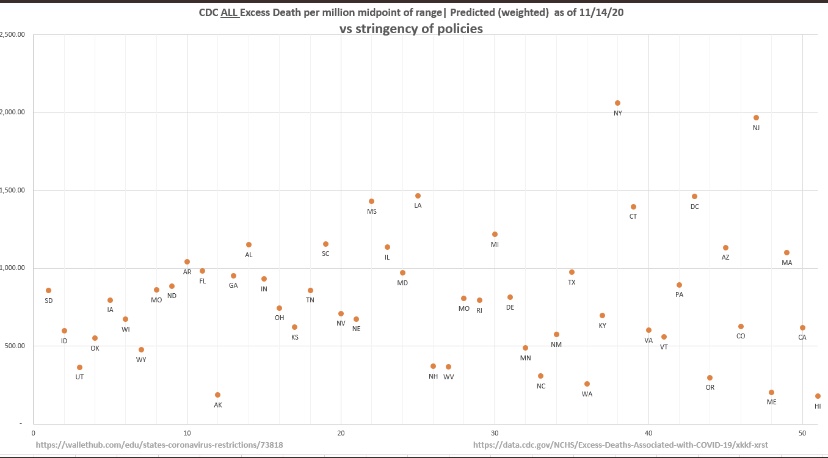
Let’s take a look at a measure of the strength of NPIs by state — the University of Oxford Stringency Index — and compare those to CDC all-cause excess deaths in each state. If it’s hard to read, try clicking on the image or turn your phone sideways. This plot covers outcomes through mid-November:
The chart doesn’t suggest any benefit to the imposition of greater restrictions, or more stringent NPIs. In fact, the truth is that people will do most of the work on their own based on perceptions of risk. That’s partly because government restrictions add little risk mitigation to what can be accomplished by voluntary social distancing and other precautions.
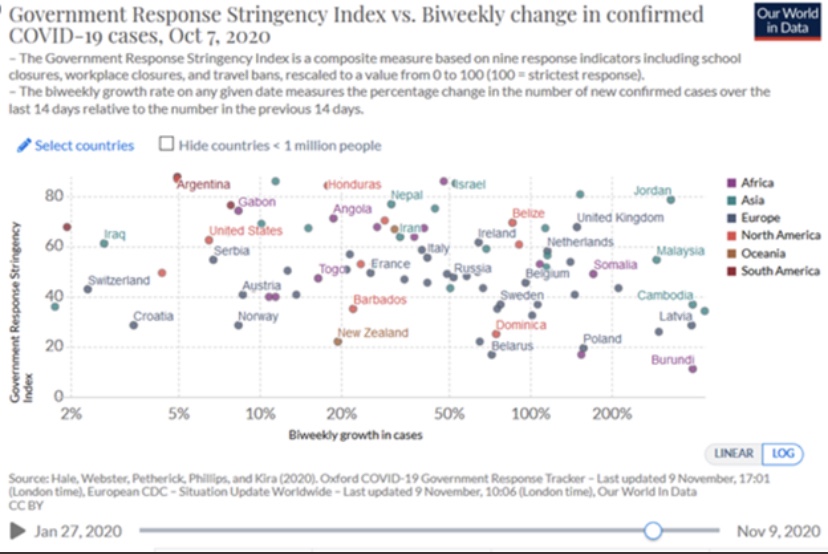
Here’s a similar chart with cross-country comparisons, though the data here ended in early October (I apologize for the fuzzy image):
But what about reverse causality? Maybe the imposition of stringency was a response to more severe contagions. Now that the virus has swept most of the U.S and Europe in three distinct waves, and given the variety and timing of NPIs that have been tried, it’s harder to make that argument. States like South Dakota have done fairly well with low stringency, while states like New Jersey with high stringency have fared poorly. The charts above provide multiple pair-wise examples and counter-examples of states or countries having faced hard waves with different results.
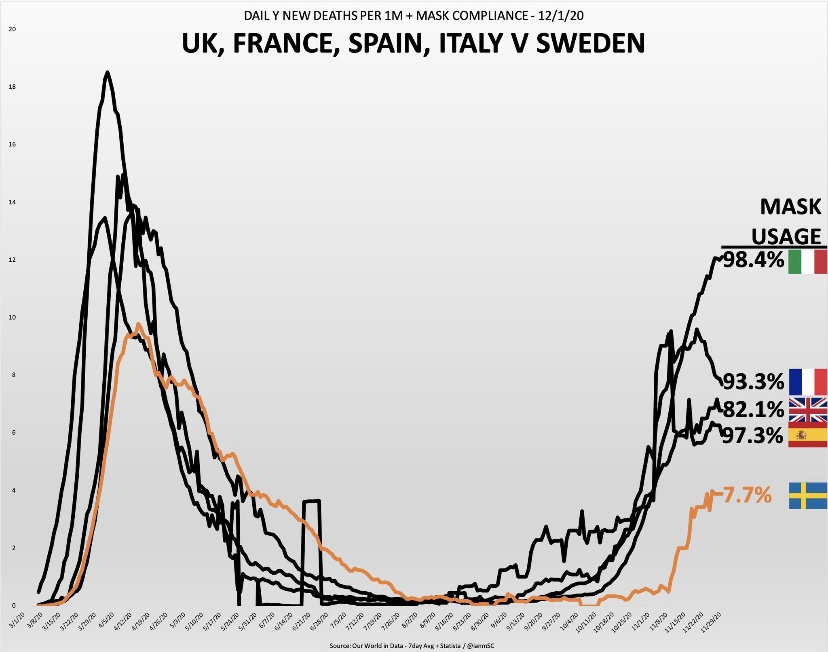
But let’s look at a few specific situations.
