It’s been said that many of the so-called “heroes” of the COVID pandemic who’ve been celebrated by the media are actually villains, and perhaps Governor Andrew Cuomo of New York should top the list. He saw to it that retirement homes were seeded with infected patients by ordering them returned their care homes rather than admitted to hospitals. Deaths in these facilities mounted, and they mounted faster than Cuomo’s administration was willing to admit. But the media and even Democrat state legislators have begun to take note, which is practically a miracle!
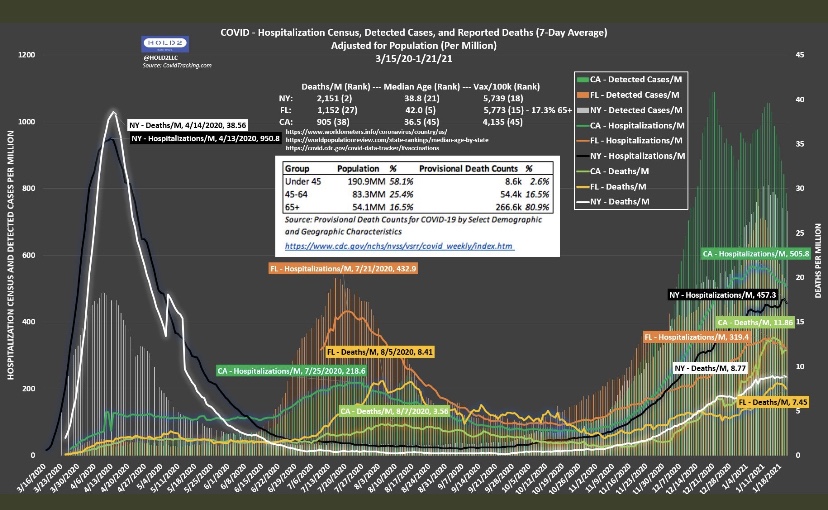
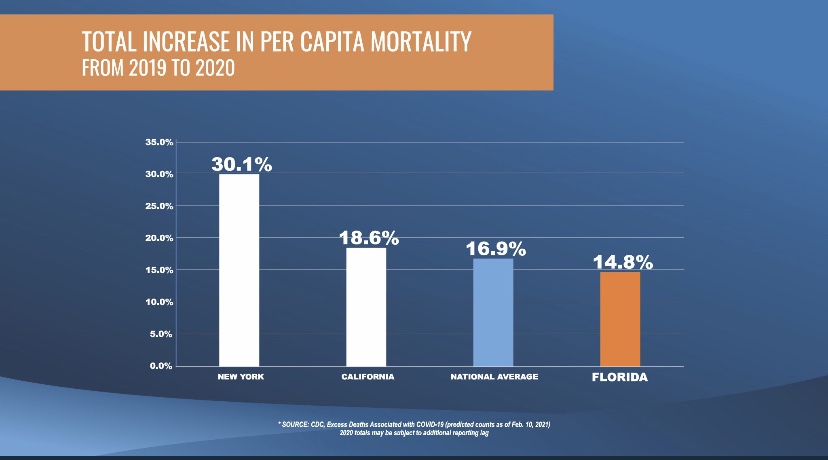
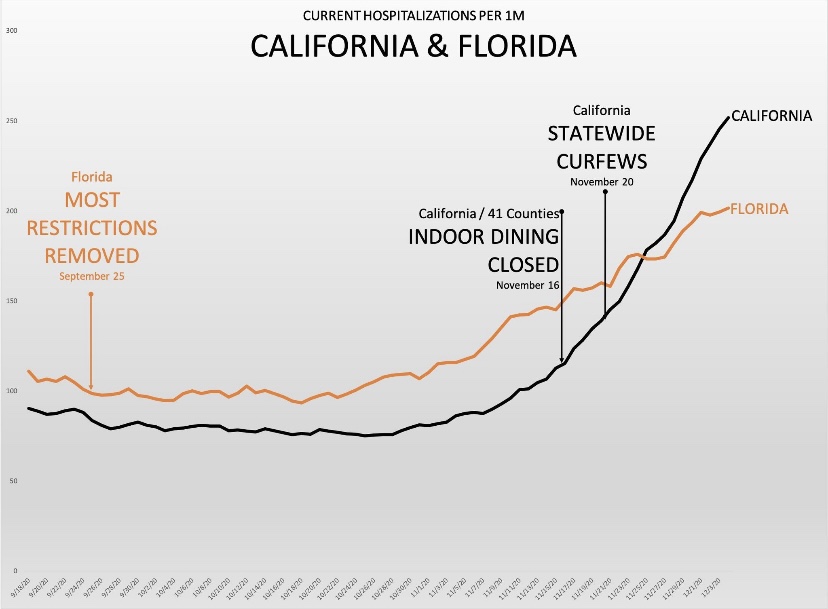
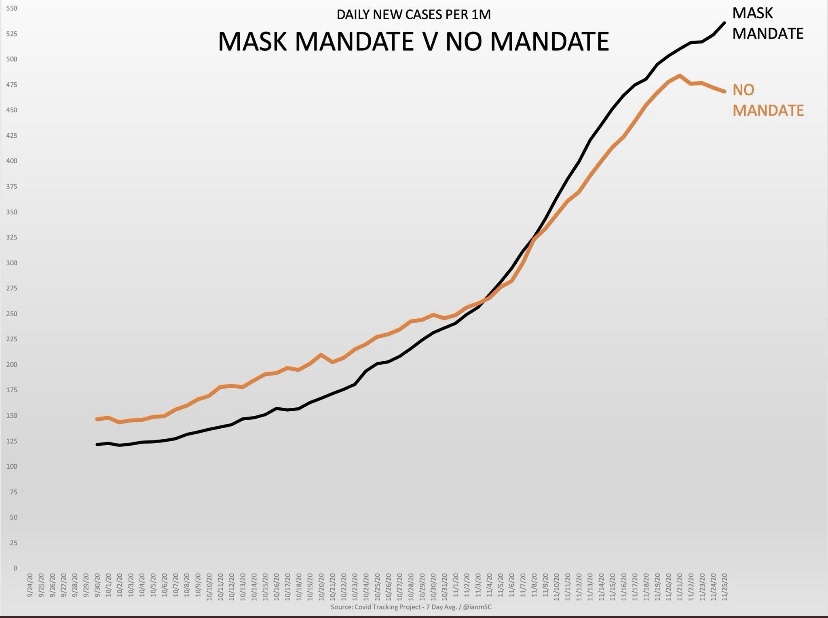
It seems equally true that some vilified by the media for their COVID response are actually heroes. Governor Ron DeSantis of Florida might deserve top honors here. Having spent the last month in Florida, I can attest that the business and social environment here is quite open compared to my home state (despite the presence of a few freaked out northerners who can’t quite fathom how stupid they look wearing masks on the beach). Florida’s infections, hospitalizations, and deaths have been lower than in California, New York, and many other states where lockdown measures have been stringent. (The first chart below is just a little busy…)
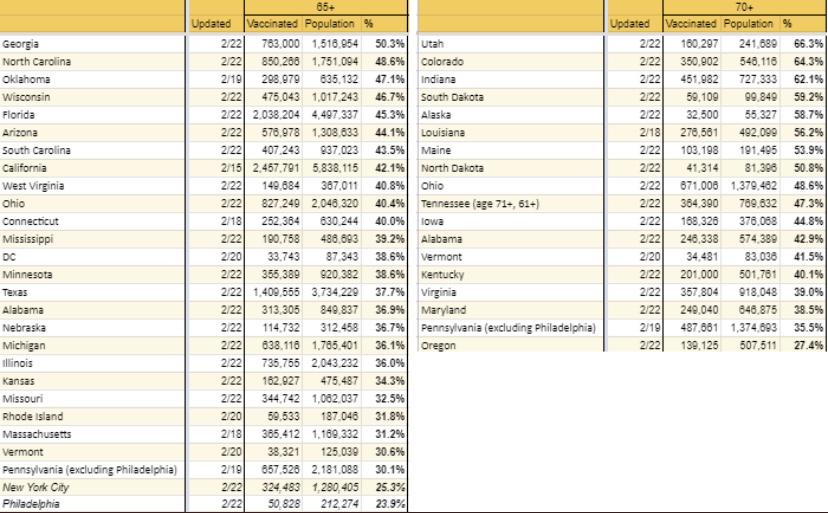
As I’ve written for much of the past year, COVID is far more dangerous to the elderly than anyone else, particularly those with co-morbidities. It’s also true that blacks (and some other minorities) are more vulnerable than whites, but if we want to save more black lives, we’re still better off prioritizing the elderly than racial groups. DeSantis understands this, and Florida is among the leaders in vaccinating the elderly population. (States don’t report this data on a uniform basis):
This approach to saving lives is obvious, yet critics at outlets like NBC News insist that DeSantis must be pandering to the senior population in Florida. Well, one wouldn’t want to be responsive to voters who happen to face high mortality risks, right? Others such as horror writer Stephen Kinghave jumped onboard to offer their bumbling public health expertise as well.
There were many experts and the usual collection of numbskulls on social media who were wrong about Florida. DeSantis handled the pandemic as it should have been handled elsewhere. But the propaganda to the contrary goes unabated. For example, this article is pathetic. Can these people be serious? Or are they really that stupid? This goes for the Biden Administration as well, which had entertained the notion of imposing federal travel restrictions on Florida!
The political attacks on Florida and its governor reveal the extent to which opponents wish to ignore the evidence in plain sight. The data on COVID outcomes put the lie to the narrative of a public health emergency requiring massive restrictions on personal liberty. We know those policies are powerless to control the course of the contagion. The pandemic, however, was the key to convincing the public to accept a more authoritarian role for government. It’s a blessing that not everyone bought in, and that there are places like Florida where you can still go about your business in approximate normalcy.
What does it take to shake people out of their statist stupor? Evidently, the sweet “logic” of universal confinement is very appealing to the prescriptive mindset of busybodies everywhere, who anxiously wag their fingers at those whom they view as insufficiently frightened. As difficult as it is for these shrieking, authoritarian curs to fathom, measures like lockdowns, restrictions on business activity, school closures, and mandates on behavior have at besta limited impact on the spread of the coronavirus, and they are enormously costly in terms of economic well-being and many dimensions of public health. Yet the storm of propaganda to the contrary continues. Media outlets routinely run scare stories, dwelling on rising case numbers but ignoring them when they fall; they emphasize inflated measures of pandemic severity; certain researchers and so-called health experts can’t learn the lessons that are plain in the data; and too many public officials feel compelled to assert presumed but unconstitutional powers. At least the World Health Organization has managed to see things clearly, but many don’t want to listen.