The countries shown above have converged somewhat over the past month: Sweden’s daily deaths have risen while the others have declined to greater or lesser degrees, but the implications for mask usage are unaltered.
And of course we have this gem, predicated on the mental gymnastics lockdown enthusiasts are fond of performing:
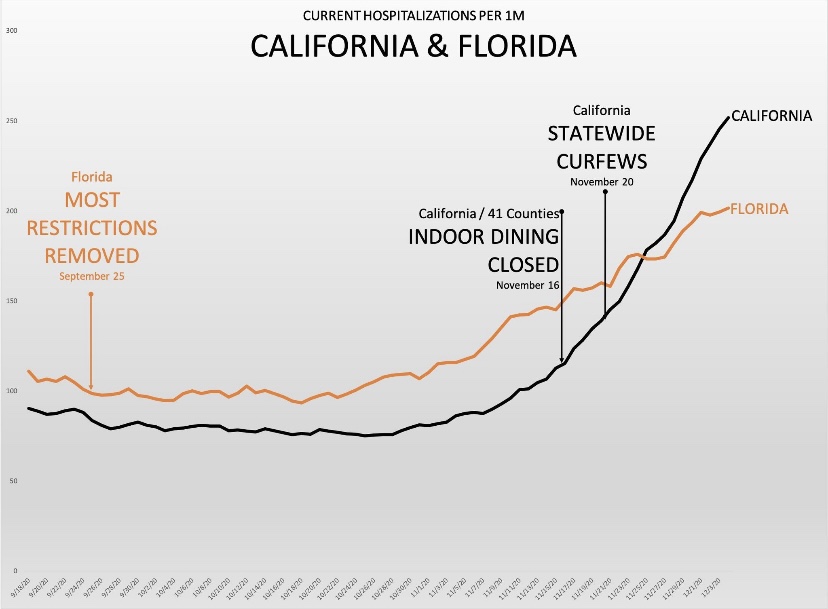
But seriously, it’s been a typical pattern: cases rise to a point at which officials muster the political will to impose restrictions, often well after the “exponential” phase of the wave or even the peak has passed. For the sake of argument, if we were to stipulate that lockdowns save lives, it would take time for these measures to mitigate new infections, time for some of the infected individuals to become symptomatic, and more time for diagnosis. For the lockdown arguments to be persuasive, the implementation of NPIs would have to precede the point at which the growth of cases begins to decline by a few weeks. That’s something we’ve seldom observed, but officials always seem to take credit for the inevitable decline in cases.
More informed lockdown proponents have been hanging their hats on this paper in Nature by Seth Flaxman, et al, published in July. As Philippe LeMoine has shown, however, Flaxman and his coauthors essentially assumed their result. After a fairly exhaustive analysis, Lemoine, a man who understands sophisticated mathematics, offers these damning comments:
“Their paper is a prime example of propaganda masquerading as science that weaponizes complicated mathematics to promote questionable policies. Complicated mathematics always impresses people because theydon’t understand it and it makes the analysis look scientific, but often it’s used to launder totally implausible assumptions, which anyone could recognize as such if they were stated in plain language. I think it’s exactly what happened with Flaxman et al.’s paper, which has been used as a cudgel to defend lockdowns, even though it has no practical relevance whatsoever.”
The Economic Costs of Stringency
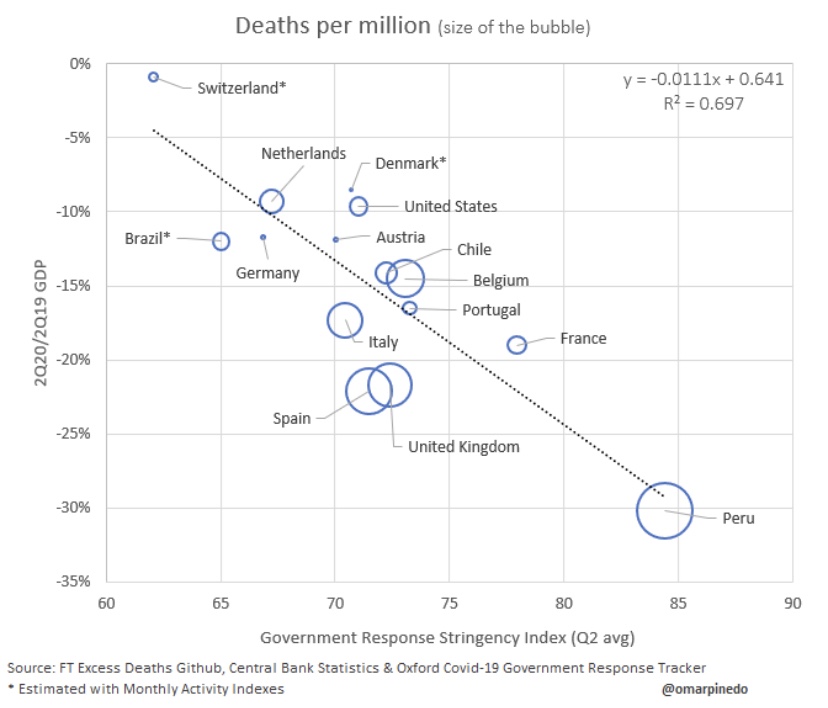
So the benefits of stringent lockdowns in terms of averting sickness and death from COVID are speculative at best. What about the costs of lockdowns? We can start with their negative impact on economic activity:
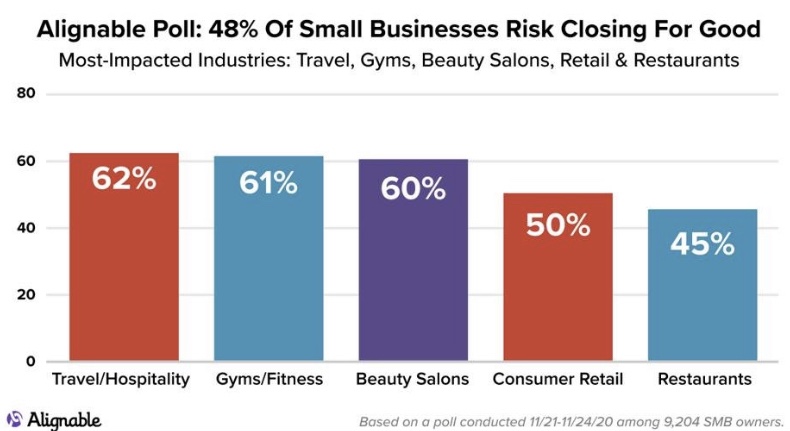
That’s a pretty bad reflection on NPI stringency. In the U.S, a 10% decline in GDP in 2020 amounts to about $2.1 trillion in lost goods and services. That’s just for starters. The many destroyed businesses and livelihoods carry an ongoing cost that could take years to fade, as this graphic on permanent business closures shows:
If you’re wondering about the distributional effects of lockdowns, here’s more bad news:
It’s possible to do many high-paying jobs from home. Not so for blue-collar workers. And distributional effects by size of enterprise are also heavily-skewed in favor of big companies. Within the retail industry, big-box stores are often designated as “essential”, while small shops and restaurants are not. The restaurant industry has been destroyed in many areas, inflicting a huge blow to owners and workers. This despite evidence from contact tracing showing that restaurants and bars account for a very small share of transmission. To add insult to injury, many restaurants invested heavily in safety measures and equipment to facilitate new, safer ways of doing business, only to be double-crossed by officials like Andrew Cuomo and Eric Garcetti, who later shut them down.
Public Health Costs of Stringency
Lives are lost due to lockdowns, but here’s a little exercise for the sake of argument: The life value implied by individual willingness-to-pay for risk reduction comes in at less than $4 million. Even if the supposed 300,000 COVID deaths had all been saved by lockdowns, that would have amounted to a value of $1.2 trillion, about half of the GDP loss indicated above. Of course, it would be outrageously generous to concede that lives saved by NPI’s have approached 300,000, so lockdowns fall far short at the very outset of any cost-benefit comparison, even if we value individual lives at far more than $4 million.