I’ll be the first to say I thought the federalist approach to COVID policy was commendable: allow states and local governments to craft policies appropriate to local conditions and political preferences, rather than have the federal government dictate a one-size-fits-all policy. I haven’t wavered in that assessment, but let’s just say I expected more variety. What I failed to appreciate was the extent to which state and local leaders are captive to provincial busybodies, mavens of precautionary excess, and fraudulent claims to scientific wisdom.
Of course, it should be obvious that the “knowledge problem” articulated by Friedrich Hayek is just as dangerous at low-levels of government as it is in a central Leviathan. And it’s not just a knowledge problem, but a political problem: officials become panicked because they fear bad outcomes will spell doom for their careers. Politicians are particularly prone to the hazards of “do-somethingism”, especially if they have willing, status-seeking “experts” to back them up. But as Scott Sumner says:
“When issues strongly impact society, the science no longer ‘speaks for itself’.
Well, the science is not quite as clear as the “follow-the-science” crowd would have you believe. And unfortunately, public officials have little interest in sober assessments of the unintended effects of lockdown policy.
In my last post, I presented a simple framework for thinking about the benefits and costs of lockdown measures, or non-pharmaceutical interventions (NPIs). I also emphasized the knowledge problem: even if there is some point at which NPI stringencies are “optimized”, government does not possess the knowledge to find that point. It lacks detailed information on both the costs and benefits of NPIs, but individual actors know their own tolerance for risk, and they surely have some sense of the risks they pose to others in their normal course of affairs. While voluntary precautions might be imperfect, they accomplish much of what interventionists hope will be gained via coercion. But, in an effort to “sell” NPIs to constituents and assert their authority, officials vastly over-estimate benefits of NPIs and under-estimate the costs.
NPI Stringency and COVID Outcomes
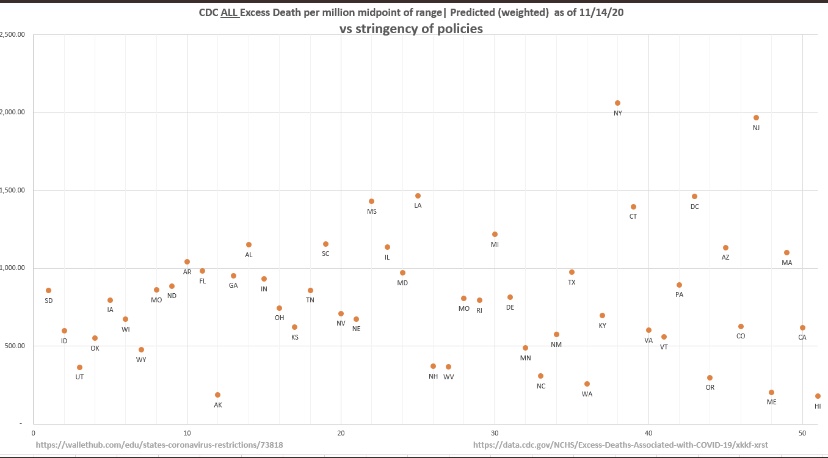
Let’s take a look at a measure of the strength of NPIs by state — the University of Oxford Stringency Index — and compare those to CDC all-cause excess deaths in each state. If it’s hard to read, try clicking on the image or turn your phone sideways. This plot covers outcomes through mid-November:
The chart doesn’t suggest any benefit to the imposition of greater restrictions, or more stringent NPIs. In fact, the truth is that people will do most of the work on their own based on perceptions of risk. That’s partly because government restrictions add little risk mitigation to what can be accomplished by voluntary social distancing and other precautions.
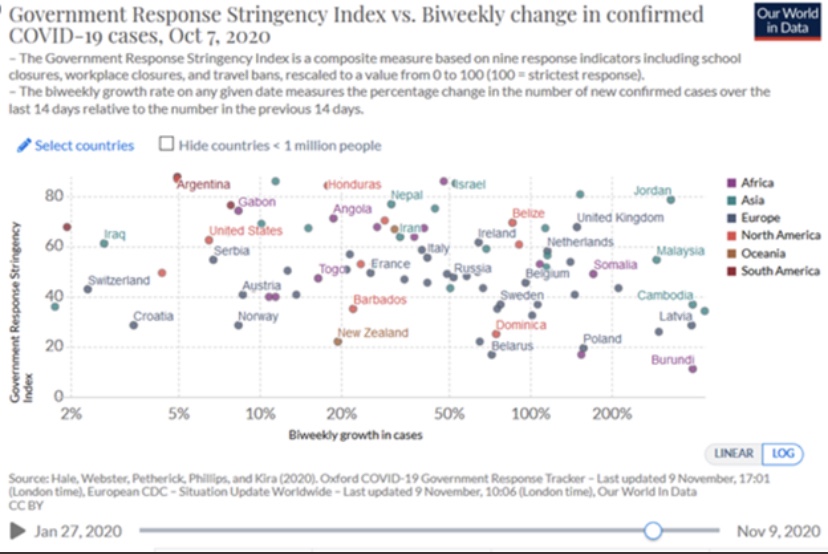
Here’s a similar chart with cross-country comparisons, though the data here ended in early October (I apologize for the fuzzy image):
But what about reverse causality? Maybe the imposition of stringency was a response to more severe contagions. Now that the virus has swept most of the U.S and Europe in three distinct waves, and given the variety and timing of NPIs that have been tried, it’s harder to make that argument. States like South Dakota have done fairly well with low stringency, while states like New Jersey with high stringency have fared poorly. The charts above provide multiple pair-wise examples and counter-examples of states or countries having faced hard waves with different results.
But let’s look at a few specific situations.
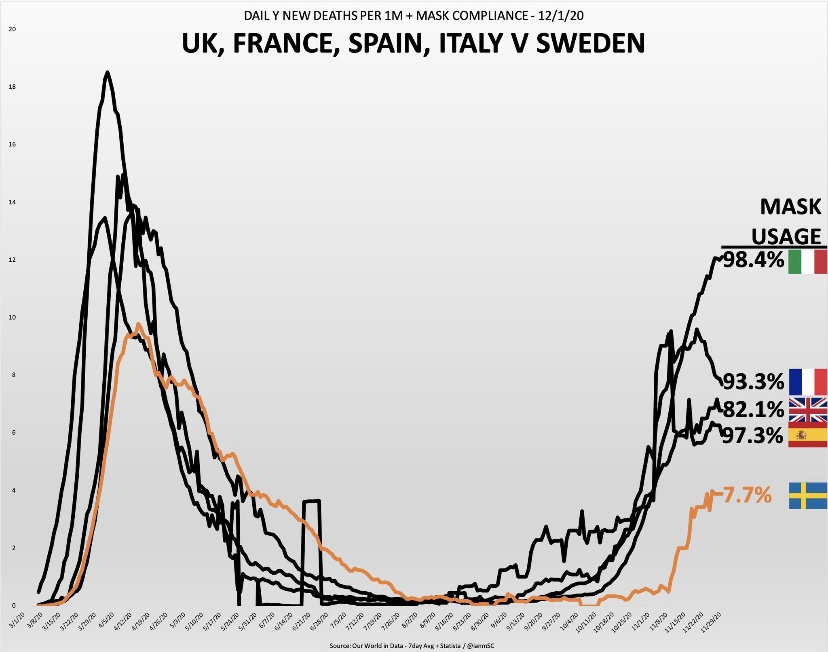
The countries shown above have converged somewhat over the past month: Sweden’s daily deaths have risen while the others have declined to greater or lesser degrees, but the implications for mask usage are unaltered.
And of course we have this gem, predicated on the mental gymnastics lockdown enthusiasts are fond of performing:
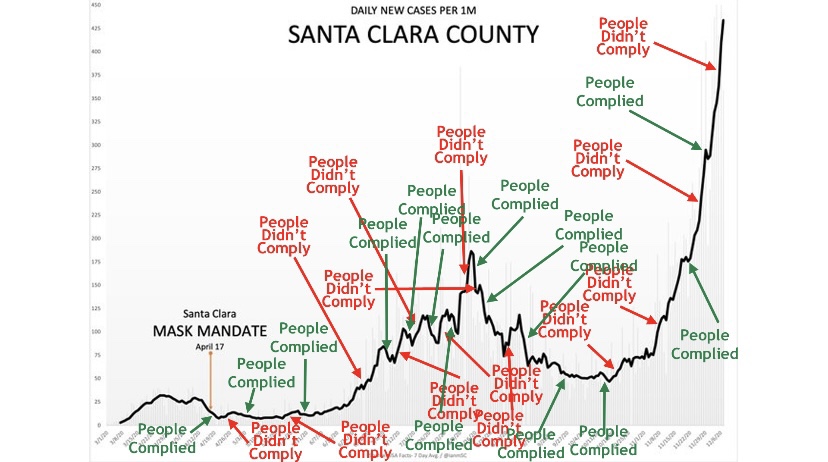
But seriously, it’s been a typical pattern: cases rise to a point at which officials muster the political will to impose restrictions, often well after the “exponential” phase of the wave or even the peak has passed. For the sake of argument, if we were to stipulate that lockdowns save lives, it would take time for these measures to mitigate new infections, time for some of the infected individuals to become symptomatic, and more time for diagnosis. For the lockdown arguments to be persuasive, the implementation of NPIs would have to precede the point at which the growth of cases begins to decline by a few weeks. That’s something we’ve seldom observed, but officials always seem to take credit for the inevitable decline in cases.
More informed lockdown proponents have been hanging their hats on this paper in Nature by Seth Flaxman, et al, published in July. As Philippe LeMoine has shown, however, Flaxman and his coauthors essentially assumed their result. After a fairly exhaustive analysis, Lemoine, a man who understands sophisticated mathematics, offers these damning comments:
“Their paper is a prime example of propaganda masquerading as science that weaponizes complicated mathematics to promote questionable policies. Complicated mathematics always impresses people because theydon’t understand it and it makes the analysis look scientific, but often it’s used to launder totally implausible assumptions, which anyone could recognize as such if they were stated in plain language. I think it’s exactly what happened with Flaxman et al.’s paper, which has been used as a cudgel to defend lockdowns, even though it has no practical relevance whatsoever.”