As AJ Kay says, the social and human costs go far beyond economic losses:
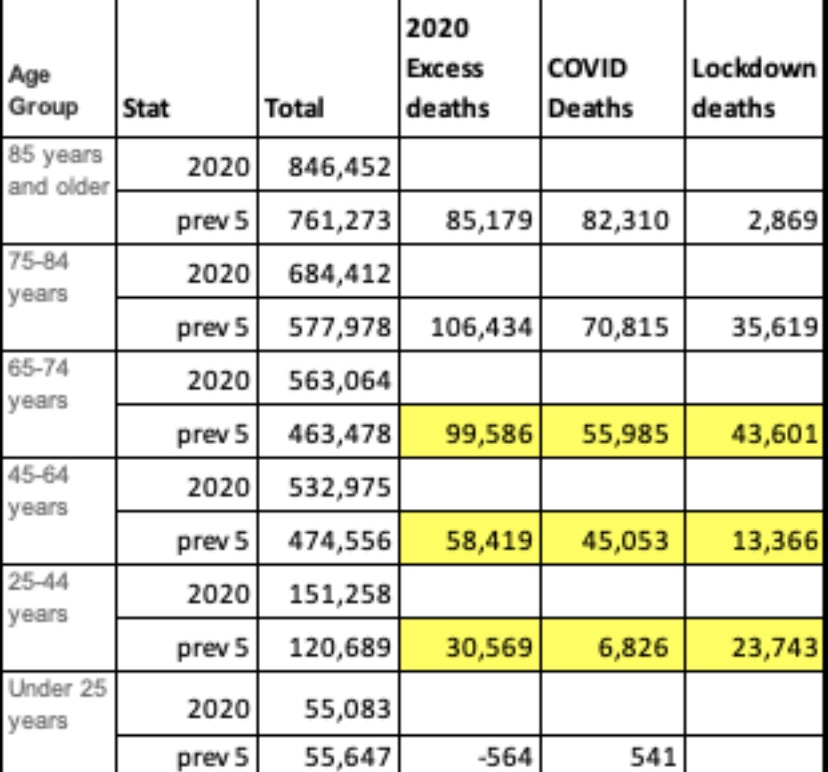
I cited specific examples of losses in many of these categories in an earlier post. But for the moment, instead of focusing on causes of death, take a look at this table provided by Justin Hart showing a measure of non-COVID excess deaths by age group in the far right-hand column:
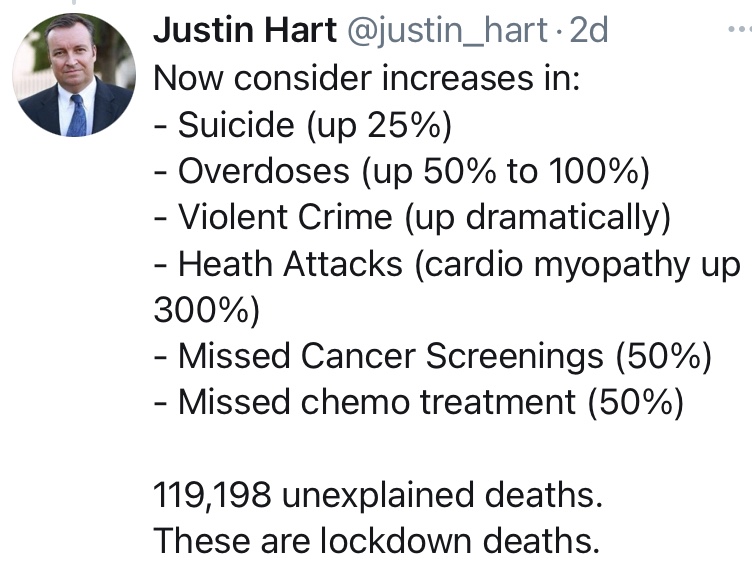
The numbers here are derived by averaging deaths by age group over the previous five years and subtracting COVID deaths in each group. I believe Hart’s numbers go through November. Of greatest interest here is the fact that younger age groups, having far less risk of death from COVID than older age groups, have suffered large numbers of excess deaths NOT attributed to COVID. As Hart notes later in his thread:
These deaths are a tragic consequence of lockdowns.
Educational Costs of Stringency
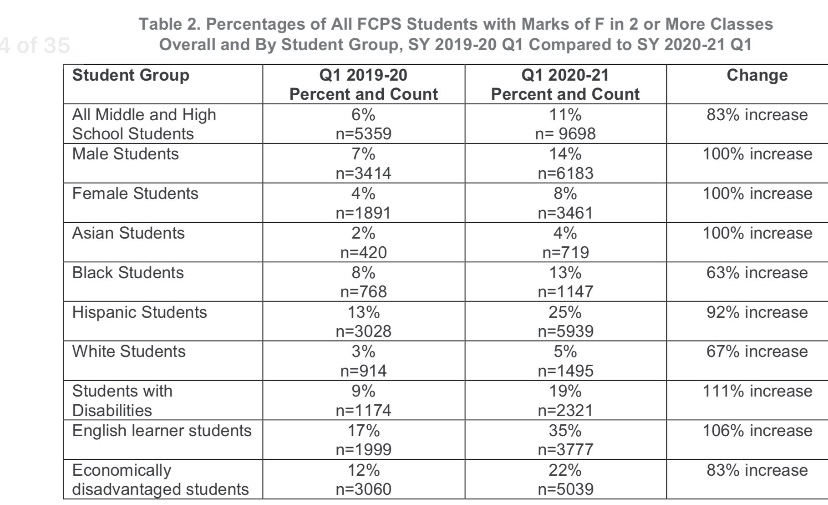
Many schools have been closed to in-person instruction during the pandemic, leading to severe disruptions to the education f children. This report from the Fairfax County, VA School District is indicative, and it is extremely disheartening. The report includes the following table:
Note the deterioration for disabled students, English learners, and the economically disadvantaged. The surfeit of failing grades is especially damaging to groups already struggling in school relative to their peers, such as blacks and Hispanics. Not only has the disruption to in-person instruction been disastrous to many students and their futures; it has also yielded little benefit in mitigating the contagion. A recent study in The Lancet confirms once again that transmission is low in educational settings. Also see here and here for more evidence on that point.
Conclusion
It’s clear that the “follow-the-science” mantra as a rationale for stringent NPIs was always a fraud, as was the knee-jerk response from those who conflated lockdowns with “leadership”. Such was the wrongheaded and ultimately deadly pressure to “do something”. We can be thankful that pressure was resisted at the federal level by President Trump. The extraordinary damage inflicted by ongoing NPIs was quite foreseeable, but there is one more very ominous implication. I’ll allow J.D. Tucille to sum that up with some of the pointed quotes he provides:
“‘The first global pandemic of the digital age has accelerated the international adoption of surveillance and public security technologies, normalising new forms of widespread, overt state surveillance,’ warned Kelsey Munro and Danielle Cave of the Australian Strategic Policy Institute’s Cyber Policy Centre last month.
‘Numerous governments have used the COVID-pandemic to repress expression in violation of their obligations under human rights law,’ United Nations Special Rapporteur on Freedom of Expression David Kaye noted in July.
‘For authoritarian-minded leaders, the coronavirus crisis is offering a convenient pretext to silence critics and consolidate power,’ Human Rights Watch warned back in April.
There’s widespread agreement, then, that government officials around the world are exploiting the pandemic to expand their power and to suppress opposition. That’s the case not only among the usual suspects where authorities don’t pretend to take elections and civil liberties seriously, but also in countries that are traditionally considered ‘free.’ … It’s wildly optimistic to expect that newly acquired surveillance tools and enforcement powers will simply evaporate once COVID-19 is sent on its way. The post-pandemic new normal is almost certain to be more authoritarian than what went before.”
The other day a friend told me “your data points always seem to miss the people points.” He imagines a failure on my part to appreciate the human cost of the coronavirus. Evidently, he feels that I treat data on cases, hospitalizations, and deaths as mere accounting issues, all while emphasizing the negative aspects of government interventions.
This fellow reads my posts very selectively, hampered in part by his own mood affiliation. Indeed, he seems to lack an appreciation for the nuance and zeitgeist of my body of blogging on the topic… my oeuvre! This despite his past comments on the very things he claims I haven’t mentioned. His responses usually rely on anecdotes relayed to him by nurses or doctors he knows. Anecdotes can be important, of course. But I know nurses and doctors too, and they are not of the same mind as his nurses and doctors. Anecdotes! We’re talking about the determination of optimal policy here, and you know what Dr. Fauci says about relying on anecdotes!
Incremental Costs and Benefits
My friend must first understand that my views are based on an economic argument, one emphasizing the benefits and costs of particular actions, including human costs. COVID is dangerous, but primarily to the elderly, and no approach to managing the virus is free. Here are two rather disparate choices:
Mandated minimization of economic and social interactions throughout society over some time interval in the hope of reducing the spread of the virus;
Laissez faire for the general population while minimizing dangers to high-risk individuals, subject to free choice for mentally competent, high-risk individuals.
To be clear, #2 entails all voluntary actions taken by individuals to mitigate risks. Therefore, #1 implies a set of incremental binding restrictions on behavior beyond those voluntary actions. However, I also include in #1 the behavioral effects of scare mongering by public officials, who regularly issue pronouncements having no empirical basis.
The first option above entails so-called non-pharmaceutical interventions (NPIs) by government. These are the elements of so-called lockdowns, such as quarantines and other restrictions on mobility, business and consumer activity, social activities, health care activities, school closures, and mask mandates. NPIs carry costs that are increasing in the severity of constraints they impose on society.
And before I proceed, remember this: tallying all fatal COVID cases is really irrelevant to the policy exercise. Nothing we do, or could have done, would save all those lives. We should compare what lives can be saved from COVID via lockdowns, if any, with the cost of those lockdowns in terms of human life and human misery, including economic costs.
Economic Losses
NPIs involve a loss of economic output that can never be recovered… it is gone forever, and a loss is likely to continue for some time to come. That sounds so very anodyne, despite the tremendous magnitude of the loss involved. But let’s stay with it for just a second. The loss of U.S. output in 2020 due to COVID has been estimated at $2.5 trillion. As Don Boudreaux and Tyler Cowen have noted, what we normally spend on safety and precautionary measures (willingness-to-pay), together with the probabilities of losses, implies that we value our lives at less than $4 million on average. Let’s say the COVID death toll reaches 300,000 by year-end (that’s incremental in this case— but it might be a bit high). That equates to a total loss of $1.2 trillion in life-value if we ignore distinctions in life-years lost. Now ask this: if our $2.5 trillion output loss could have saved every one of those 300,000 lives, would it have been worth it? Not even close, and the truth is that the sacrifice will not have saved even a small fraction of those lives. I grant, however, that the economic losses are partly attributable to voluntary decisions, but goaded to a great extent by the alarmist commentary of public health officials.
The full depth of losses is far worse than the dollars and cents comparison above might sound. Output losses are always matched by (and, in value, are exactly the same as) income losses. That involves lost jobs, lost hours, failed businesses, and destroyed careers. Ah, now we’re getting a bit more “human”, aren’t we! It’s nothing short of callous to discount these costs. Unfortunately, the burden falls disproportionately on low-income workers. Our elites can mostly stay home and do their jobs remotely, and earn handsome incomes. The working poor spend their time in line at food banks.
Yes, government checks can help those with a loss of income compete with elites for the available supply of goods, but of course that doesn’t replace the lost supply of goods! Government aid of this kind is a palliative measure; it doesn’t offset the real losses during a suspension of economic activity.