The Economic Costs of Stringency
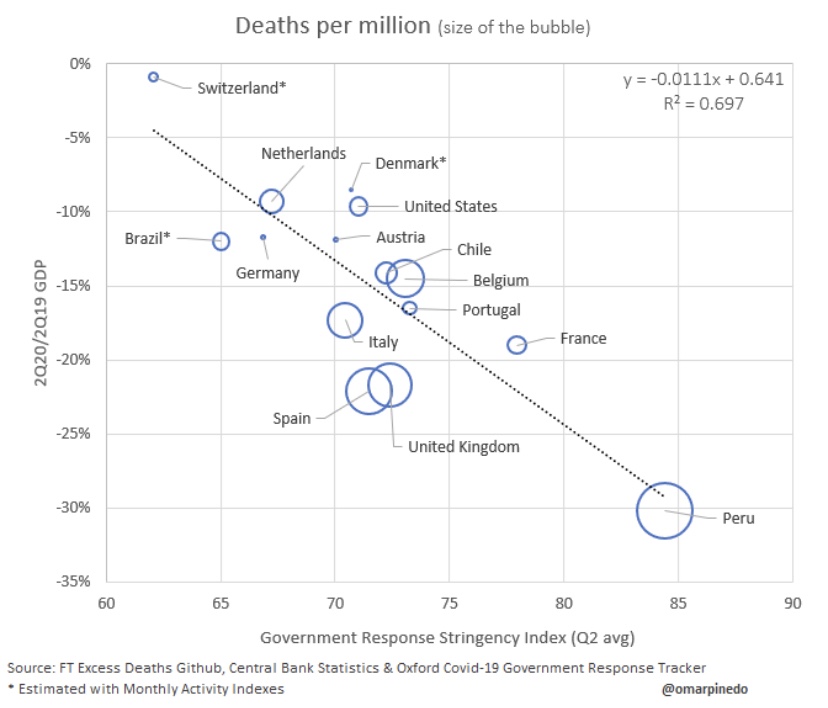
So the benefits of stringent lockdowns in terms of averting sickness and death from COVID are speculative at best. What about the costs of lockdowns? We can start with their negative impact on economic activity:
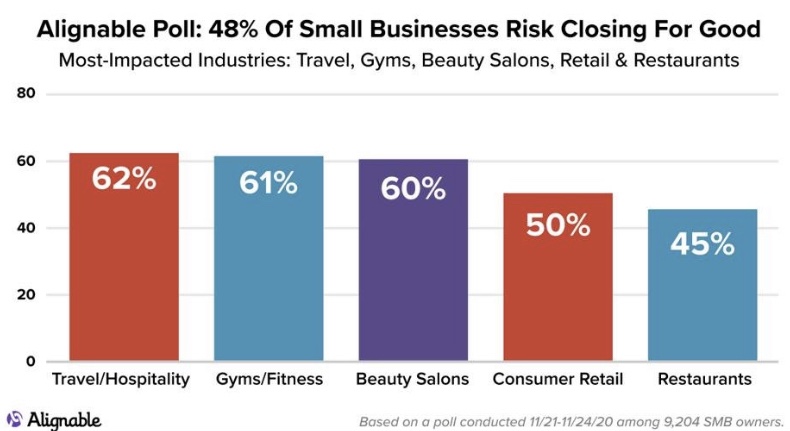
That’s a pretty bad reflection on NPI stringency. In the U.S, a 10% decline in GDP in 2020 amounts to about $2.1 trillion in lost goods and services. That’s just for starters. The many destroyed businesses and livelihoods carry an ongoing cost that could take years to fade, as this graphic on permanent business closures shows:
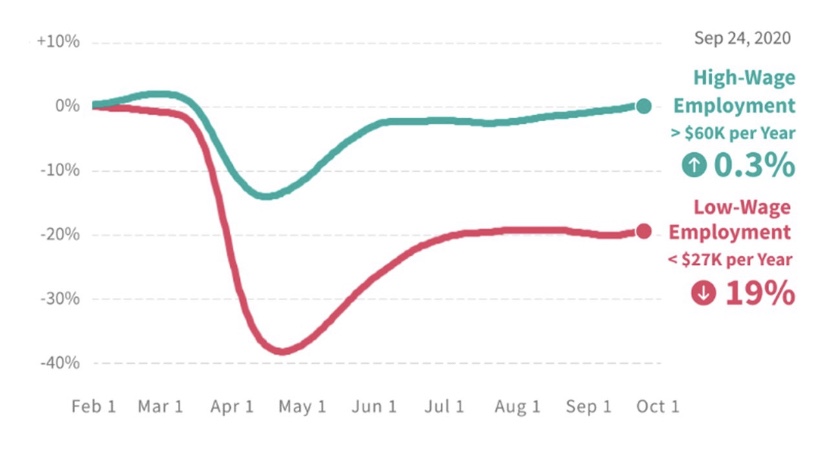
If you’re wondering about the distributional effects of lockdowns, here’s more bad news:
It’s possible to do many high-paying jobs from home. Not so for blue-collar workers. And distributional effects by size of enterprise are also heavily-skewed in favor of big companies. Within the retail industry, big-box stores are often designated as “essential”, while small shops and restaurants are not. The restaurant industry has been destroyed in many areas, inflicting a huge blow to owners and workers. This despite evidence from contact tracing showing that restaurants and bars account for a very small share of transmission. To add insult to injury, many restaurants invested heavily in safety measures and equipment to facilitate new, safer ways of doing business, only to be double-crossed by officials like Andrew Cuomo and Eric Garcetti, who later shut them down.
Public Health Costs of Stringency
Lives are lost due to lockdowns, but here’s a little exercise for the sake of argument: The life value implied by individual willingness-to-pay for risk reduction comes in at less than $4 million. Even if the supposed 300,000 COVID deaths had all been saved by lockdowns, that would have amounted to a value of $1.2 trillion, about half of the GDP loss indicated above. Of course, it would be outrageously generous to concede that lives saved by NPI’s have approached 300,000, so lockdowns fall far short at the very outset of any cost-benefit comparison, even if we value individual lives at far more than $4 million.
As AJ Kay says, the social and human costs go far beyond economic losses:
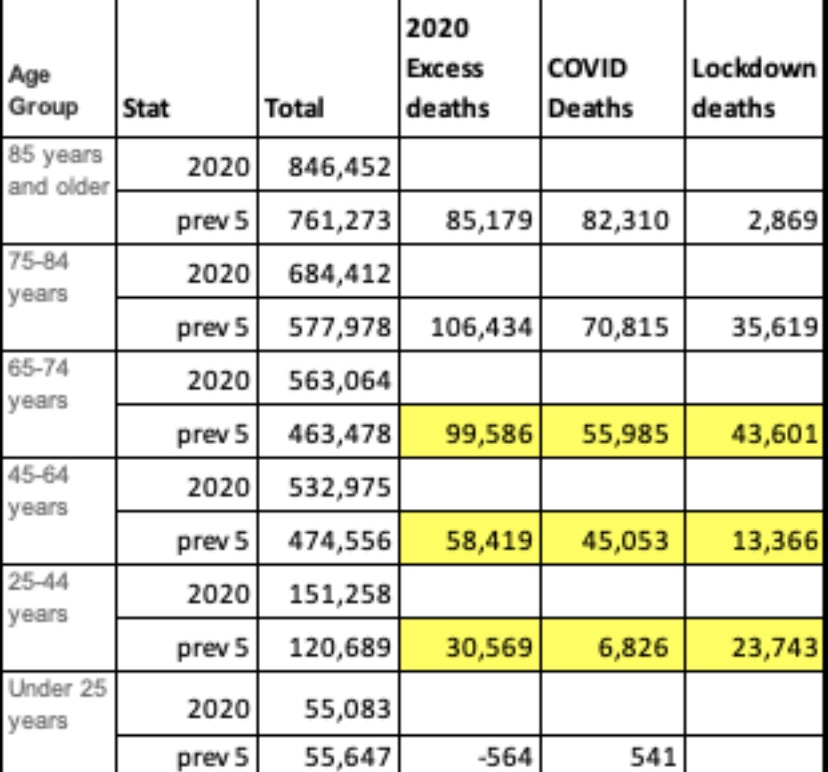
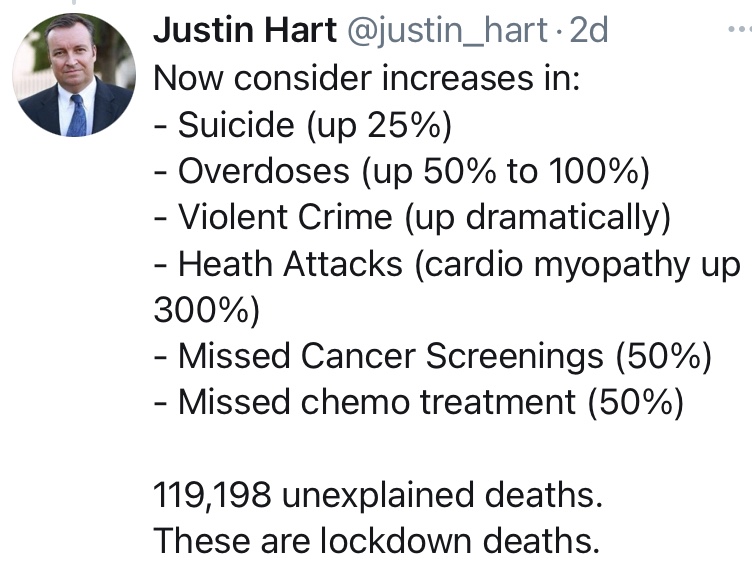
I cited specific examples of losses in many of these categories in an earlier post. But for the moment, instead of focusing on causes of death, take a look at this table provided by Justin Hart showing a measure of non-COVID excess deaths by age group in the far right-hand column:
The numbers here are derived by averaging deaths by age group over the previous five years and subtracting COVID deaths in each group. I believe Hart’s numbers go through November. Of greatest interest here is the fact that younger age groups, having far less risk of death from COVID than older age groups, have suffered large numbers of excess deaths NOT attributed to COVID. As Hart notes later in his thread:
These deaths are a tragic consequence of lockdowns.
Educational Costs of Stringency
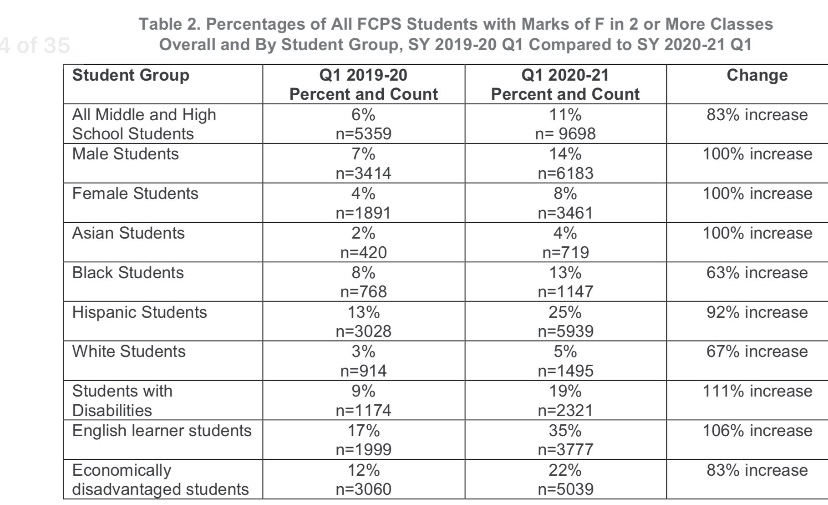
Many schools have been closed to in-person instruction during the pandemic, leading to severe disruptions to the education f children. This report from the Fairfax County, VA School District is indicative, and it is extremely disheartening. The report includes the following table:
Note the deterioration for disabled students, English learners, and the economically disadvantaged. The surfeit of failing grades is especially damaging to groups already struggling in school relative to their peers, such as blacks and Hispanics. Not only has the disruption to in-person instruction been disastrous to many students and their futures; it has also yielded little benefit in mitigating the contagion. A recent study in The Lancet confirms once again that transmission is low in educational settings. Also see here and here for more evidence on that point.