Decimated Public Health
The strain of the losses has been massive in the U.S. and nearly everywhere in the world. People are struggling financially, making do with less on the table, depleting their savings, and seeking forbearance on debts. The emotional strains are no less real. Anxiety is rampant, drug overdoses have increased, calls to suicide hotlines have exploded, and the permanence of the economic losses may add to suicide rates for some time to come. Dr. Robert Redfield of the CDC says more teenagers will commit suicide this year than will die from COVID (also see here). There’s also been a terrifying escalation in domestic abuse during the pandemic, including domestic homicide. The despair caused by economic losses is all too real and should be viewed as a multiplier on the total cost of severe NPIs.
More on human costs: a health care disaster has befallen locked-down populations, including avoidance of care on account of panic fomented by so-called public health experts, the media, and government. Some of the consequences are listed here. But to name just a few, we have huge numbers of delayed cancer diagnoses, which sharply decrease survival time; mass avoidance of emergency room visits, including undiagnosed heart attacks and strokes; and unacceptable delays in cardiac treatments. Moreover, lockdowns worldwide have severely damaged efforts to deal with scourges like HIV, tuberculosis, and malaria.
The CDC reports that excess mortality among 25-44 year-olds this year was up more than 26%, and the vast bulk of these were non-COVID deaths. A Lancet study indicates that a measles outbreak is likely in 2021 due to skipped vaccinations caused by lockdowns. The WHO estimates that 130,000,000 people are starving worldwide due to lockdowns. That is roughly the population of the U.S. east coast. Again, the callousness with which people willfully ignore these repercussions is stunning, selfish and inhumane, or just stupid.
Excess Deaths
Can we quantify all this? Yes we can, as a matter of fact. I’ve offered estimates in the past, and I already mentioned that excess deaths, COVID and non-COVID, are reported on the CDC’s web site. The Ethical Skeptic (TES) does a good job of summarizing these statistics, though the last full set of estimates was from October 31. Here is the graphic from the TES Twitter feed:
Note particularly the huge number of excess deaths attributable to SAAAD (Suicide, Addiction Abandonment, Abuse and Despair): over 50,000! The estimate of life-years lost due to non-COVID excess deaths is almost double that of COVID deaths because of the difference in the age distributions of those deaths.
Here are a few supporting charts on selected categories of excess deaths, though they are a week behind the counts from above. The first is all non-COVID, natural-cause excess deaths (the vertical gap between the two lines), followed by excess deaths from Alzheimer’s and dementia, other respiratory diseases, and malignant neoplasms (cancer):
The clearest visual gap in these charts is the excess Alzheimer’s and dementia deaths. Note the increase corresponding to the start of the pandemic, when these patients were suddenly shut off from loved ones and the company of other patients. I also believe some of these deaths were (and are) due to overwhelmed staff at care homes struck by COVID, but even discounting this category of excess deaths leaves us with a huge number of non-COVD deaths that could have been avoided without lockdowns. This represents a human cost over and above those tied to the economic losses discussed earlier.
Degraded Education and Health
Lockdowns have also been destructive to the education of children. The United Nations has estimated that 24 million children may drop out of school permanently as a result of lockdowns and school closures. This a burden that falls disproportionately on impoverished children. This article in the Journal of the American Medical Association Network notes the destructive impact of primary school closures on educational attainment. Its conclusions should make advocates of school closures reconsider their position, but it won’t:
“… missed instruction during 2020 could be associated with an estimated 5.53 million years of life lost. This loss in life expectancy was likely to be greater than would have been observed if leaving primary schools open had led to an expansion of the first wave of the pandemic.“
Lockdown Inefficacy
Lockdowns just don’t work. There was never any scientific evidence that they did. For one thing, they are difficult to enforce and compliance is not a given. Of course, Sweden offers a prime example that draconian lockdowns are unnecessary, and deaths remain low there. This Lancet study, published in July, found no association between lockdowns and country mortality, though early border closures were associated with lower COVID caseloads. A French research paper concludes that public decisions had no impact on COVID mortality across 188 countries, U.S. states, and Chinese states. A paper by a group of Irish physicians and scientists stated the following:
“Lockdown has not previously been employed as a strategy in pandemic management, in fact it was ruled out in 2019 WHO and Irish pandemic guidelines, and as expected, it has proven a poor mitigator of morbidity and mortality.”
One of the chief arguments in favor of lockdowns is the fear that asymptomatic individuals circulating in the community (and there are many) would spread the virus. However, there is no evidence that they do. In part, that’s because the window during which an individual with the virus is infectious is narrow, but tests may detect tiny fragments of the virus over a much longer span of time. And there is even some evidence that lockdown measures may increase the spread of the virus!
Lockdown decisions are invariably arbitrary in their impact as well. The crackdown on gyms is one noteworthy example, but gyms are safe. Restaurants don’t turn up in many contact traces either, and yet restaurants have been repeatedly implicated as danger zones. And think of the many small retailers shut down by government, while giant competitors like Wal-Mart continue to operate with little restriction. This is manifest corporatism!
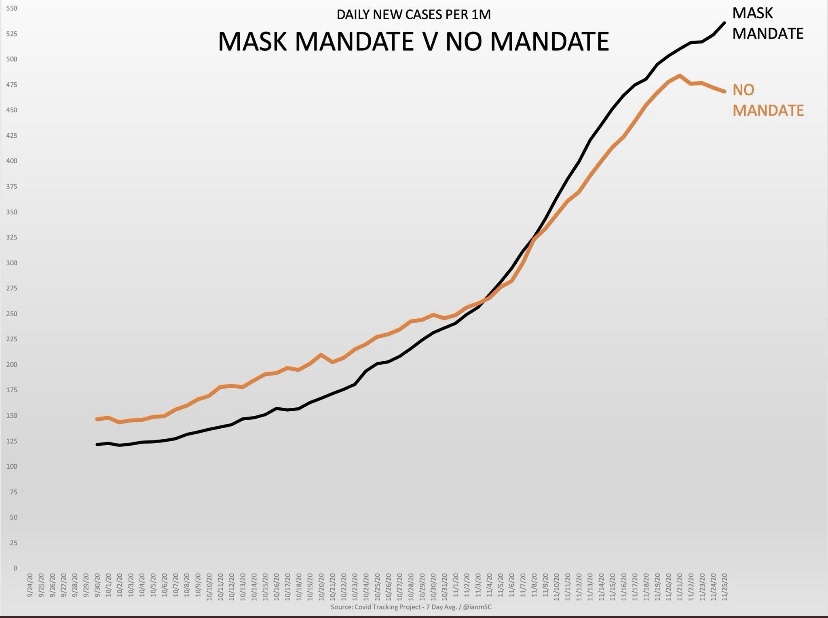
Then there is the matter of mask mandates. As readers of this blog know, I think masks probably help reduce transmission from droplets issued by a carrier, that is, at close range. However, this recent Danish study in the Annals of Internal Medicine found that cloth masks are ineffective in protecting the wearer. They do not stop aerosols, which seem to be the primary source of transmission. They might reduce viral loads, at least if worn properly and either cleaned often or replaced. Those are big “ifs”.
To the extent that masks offer any protection, I’m happy to wear them within indoor public accommodations, at least for the time being. To the extent that people are “scared”, I’m happy to observe the courtesy of wearing a mask, but not outside in uncrowded conditions. To the extent that masks are required under private “house rules”, of course I comply. Public mask mandates outside of government buildings are over the line, however. The evidence that those mandates work is too tenuous and our liberties are too precious too allow that kind of coercion. And private facilities should be subject to private rules only.
QED
So my poor friend is quite correct that COVID is especially deadly to certain cohorts and challenging for the health care community. But he must come to grips with a few realities:
The virus won’t be defeated with NPIs; they don’t work!
NPIs inflict massive harm to human well-being.
Lockdowns or NPIs are little or no gain, high-pain propositions.
The rejection of NPI’s, or lockdowns, is based on compelling “human” data points. As Don Boudreaux says:
“The lockdowns and other restrictions on economic and social activities are astronomically costly – in a direct economic sense, in an emotional and spiritual sense, and in a ‘what-the-hell-do-these-arbitrary-diktats-portend-for-our-freedom?’ sense.”
This doctor has a message for the those denizens of social media with an honest wish to dispense helpful public health advice:
“Americans have admitted that they will meet for Thanksgiving. Scolding and shaming them for wanting this is unlikely to slow the spread of SARS-CoV-2, though it may earn you likes and retweets. Starting with compassion, and thinking of ways they can meet, but as safely as possible, is the task of real public health. Now is the time to save public health from social media.”
Acceptance of risk is a necessary part of a good life, and extreme efforts to avoid it are your own business. Government has no power to guarantee absolute safety, nor should we presume to have such a right. Ongoing COVID lockdowns are an implicit assertion of exactly that kind of government power, despite the impotence of those efforts, and they constitute a rejection of more fundamental rights.
Lockdowns have had destructive effects on health and economic well being while conferring little if any benefit in mitigating harm from the virus. The lockdowns were originally sold as a way to “flatten the curve”, that is, to avoid a spike in cases and an overburdened health care system. However, this arguably well-qualified rationale later expanded in scope to encompass the mitigation of smaller and much less deadly outbreaks among younger cohorts, and then to the very idea of extinguishing the virus altogether. It’s become painfully obvious that such measures are not capable of achieving those goals.
In the U.S., the ongoing lockdowns have been a cause célèbre largely on the interventionist Left, and they have been prolonged mainly by Democrats at various levels of government. In a way, this is not unlike many other policies championed by the Left, often ostensibly designed to help members of the underclasses: instead, those policies often destroy or wrongly obviate incentives and promote dependency on the state. In this case, the plunge into dependency is a reality the Left would very much like to ignore, or to blame on someone else. You know who.