Conclusion
It’s clear that the “follow-the-science” mantra as a rationale for stringent NPIs was always a fraud, as was the knee-jerk response from those who conflated lockdowns with “leadership”. Such was the wrongheaded and ultimately deadly pressure to “do something”. We can be thankful that pressure was resisted at the federal level by President Trump. The extraordinary damage inflicted by ongoing NPIs was quite foreseeable, but there is one more very ominous implication. I’ll allow J.D. Tucille to sum that up with some of the pointed quotes he provides:
“‘The first global pandemic of the digital age has accelerated the international adoption of surveillance and public security technologies, normalising new forms of widespread, overt state surveillance,’ warned Kelsey Munro and Danielle Cave of the Australian Strategic Policy Institute’s Cyber Policy Centre last month.
‘Numerous governments have used the COVID-pandemic to repress expression in violation of their obligations under human rights law,’ United Nations Special Rapporteur on Freedom of Expression David Kaye noted in July.
‘For authoritarian-minded leaders, the coronavirus crisis is offering a convenient pretext to silence critics and consolidate power,’ Human Rights Watch warned back in April.
There’s widespread agreement, then, that government officials around the world are exploiting the pandemic to expand their power and to suppress opposition. That’s the case not only among the usual suspects where authorities don’t pretend to take elections and civil liberties seriously, but also in countries that are traditionally considered ‘free.’ … It’s wildly optimistic to expect that newly acquired surveillance tools and enforcement powers will simply evaporate once COVID-19 is sent on its way. The post-pandemic new normal is almost certain to be more authoritarian than what went before.”
The CDC changed its guidelines on completion of death certificates on April 5th of this year, and only for COVID-19 (C19), just as infections and presumed C19 deaths were ramping up. The substance of the change was to broaden the definition under which death should be attributed to C19. This ran counter to CDC guidelines followed over the previous 17 years, and the change not only makes the C19 death counts suspect: it also makes comparisons of C19 deaths to other causes of death unreliable, since only C19 is subject to the new CDC guidance. That’s true for concurrent and historical comparisons. The distortions are especially bad relative to other respiratory diseases, but also relative to other conditions that are common in mortality data.
The change in the CDC guidelines was noted in a recent report prepared for the Florida House of Representatives. It was brought to my attention by a retweet by Justin Hart linked tothis pieceon Andrew Bostom’s site. Death certificates are divided into two parts: Part 1 provides four lines in which causes of death are listed in reverse clinical order of events leading to death. Thus, the first line is the final clinical condition precipitating death. Prior clinical events are to be listed below that. The example shown above indicates that an auto accident, listed on the fourth line, initiated the sequence of events. Part 2 of the certificate is available for physicians or examiners to list contributing factors that might have played a role in the death that were not part of the sequence of clinical events leading to death.
The CDC’s change in guidelines for C19, and C19 only, made the criteria for inclusion in Part 1 less specific, and it essentially eliminated the distinction between Parts 1 and 2. The following appears under “Vital Records Criteria”:
“A death certificate that lists COVID-19 disease or SARS-CoV-2 as a cause of death or a significant condition contributing to death.”
How much difference does this make? For one thing, it opens the door to C19-attributed deaths in cases of false-positive PCR tests. When large cohorts are subject to testing — for example, all patients admitted to hospitals — there will always be a significant number of false positives even when test specificity is as high as 98 – 99%.
The elimination of any distinction between Parts 1 and 2 causes other distortions. A review of the Florida report is illustrative. The House staff reviewed almost 14,000 certificates for C19-19 attributed deaths. Over 9% of those did not list C19 among the clinical conditions leading to death. Instead, in those cases, C19 was listed as a contributing factor. Under the CDC’s previous guidelines, those would not have been counted as C19 deaths. The Florida House report is conservative in concluding that the new CDC guidelines inflated C19 deaths by only those 9% of the records examined.
There are reasons to think that the exaggeration was much greater, however. First, the Florida House report noted that nearly 60% of the certificates contained information “recorded in a manner inconsistent with state and national guidance”. In addition, almost another 10% of the fatalities were among patients already in hospice! Do we really believe the deaths of all those patients whose diseases had reached such an advanced stage should be classified as C19 fatalities? And another 1-2% listed non-C19 conditions as the immediate and underlying causes.
Finally, more than 20% of the certificates listed C19 alone as a cause of death despite a range of other contributing conditions or co-morbidities. This in itself may have been prompted by the change in the CDC’s guidelines, as the normal standards often involve a “comorbidity” as the initial reason for hospitalization — in that case a clinical event ordinarily listed in Part 1. The high rate of errors and the fact that roughly two-thirds of the deaths reviewed occurred in the hospital, where patients are all tested and often multiple times, raises the specter that up to 20% more of the C19 deaths were either erroneous and/or misclassified due to false positives.
(An exception may have occurred in New York, where an order issued in March by Governor Andrew Cuomo to return C19-positive residents of nursing homes (including suspected C19 cases) back to those homes, The order was made before the change in CDC guidelines and wasn’t rescinded until later in April. There is reason to believe that some of the C19 deaths among nursing home residents in New York were undercounted.)
All told, in the Florida data we have potential misclassification of deaths of 9% + 9% + 2% + 20% = 40%, or inflation relative to actual C19 deaths of up to 40%/60% = 67%! I strongly doubt it’s that high, but I would not consider a range of 25% – 50% exaggeration to be unreasonable.
We know that reports of C19 deaths lag actual dates of death by anywhere from 1 to 8 weeks, sometimes even more. This is misleading when no effort is made to explain that difference, which I’ve never heard out of a single journalist. We also know that false positive tests inflate C19 deaths. The Florida report gives us a sense of how large that exaggeration might be. In addition, the Florida data show that the CDC guidelines inflate C19 deaths in other ways: as a mere contributing factor, it can now be listed as the cause of death, unlike the treatment of pneumonia as a contributing factor, for instance. The same kind of distortion occurs when patients contract C19 (or have a false positive test) while in hospice.
There is no doubt that C19 led to “excess deaths” relative to all-cause mortality. However, many of these fatalities are misclassified, and it’s likely that a large share were and are lockdown deaths as opposed to C19 deaths. That’s tragic. The CDC has done the country a massive disservice by creating “special rules” for attributing cause-of-death to C19. If reported C19 fatality rates reflected the same rules applied to other conditions, our approach to managing the pandemic surely would have inflicted far less damage to health and economic well being.
I’ve said this before, but it bears repeating: allegations of the White House’s “poor leadership” and preparedness for COVID-19 (C19) are a matter of selective memory. At the link above, I “graded” Trump’s pandemic job performance through May. Among other things, I said:
“Many have criticized the Trump Administration for not being ‘ready’ for a pandemic. I assign no grade on that basis because absolutely no one was ready, at least not in the West, so there is no sound premise for judgement. I also view the very general charge that Trump did not provide “leadership” as code for either ‘I don’t like him’, or ‘he refused to impose more authoritarian measures’, like a full-scale nationwide lockdown. Such is the over-prescriptive instinct of the Left.”
The President of the United States does not have the constitutional authority to impose a national lockdown, though Trump himself seemed confused at times as to whether he had that power. However, on this basis at least, the ad nauseam denigration of his “leadership” is vapid. At this point, the course of the pandemic in the U.S. is less severe than in several other industrialized countries who didn’t even have Andrew Cuomo around to exacerbate the toll, and it’s still not as deadly in per capita terms as the Asian Flu of 1957-58.
Who exactly was “ready” for C19? Perhaps critics are thinking of South Korea, or parts of South Asia. Those countries might have been “ready” to the extent that they had significant prior exposure to SARS viruses. There was already some degree of immunological protection. Those countries also were exposed to an earlier genetic variant of C19 that was much less severe than the strain that hit most of the western world. These are hardly reasons to blame Trump for a lack of “readiness”.
A related charge I hear all the time is that Trump “ignored the advice of medical experts“, or that he “ignored the science“. Presumably, those “experts” include the darling of the Prescriptive Class, Dr. Anthony Fauci. On February 28, Dr Fauci said:
“Right now, at this moment, there’s no need to change anything you’re doing on a day by day basis.“
Likewise, Dr. Robert Redfield, Director of the Centers for Disease Control, said the following on February 27:
“The risk to the American public is low. We have an aggressive containment strategy that really has worked up to this time, 15 cases in the United States. Until the last case that we just had in Sacramento we hadn’t had a new case in two weeks.”
Then there is the World Health Organization, whichdownplayed the virus in January and February, and giving a convincing impression that it servied as a mouthpiece for the CCP.
In fact, the American people were badly harmed by wrongheaded decisions made by the “experts” at the CDC in January and February, when the agency insisted that testing could not proceed until a test of their own design was ready. Then, the first version it approved was discovered to be flawed! This set the testing effort back by well over a month, a delay that proved critical. It’s no exaggeration to say this bureaucratic overreach denied the whole country, and Trump, the information needed to properly assess the spread of the virus.
But let’s think about actual policy once it became clear that the virus was getting to be a serious matter in parts of the U.S. Here’s another excerpt from my post in May:
“Trump cannot be accused of ignoring expert advice through the episode. He was obviously on-board with Fauci, Dr. Deborah Birx, Dr. Robert Redfield, and other health care advisors on the ‘15 Days to Slow the Spread‘ guidelines issued on March 16. His messaging wavered during those 15 days, expressing a desire to fully reopen the nation by Easter, which Vice President Michael Pence later described as “aspirational”. Before the end of March, however, Trump went along with a 30-day extension of the guidelines. Finally, by mid-April, the White House released guidelines for ‘Opening Up America Again‘, which was a collaboration between Trump’s health care experts and the economic team. Trump agreed that the timeline for reopening should be governed by ‘the data’.”
We should give Trump credit for shutting down flights into the U.S. from China, where the virus originated, late in January. That was an undeniably prescient move. Let’s also not forget that the original intent of the “15 Days” was to prevent hospitals and other medical resources from being overwhelmed. Today, the data show a strong seasonal tendency to the spread of the virus, but medical resources are not close to being overwhelmed, our ability to treat the virus has vastly improved, and its consequences are much less deadly than in the spring. That’s good progress, whatever the President’s detractors may say.
More than anything else, what Trump’s COVID critics fail to understand is that the executive leader of a republic is not possessed of monarchical powers. And in the U.S., the Constitution provides an additional layer of sovereignty for member states of the Union, a manifestation of the federalist principals without which the Union would not have been possible. The 15-day guidelines produced by the White House, and the guidelines for reopening, were consistent with this framework. The states have adapted their own policies to actual conditions and, if their leaders haven’t worn out their goodwill among voters, internal political realities. Those adaptations were often bad from my perspective, or even tyrannical, but sometimes good. That is exactly how our federalist system was designed to work.
Many haven’t quite gathered it in, but our public education system is an ongoing disaster for many low-income and minority students and families. The pandemic, however, is creating a major upheaval in K-12 education that might well benefit those students in the end. But before I get into that, a quick word about National Public Radio (NPR): it doesn’t make its political leanings a secret, which is why it should not be supported by taxpayers. Yes, like many other mainstream media outlets, NPR serves as a political front organization for Democrats (and worse).
Last week, NPR did a segment on “learning pods”, which I’d describe as private adaptations to the failure of many public schools (and teachers’ unions) to do their job during the pandemic. Glenn Reynolds passed along an interpretation of that NPR segment from a friend on Facebook, which I quote in its entirety below (bold emphasis mine). It was either this segment or else NPR has taken it down … but that link more or less matches the description. The post is somewhat satiric, but it captures much of what was actually said:
“Hilarious NPR, last week’s edition. They had an hour-long segment on learning pods. Participants: Host (white woman), Black Woman Activist, Asian Woman Parent, School-System Man.
Host: In wealthy areas, parents get together and organize learning pods. What do we make of it?
School-System Man: Inequitable! Inappropriate! Bad! We do not support it!
Asian Woman Parent: Equity requires that we form these pods to educate our own children! Otherwise, only the rich can get education! Rich bad!
Host: Rich bad.
School-System Man: Rich horrible! They withdraw kids from public schools during the pandemic, so schools have less money!
Asian Woman Parent: We have no choice. You are not teaching.
Host: But what are you doing for the equity?
Asian Woman Parent: Why are the parents supposed to be doing something for the equity? That’s why we pay taxes, so professionals do something!
School-System Man: We cannot fix equity if you are clandestinely educating your own children, but not everyone else’s children!
Asian Woman Parent: The proper solution would have been to end the pandemic. But Trump did not end the pandemic. So, we must do learning pods. As soon as the pandemic is over, we’ll get back to normal, and everyone will catch up.
Everyone [with great relief]: Trump bad. Bad.
Black Woman Activist: No, wait a minute. This sounds as though in a regular school year, black children get good education. And they are getting terrible education! Unacceptable!
Host: Bad Trump!
Black Woman Activist: Foggeraboutit! It’s not Trump! It’s always been terrible! Black children are dumped into horrible public schools, where nobody is teaching them! So, my organization is now helping organize these learning pods for minority kids everywhere.
School-System Man [cautiously]: This is only helping Trump…
Black Woman Activist: Forget Trump! Don’t tell me black kids get no education because things are not normal now. When things were normal, their education was just as bad!
School-System Man: Whut??? How dare you! Our public schools are the best thing that ever happened to black children.
Asian Woman Parent: I’ll second that. Public schools in my neighborhood are just svelte.
Black Woman Activist: That’s the point! You live in a rich suburb, and your kids get a great public school! Black kids don’t!
Asian Woman Parent: If Trump managed the pandemic properly, we would not be having this conversation.
Host: Bad Trump!
Everyone: Bad Trump!
The end.”
Ah yes, so we’re back to blaming Donald Trump for following the advice of his medical experts, most prominently Dr. Anthony Fauci. And, while we’re at it, let’s blame Mr. Trump for following federalist principles by deferring to state and local governments to deal flexibly with the varying regional conditions of the pandemic, rather than ruling by federal executive edict. Of course, some of those state and local officials botched it, such as Andrew Cuomo. That’s tragic, but had Trump followed a more prescriptive tack, the howling from the Left would have been even more deafening.
We know that children are at little risk from the coronavirus. Nor do they seem to transmit the virus like older individuals, but teachers unions are adamant that the risks their members face at school would far exceed those shouldered by other “essential” workers. And the unions, not shy about partisanship even while representing public employees, want nothing more than to see Trump lose the election. So the unions and the schools districts they seem to control hold parents hostage. They collect their tax revenue and salaries while delivering virtual service at lower standards than usual, or no service at all. (Of course, public schools in some parts of the country are in session.)
The teachers’ unions and public schools might get their comeuppance. The situation represents a tremendous opportunity for private schools, home schooling, and innovative schooling paradigms. Many private schools are holding classes in-person, more parents are homeschooling, and alternative arrangements like learning pods have formed, many of which are quite cost-effective.
Pressure is building to allow education dollars to follow individual students, not simply to flow to specific government schools. You can buy a decent K-12 education for $12,000 a year or so, and it’s likely to be a better education than you’ll get in many public schools. (One of the panelists on the NPR segment smugly called this an “insidious temptation”). At long last, parents would be allowed real choice in educating their children, and at long last schools would be incentivized to compete for those students. That might be one of the best things to come out of the pandemic.
Policymakers, public health experts, and the media responded to the coronavirus in ways that have often undermined public health and magnified the deadly consequences of the pandemic. Below I offer several examples of perverse politics and policy prescriptions, and a few really bad decisions by certain elected officials. Some of the collateral damage was intentional and motivated by an intent to inflict political damage on Donald Trump, and people of good faith should find that grotesque no matter their views on Trump’s presidency.
“On May 27, I published an article in theAmerican Journal of Epidemiology(AJE) entitled, ‘Early Outpatient Treatment of Symptomatic, High-Risk COVID-19 Patients that Should be Ramped-Up Immediately as Key to the Pandemic Crisis.’ That article, published in the world’s leading epidemiology journal, analyzed five studies, demonstrating clear-cut and significant benefits to treated patients, plus other very large studies that showed the medication safety. …
Since [then], seven more studies have demonstrated similar benefit. In a lengthy follow-up letter, also published by AJE, I discuss these seven studies and renew my call for the immediate early use of hydroxychloroquine in high-risk patients.”
Risch is careful to couch his statements in forward-looking terms, but this also implies that tens of thousands of lives could have been saved, or patients might have recovered more readily and without lasting harm, had use of the drug not been restricted. The FDA revoked its Emergency Use Authorization for HCQ on June 15th, alleging that it is not safe and has little if any benefit. An important rationale cited in the FDA’s memo was an NIH study of late-stage C19 patients that found no benefit and potential risks to HCQ, but this is of questionable relevance because the benefit appears to be in early-stage treatment or prophylaxis. Poor research design also goes for this study and this study, while this study shared in some shortcomings (e.g., and no use of and/or controls for zinc) and a lack of statistical power. Left-wing outlets like Politico seemed almost gleeful, and blissfully ignorant, in calling those studies “nails in the coffin” for HCQ. Now, I ask: putting the outcomes of the research aside, was it really appropriate to root against a potential treatment for a serious disease, especially back in March and April when there were few treatment options, but even now?
Then we have the state governors who restricted the use of HCQ for treating C19, such as Gretchen Whitmer (MI) and Steve Sisolak (NV). Andrew Cuomo (NY) decided that HCQ could be dispensed only for hospital use, exactly the wrong approach for early stage treatment. And all of this resistance was a reaction to Donald Trump’s optimism about the promise of HCQ. Yes, there was alarm that lupus patients would be left without adequate supplies, but the medication is a very cheap, easy to produce drug, so that was never a real danger. Too much of the media and politicians have been complicit in denying a viable treatment to many thousands of C19 victims. If you were one of the snarky idiots putting it down on social media, you are either complicit or simply a poster child for banal evil.
Seeding the Nursing Homes
The governors of several states issued executive orders to force nursing homes to accept C19 patients, which was against CMS guidance issued in mid-March. The governors were Andrew Cuomo (NY), Gretchen Whitmer (MI), Gavin Newsom (CA), Tom Wolf (PA), and Phil Murphy (PA). This was a case of stupidity more than anything else. These institutions are home to the segment of the population most vulnerable to the virus, and they have accounted for about 40% of all C19 deaths. Nursing homes were ill-prepared to handle these patients, and the governors foolishly and callously ordered them to house patients who required a greater level of care and who represented an extreme hazard to other residents and staff.
Party & Protest On
Then of course we had the mayor of New York City, Bill De Blasio, who urged New Yorkers to get out on the town in early March. That was matched in its stupidity by the array of politicians and health experts who decided, having spent months proselytizing the need to “stay home”, that it was in their best interests toendorse participation in street protests that were often too crowded to maintain effective social distance. That’s not a condemnation of those who sought to protest peacefully against police brutality, but it was not a good or consistent recommendation in the domain of public health. Thankfully, the protests were outside!
Testing, Our Way Or the Highway
The FDA and CDC were guilty of regulatory overreach in preventing early testing for C19, and were responsible for many lives lost early in the pandemic. By the time the approved CDC tests revealed that the virus was ramping up drastically in March, the country was already behind in getting a handle on the spread of the virus, quarantining the infected, and tracing their contacts. There is no question that this cost lives.
Masks… Maybe, But Our Way Or the Highway
U.S. public health authorities were guilty of confused messaging on the efficacy of masks early in the pandemic. As Joel Zinberg notes in City Journal, Anthony Fauci admitted that his own minimization of the effectiveness of masks was motivated by a desire to prevent a shortage of PPE for health care workers:
“In discouraging mask use, Fauci—for decades, the nation’s foremost expert on viral infectious diseases—was not acting as a neutral interpreter of settled science but as a policymaker, concerned with maximizing the utility of the limited supply of a critical item. An economist could have told him that there was no need to misinform the public. Letting market mechanisms work and relaxing counterproductive regulations would ease shortages. Masks for health-care workers would be available if we were willing to pay higher prices; those higher prices, in turn, would elicit more mask production.”
Indeed, regulators made acquisition of adequate supplies of PPE more difficult than necessary via compliance requirements, “price gouging” rules, and import controls.