The lockdowns have been largely unsuccessful in mitigating the spread of the virus. At the same time, they have been used as a pretext to deny constitutional rights such as the free practice of religion, assembly, and a broad range of unenumerated rights under the “penumbra” of the Bill of Rights and the Ninth Amendment. What’s more, the severity of the economic blow caused by lockdowns has been borne disproportionately by the working poor and the small businesses who employ so many of them.
Lockdowns are deadly. It’s not clear that they’ve saved any lives, but they have massively disrupted the operation of the health care system with major consequences for those with chronic and undiagnosed conditions. The lockdowns have also led to spikes in mental health issues, alcoholism, drug abuse, and deaths of despair. A recent study found that over 26% of the excess deaths during the pandemic were non-COVID deaths. Those deaths were avoidable or accelerated, whereas the lockdowns have failed to meaningfully curtail COVID deaths. Don’t tell me about reduced traffic fatalities: that reduction is relatively small relative to the increase in non-COVID excess deaths (see below).
What proof do we have that lockdowns cause excess deaths? See this study in The Lancet on cancer deaths due to lockdown-induced delays in diagnoses. See this study on UK school closures. See this Oxfam Internationalreport on lockdown-induced starvation. Other reports from the UK suggests that lockdown deaths are widespread, having taken nearly 2,800 per week early in the pandemic, and many other deaths yet to occur have been made inevitable by lockdowns. Doctors in the U.S. have warned that lockdowns are a “mass casualty incident”, and a German government study warned of the same.
The Ethical Skeptic (TES) on Twitter has been tracking a measure of lockdown deaths for some time now. The following graphic provides a breakdown of excess non-COVID deaths since the start of the pandemic. The total “pie” shows almost 320,000 excess deaths through September 26th (avoiding less complete counts in recent weeks), as reported by the CDC. COVID accounted for 202,000 of those deaths, based on state-level reporting. Of the remaining 117,000 excess deaths, TES uses CDC data to allocate roughly 85,000 to various causes, the largest (more than half) being “Suicide, Addiction, Abandonment, and Abuse”. Other large categories include Cardio/Diabetes, Stroke, premature Alzheimers/Dementia death, and Cancer Access. Nearly 32,000 excess deaths remain as a “backlog”, not yet reported with a cause by states.
Also of interest in the graphic are estimates of life-years lost. The vast bulk of COVID victims are elderly, of course, which means that any estimate of lost years per victim must be relatively low. On the other hand, most non-COVID, lockdown-related deaths are among younger victims, with correspondingly greater life-years lost. TES’s aggregate estimate is that lockdown-related excess deaths involve double the life-years lost of COVID deaths. Of course, that is an estimate, but even granting some latitude for error, the reality is horrifying!
John Tierney in City Journal cites several recent studies concluding that lockdowns have been largely ineffective in Europe and in the U.S. While Tierney doesn’t rule out the possibility that lockdowns have produced some benefits, they have carried excessive costs and risks to public health going forward, such as lingering issues for those having deferred important health care decisions as well as disruption in future economic prospects. Ultimately, lockdowns don’t accomplish anything:
“While the economic and social costs have been enormous, it’s not clear that the lockdowns have brought significant health benefits beyond what was achieved by people’s voluntary social distancing and other actions.”
Tierney also discusses the costs and benefits of lockdowns in terms of life years: quality-adjusted life-years (QALY), which is a widely-used measure for evaluating of the use of health care resources:
“By the QALY measure, the lockdowns must be the most costly—and cost-ineffective—medical intervention in history because most of the beneficiaries are so near the end of life. Covid-19 disproportionately affects people over 65, who have accounted for nearly 80 percent of the deaths in the United States. The vast majority suffered from other ailments, and more than 40 percent of the victims were living in nursing homes, where the median life expectancy after admission is just five months. In Britain, a study led by the Imperial College economist David Miles concluded that even if you gave the lockdown full credit for averting the most unrealistic worst-case scenario (the projection of 500,000 British deaths, more than ten times the current toll), it would still flunk even the most lenient QALY cost-benefit test.”
We can now count the World Health Organizationamong the detractors of lockdowns. According to WHO’s Dr. David Nabarro:
“Lockdowns just have one consequence that you must never ever belittle, and that is making poor people an awful lot poorer…. Look what’s happened to smallholder farmers all over the world. … Look what’s happening to poverty levels. It seems that we may well have a doubling of world poverty by next year. We may well have at least a doubling of child malnutrition.”
In another condemnation of the public health consequences of lockdowns, number of distinguished epidemiologists have signed off on a statement known as The Great Barrington Declaration. The declaration advocates a focused approach of protecting the most vulnerable from the virus, while allowing those at low risk to proceed with their lives in whatever way they deem acceptable. Those at low risk of severe disease can acquire immunity, which ultimately inures to the benefit of the most vulnerable. With few, brief, and local exceptions, this is how we have always dealt with pandemics in the past. That’s real life!
In advanced civilizations the period loosely called Alexandrian is usually associated with flexible morals, perfunctory religion, populist standards and cosmopolitan tastes, feminism, exotic cults, and the rapid turnover of high and low fads---in short, a falling away (which is all that decadence means) from the strictness of traditional rules, embodied in character and inforced from within. -- Jacques Barzun