Bans on Elective Surgery
Another series of unnecessary deaths was caused by various bans on elective surgeries across the U.S. (also see here), and we’re now in danger of repeating that mistake. These bans were thought to be helpful in preserving hospital capacity, but hospitals were significantly underutilized for much of the pandemic. Add to that the fright inspired by official reaction to C19, which keeps emergency rooms empty, and you have a universe of diverse public health problems to grapple with. As I said on this blog a couple of months ago:
“… months of undiagnosed cardiac and stroke symptoms; no cancer screenings, putting patients months behind on the survival curve; deferred procedures of all kinds; run-of-the-mill infections gone untreated; palsy and other neurological symptoms anxiously discounted by victims at home; a hold on treatments for all sorts of other progressive diseases; and patients ordinarily requiring hospitalization sent home. And to start back up, new health problems must compete with all that deferred care. Do you dare tally the death and other worsened outcomes? Both are no doubt significant.”
Lockdowns
The lockdowns were unnecessary and ineffectual in their ability to control the spread of the virus. A study of 50 countries published by The Lancet last week found the following:
“Increasing COVID-19 caseloads were associated with countries with higher obesity … median population age … and longer time to border closures from the first reported case…. Increased mortality per million was significantly associated with higher obesity prevalence … and per capita gross domestic product (GDP) …. Reduced income dispersion reduced mortality … and the number of critical cases …. Rapid border closures, full lockdowns, and wide-spread testing were not associated with COVID-19 mortality per million people.”
That should have been obvious for a virus that holds little danger for prime working-age cohorts who are most impacted by economic lockdowns.
Like the moratoria on elective surgeries, lockdowns did more harm than good. Livelihoods disappeared, business were ruined, savings were destroyed, dreams were shattered, isolation set in, and it continues today. These kinds of problems are strongly associated with health troubles, family dysfunction, drug and alcohol abuse, and even suicide. It’s ironic that those charged with advising on matters pertaining to public health should focus exclusively on a single risk, recommending solutions that carry great risk themselves without a second thought. After all, the protocol in reviewing new treatments sets the first hurdle as patient safety, but apparently that didn’t apply in the case of shutdowns.
Even as efforts were made to reopen, faulty epidemiological models were used to predict calamitous outcomes. While case counts have risen in many states in the U.S. in June and July, deaths remain far below model predictions and far below deaths recorded during the spring in the northeast.
One last note: I almost titled this post “Attack of the Killer Morons”, but as a concession to what is surely a vain hope, I decided not to alienate certain readers right from the start.
It’s a bit early to fully evaluate President Trump’s performance in dealing with the coronavirus pandemic, but there are a number of criteria on which I might assign marks. I’ll address some of those below, but in so doing I’m reminded of Jerry Garcia’s quip that he was “shopping around for something no one will like.” That might be how this goes. Of course, many of the sub-topics are worthy of lengthier treatment. The focus here is on the pandemic and not more general aspects of his performance in office, though there is some unavoidable overlap.
General “Readiness”
Many have criticized the Trump Administration for not being “ready” for a pandemic. I assign no grade on that basis because absolutely no one was ready, at least not in the West, so there is no sound premise for judgement. I also view the very general charge that Trump did not provide “leadership” as code for either “I don’t like him”, or “he refused to impose more authoritarian measures”, like a full-scale nationwide lockdown. Such is the over-prescriptive instinct of the Left.
Equally misleading is the allegation that Trump had “disbanded” the White House pandemic response team, and I have addressed that here. First, while the NSC would play a coordinating role, pandemic response is supposed to be the CDC’s job, when it isn’t too busy with diseases of social injustice to get it done. Second, it was John Bolton who executed a reorganization at the NSC. There were two high profile departures from the team in question at the time, and one one was a resignation. Most of the team’s staff remained with the NSC with the same duties as before the reirganization.
Finally, there was the matter of a distracting impeachment on false charges. This effort lasted through the first three years of Trump’s administration, finally culminating in January 2020. Perhaps the Administration would have had more time to focus on what was happening in China without the histrionics from the opposition party. So whatever else I might say below, these factors weigh toward leniency in my appraisal of Trump’s handing of the virus.
Messaging: C
As usual, Trump’s messaging during the pandemic was often boorish and inarticulate. His appearances at coronavirus briefings were no exception, often cringeworthy and sometimes featuring misinterpretations of what his team of experts was saying. He was inconsistent in signaling optimism and pessimism, as were many others such as New York Governor Andrew Cuomo and New York City Mayor Bill De Blasio. It shifted from “the virus is about like the flu” in February to a more sober assessment by mid-March. This was, however, quite consistent with the messaging from Dr. Anthony Fauci over the same time frame, as well as the World Health Organization (WHO). Again, no one really knew what to expect, so it’s understandable. A great deal of that can be ascribed to “the fog of war”.
Delegation and Deference: B
Trump cannot be accused of ignoring expert advice through the episode. He was obviously on-board with Fauci, Dr. Deborah Birx, Dr. Robert Redfield, and other health care advisors on the “15 Days to Slow the Spread” guidelines issued on March 16. His messaging wavered during those 15 days, expressing a desire to fully reopen the nation by Easter, which Vice President Michael Pence later described as “aspirational”. Before the end of March, however, Trump went along with a 30-day extension of the guidelines. Finally, by mid-April, the White House released guidelines for “Opening Up America Again“, which was a collaboration between Trump’s health care experts and the economic team. Trump agreed that the timeline for reopening should be governed by “the data”. There is no question, however, that Trump was chomping at the bit for reopening at several stages of this process. I see value in that positioning, as it conveys an intent to reopen asap and that people should have confidence in progress toward that goal.
International Travel Bans: A
If anyone wonders why the world was so thoroughly blindsided by the coronavirus, look no further than China’s failure to deliver a proper warning as 2019 drew to a close. Wuhan, China was ground zero; the virus spread to the rest of the world with travelers out of Wuhan and other Chinese cities. The White House announced severe restrictions on flights from China on January 31, including a two-week quarantine for returning U.S. citizens. In retrospect, it wasn’t a minute too soon, yet for that precaution, Trump was attacked as a racist by the Left. In early February, WHO actually said travel bans were unnecessary, among other missteps. Other bans were instituted on entry from Iran and Brazil, as well as entry from Europe in early March, as countries around the globe closed their borders. Trump’s actions on incoming travelers were prescient, so I’ll score this one for Trump. Some of these travel restrictions can and should be eased now, and certainly that is expected in coming months, so we’ll see how well that process is managed.
Deference to States: A-
As a federalist, I was pleased that Trump and his team left most of the specifics on closures and bans on public gatherings up to state and local governments. That allowed more targeted mitigation efforts as dictated by local conditions and, to some extent, public opinion. This is a classic case of “laboratory federalism” whereby the most effective policies can be identified, though as we’ve seen, there’s no guarantee less successful states will emulate them. I grade Trump well on this one.
On reopening, too, Trump has been a consistent advocate of allowing flexility where local conditions permit, though he wrongly claimed he had “total authority” over ending social distancing rules. It’s hard to square that remark with his general stand on the issue of autonomy except as a tactic to strong-arm certain governors on other points.
CDC/FDA Snafus: D
I applaud the Administration for its emphasis on the salutary effects of deregulation, but Trump went along with some major pieces of “expert advice” that were not only poor from regulatory perspective, but an affront to federalism. One was a directive issued by the CDC to delay “all elective surgeries, non-essential medical, surgical, and dental procedures during the 2019 Novel Coronavirus (COVID-19) outbreak“. (See my post “Suspending Medical Care in the Name of Public Health“.)
This is exactly the kind of “one size fits all” regulatory policy that has proven so costly, sacrificing not just economic activity but lives and care for the sick, creating avoidable illnesses and complications. The idea was to assure that adequate health care resources were available to treat an onslaught of coronavirus patients, but that was unneeded in most jurisdictions. And while the contagion was in it’s early “exponential” phase at the time, a more nuanced approach could have been adopted to allow different geographic areas and facilities more discretion, especially for different kinds of patients, or perhaps something less than a complete suspension of care. In any case, the extensions into May were excessive. I must grade Trump poorly for allowing this to happen, despite what must have been extreme pressure to follow “expert advice” on the point and the others discussed earlier.
That’s not the only point on which I blame Trump for caving to the CDC. In a case of massive regulatory failure, the CDC and FDA put the U.S. well over a month behind on testing when the first signs of the virus appeared here. Not only did they prohibit private labs and universities from getting testing underway, insisting on exclusive use of the CDC’s own tests, they also distributed faulty tests in early February that took over a month to replace. The FDA also enforced barriers to imported N95-type masks during the pandemic. Trump tends to have a visceral understanding of the calcifying dangers of regulation, but he let the so-called “experts” call the shots here. Big mistake, and Trump shares the blame with these agencies.
Health Resources: B-
Managing the emergency distribution of PPE and ventilators to states did not go as smoothly as might have been hoped. The shortage itself left FEMA with the unenviable task of allocating quantities that could never satisfy all demands. A few states were thought to have especially acute needs, but there was also an obligation to hold stockpiles against potential requests from other states. In fact, a situation of this kind creates an incentive for states to overstate their real needs, and there are indications that such was the case. Trump sparred with a few governors over these allocations. There is certainly blame to be shared, but I won’t grade Trump down for this.
Vaccines and Treatments: C+
The push to develop vaccines might not achieve success soon, if ever, but a huge effort is underway. Trump gets some of the credit for that, as well as the investment in capacity now to produce future vaccine candidates in large quantities. As for treatments, he was very excited about the promise of hydroxychloraquine, going so far as to take it himself with zinc, a combination for which no fully randomized trial results have been reported (the recent study appearing in the Lancet on HCQ taken by itself has been called into question). Trump also committed an unfortunate gaffe when the DHS announced the results of a study showing that sunlight kills coronavirus in a matter of minutes, as do bleach and other disinfectants. Trump mused that perhaps sunlight or some form of disinfectant could be used as a treatment for coronavirus patients. He might have been thinking about an old and controversial practice whereby blood is exposed to UV light and then returned to the body. Later, he said he used the term “disinfectant” sarcastically, but he probably meant to say “euphemistically” …. I’m not sure he knows the difference. In any case, his habit of speculating on such matters is often unhelpful, and he loses points for that.
Fiscal Policy: B
The several phases of the economic stimulus program were a collaboration between the Trump Administration and Congress. A reasonably good summary appears here. The major parts were the $2.3 trillion CARES Act in late March and a nearly $500 billion supplemental package in late April. These packages were unprecedented in size. Major provisions were direct cash payments and the Paycheck Protection Program (PPP), which provides loans and grants to small businesses. The execution of both was a bit clunky, especially PPP, which placed a burden on private banks to extend the loans but was sketchy in terms of qualifications. The extension of unemployment compensation left some workers with more benefits than they earned in their former jobs, which could be an impediment to reopening. There were a number of other reasonable measures in these packages and the two smaller bills that preceded them in March. A number of these measures were well-targeted and inventive, such as waiving early withdrawal penalties from IRA and 401(k) balances. The Trump Administration deserves credit for helping to shape these efforts as well as others taken independently by the executive branch.
Trump’s proposal to suspend payroll taxes did not fly, at least not yet. The idea is to reduce the cost of hiring and increase the return to work, if only temporarily. This is not a particularly appealing idea because so much of the benefits would flow to those who haven’t lost their jobs. It could be improved if targeted at new hires and rehires, however.
Trump’s proposal to grant liability waivers to reopened private businesses is extremely contentious, but one I support. Lockdowns are being eased under the weight of often heavy public and private regulation of conduct. As John Cochrane says in “Get Ready for the Careful Economy“:
“One worry on regulation is that it will provide a recipe for a wave of lawsuits. That may have been a reason the Administration tried to hold back CDC guidance. A long, expensive, and impractical list of things you must do to reopen is catnip when someone gets sick and wants to blame a business. Show us the records that you wiped down the bathrooms every half hour. A legal system that can sue over talcum powder is not above this.”
Indeed, potential liability might represent a staggering cost to many businesses, one that might not be insurable. Accusations of negligence, true or false, can carry significant legal costs. Customers and employees, not just businesses, must accept some of the burden of risks of doing business. I give Trump good marks for this one, but we’ll see if it goes anywhere.
Some of the proposals for new stimulus legislation from democrats are much worse, including diversity initiatives, massive subsidies for “green” technologies, and bailouts for state and local government for unfunded pension liabilities. None of these has anything to do with the virus. The burden of pension shortfalls in some states should not fall on taxpayers nationwide, but on the states that incurred them. The Trump Administration and congressional Republicans should continue resisting these opportunistic proposals.
The Grade
Without assigning weights to the sub-topics covered above, I’d put the overall grade for Trump and his Administration’s handling of matters during the pandemic at about a B-, thus far. When it comes to politics, it’s often unfair to credit or blame one side for the promulgation of an overall set of policies. Nevertheless, I think it’s fair to say that Trump, could have done much better and could have done much worse. We will learn more with the passage of time, the continued evolution of the virus, the development of treatments or vaccines, and the course of the economy.
Here’s an all-time dumbass bromide: “If it saves only one life, it’s worth it.” New York Governor Andrew Cuomo said it last week in a bit of sanctimonious posturing intended for consumption by the unthinking. A variant on this is, “You can’t put a value on a human life,” and Cuomo said that too. But of course we do that every day. Yes, we weigh lives against costs, and we must. Each and every decision involving any personal or public health risk entails an implicit and sometimes explicit valuation of human life. There are few costless decisions in a world of scarce resources, and lives are often one of those costs. These might be matters of probability in an ex ante sense, which might make it more palatable. Ex post, they add up to real lives.
Imagine a world in which we spared no expense to save lives. We’d shift massive resources into health care to the detriment of all production and consumption that does not save lives. No precaution would be too conservative. No driving or biking, because those prohibitions would save many lives. Many risky construction and maintenance jobs would be off limits. No smoking, of course, and no drinking! No chips! Every BMI greater than 25 and you’re off to mandatory fat camp. Sadly, the effort to save a life is sometimes fruitless, but as long as there’s a chance, we’d try and try, providing mechanical life support to every patient hanging on by a tattered thread. No, we don’t do these things because it’s too damn costly.
We face an infinite number of tradeoffs in medical care and in public health more generally. The question “Who Shall Live?” must be answered every day when deciding how health care resources are to be allocated. No matter how you answer that question, certain lives will be lost as the cost of meeting your preferred medical objectives. You can’t meet them all. Resources are scarce — or in more everyday language, budgets are tight.
So human life is often assigned an implicit or shadow value in decision making. But even explicit assignment of economic value to human life is not uncommon. Valuing lives is a standard practice in cost-benefit analysis. It’s also quite common for life values to be estimated as part of forensic analyses in support of legal proceedings.
Andrew Cuomo surely knows all this. That makes his statements all the more disingenuous. This article in The Nation from the end of March implies that Cuomo has valued life all too cheaply in light of his past budget proposals for health care programs. Along the same lines, see this eye-opening critique of the policies Cuomo has pursued that left NY poorly prepared for a pandemic. And now, he’d like to keep his costly lockdown order in place even if it saves “just one life”.
Beyond all that, Cuomo is a stupendous hypocrite, asserting that life is too precious to spare any expense after signing an order in March requiring nursing homes to accept individuals with active Covid infections. Nursing homes have been the very hottest of spots for Covid infections and deaths, so the order was glaringly dismissive in valuing the lives of vulnerable nursing home residents. The rationale for the order was to save hospital beds, but there was no shortage.
In fairness, Cuomo was also clamoring for assistance to add hospital capacity. Millions were spent to convert the Javits Center to a temporary field hospital and to bring a U.S. Navy hospital ship up the Hudson, but they went almost completely unused. Why not send the elderly patients there, instead of back to the nursing homes?
Recently, Cuomo felt it necessary to demonstrate his anti-Western bona fides by labeling the coronavirus the “European Virus“. He must think that’s a clever poke in the eye to those who prefer “Wuhan Virus”, though it is quite correct (and not the least bit “racist”) to note that the virus originated in Wuhan, China. For what it’s worth, the genome of the European strain, like the others that hit New York, differs by less than 12 out of 30,000 base-pairs of DNA from the original Wuhan strain. And of course the New York metropolitan area has made a massive contribution to the U.S. case load and death toll from the virus. Travelers from New York did much to spread Covid-19 to the rest of the country. So, as some have suggested, perhaps a better name might be “New York Virus”.
Andrew Cuomo is nothing if not a politician, and I suppose he’s just behaving like one. I probably wouldn’t gripe were it not for the minions who fall for Cuomo’s sham virtue. But it’s worse than that: the claim that public intervention at any cost is worthwhile if it saves “just one life” is a deeply statist sentiment.
My original post on the dominance of voluntary social distancing over the mandated variety appears below. That dominance is qualified by the greater difficulty of engaging in certain activities when they are outlawed by government, or when the natural locations of activities are declared off-limits. Nevertheless, as with almost all regulation, people make certain “adjustments” to suit themselves (sometimes involving kickbacks to authorities, because regulation does nothing so well as creating opportunities for graft). Those “adjustments” often lead to much less desirable outcomes than the original, unregulated state. In the case of a pandemic, however, it’s tempting to view such unavoidable actions as a matter of compromise.
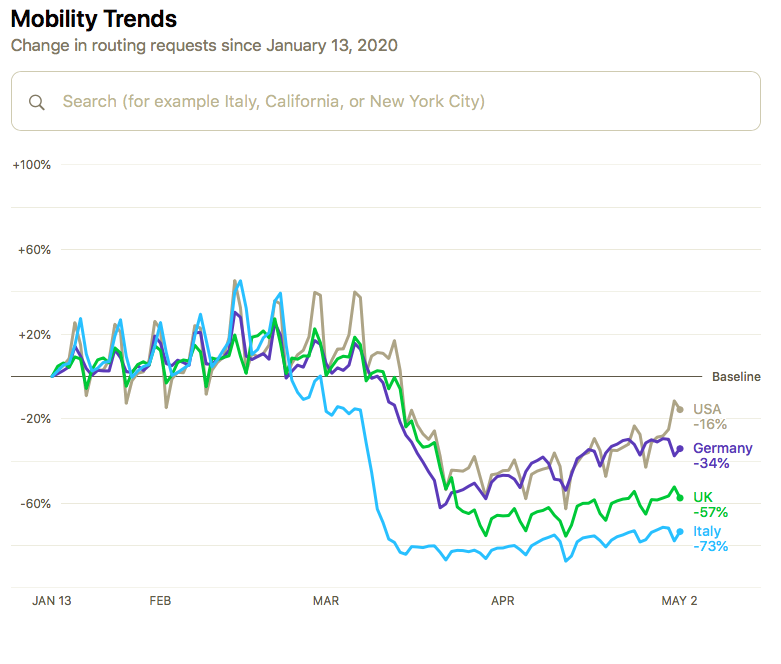
I say this now because the voluntary social distancing preceding most government lockdown orders in March (discussed in the post below) is subject to a degree of self-reversal. Apple Mobility Data suggests that something like that was happening throughout much of April, as shown in the chart at the top of this post. Now, in early May, the trend is likely to continue as some of the government lockdown mandates are being lifted, or at least loosened.
An earlier version of the chart above appeared in a Forbes article entitled, “Apple Data Shows Shelter-In-Place Is Ending, Whether Governments Want It To Or Not“. The author, John Koetsier, noted the Apple data are taken from map searches, so they may not be reliable indicators of actual movement. But he also featured some charts from Foursquare, which showed actual visits to various kinds of destinations, and some of theoe demonstrate the upward trend in activity.
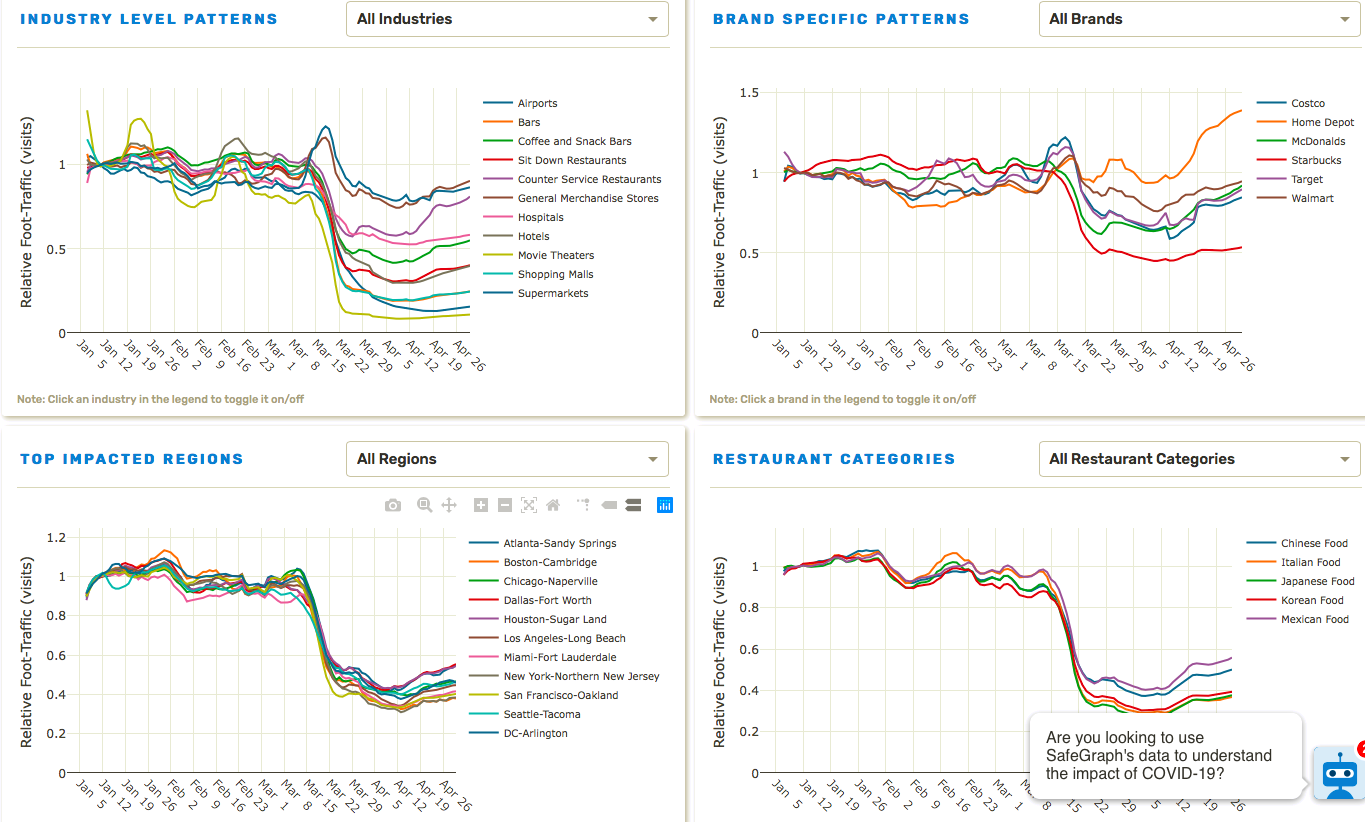
In the original post below, I used SafeGraph charts lifted from a paper I described there. The four charts below are available on the SafeGraph website, which offered the services of the friendly little robot in the lower right-hand corner, but I demurred. You’ll probably need to click on the image to read the detail. They show more granular information by industry, brand, region, and restaurant categories. The upward trends are evident in quite a few of the series.
I should qualify my interpretation of the charts above and those in my original post: First, nine states did not have stay-at-home orders, though a few of those had varying restrictions on individuals and on the operation of “non-essential” businesses. The five having no orders of any kind (that I can tell) are lightly-populated, very low-density states, so the vast majority of the U.S. population was subject to some sort of lockdown measure. Second, eight states began to ease or lift orders in the last few days of April, Georgia and Colorado being the largest. Therefore, at the tail end, a small part of the increase in activity could be related to those liberalizations. Then again, it might have happened anyway.
The authoritarian impulse to shut everything down was largely unnecessary, and it did not accomplish much that voluntary distancing hadn’t accomplished already (again, see below). Healthy people need to stop cowering and take action. That includes the non-elderly and those free of underlying health conditions. Sure, take precautions, keep your distance, but get out of your home if you can. Get some sunny Vitamin D.
Committing yourself to the existence of a shut-in is not healthy, not wise, and it might destroy whatever wealth you possess if you are a working person. The data above show that people are recognizing that fact. As much as the Left wishes it were so, government seldom “knows better”. It is least effective when it uses force to suppress voluntary behavior; it is most effective when it follows consensus, and especially when it protects the rights of individuals to make their own choices where no consensus exists.
Last week’s post follows:
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
How much did state and local governments accomplish when they decided to issue stay-at-home orders? Perhaps not much. That’s the implication of data presented by the authors of “Internal and external effects of social distancing in a pandemic” (starts on page 22 in the linked PDF). Social distancing began in the U.S. in a series of voluntary, private actions. Government orders merely followed and, at best, reinforced those actions, but often in ham-handed ways.
The paper has a broader purpose than the finding that social distancing is often a matter of private initiative. I’ll say a bit more about it, but you can probably skip the rest of this paragraph without loss of continuity. The paper explores theoretical relationships between key parameters (including a social distancing construct) and the dynamics of a pandemic over time in a social welfare context. The authors study several alternatives: a baseline in which behavior doesn’t change in any way; a “laissez faire” path in which actions are all voluntary; and a “socially optimal” path imposed by a benevolent and all-knowing central authority (say what???). I’d offer more details, but I’ll await the coming extension promised by the authors to a world in which susceptible populations are heterogenous (e.g., like Covid-19, where children are virtually unaffected, healthy working age adults are roughly as at-risk as they are to the flu, and a population of the elderly and health-compromised individuals for which the virus is much more dangerous than the flu). In general, the paper seems to support a more liberalized approach to dealing with the pandemic, but that’s a matter of interpretation. Tyler Cowen, who deserves a hat-tip, believes that reading is correct “at the margin”.
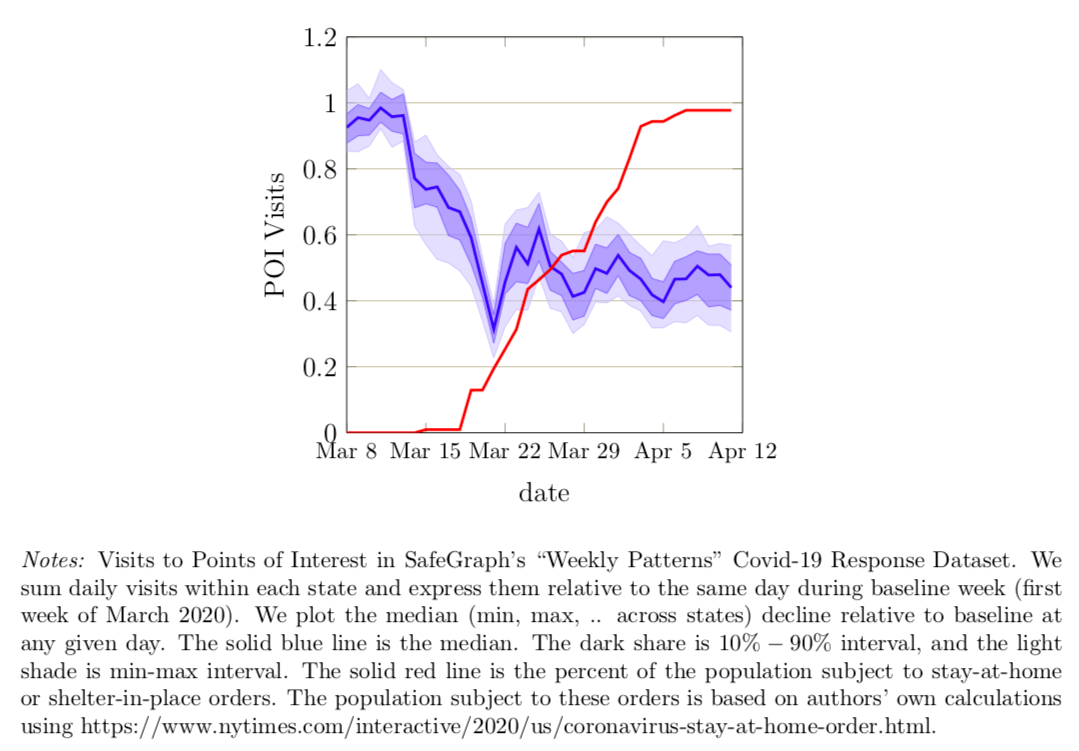
Let’s look at some of the charts the authors present early in the paper. The data on social distancing behavior comes from Safegraph, a vendor of mobility data taken from cell phone location information. This data can be used to construct various proxies for aggregate social activity. The first chart below shows traffic at “points of interest” (POI) in the U.S. from March 8 to April 12, 2020. That’s the blue line. The red line is the percentage of the U.S. population subject to lockdown orders on each date. The authors explain the details in the notes below the chart:
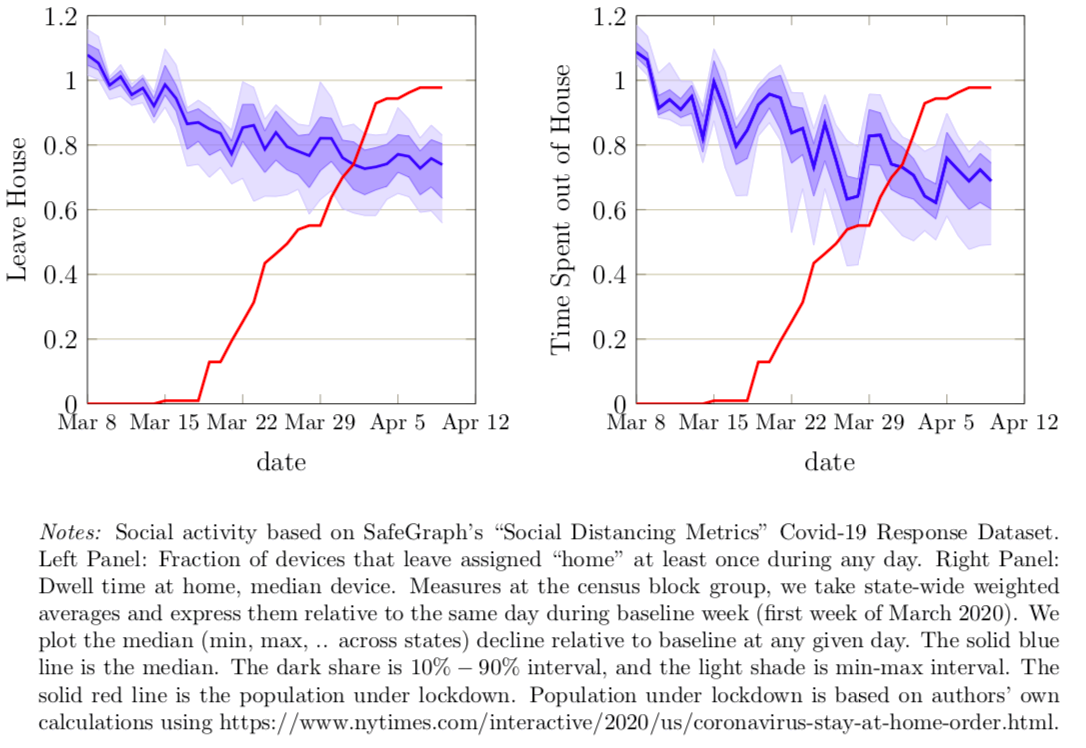
Clearly POI visits were declining sharply before any governments imposed their own orders. The next two charts show similar declines in the percent of mobile devices that leave “home” each day (“home” being the device’s dominant location during nighttime hours) and the duration over which devices were away from “home”, on average.
So all of these measures of social activity began declining well ahead of the government orders. The authors say private social distancing preceded government action in all 50 states. POI traffic was down almost 40% by the time 10% of the U.S. population was subject to government orders, and those early declines accounted for the bulk of the total decline through April 12. The early drops in the two away-from-home measures were 15-20%, again accounting for well over half of the total decline.
The additional declines beyond that time, to the extent they can be discerned, could be either trends that would have continued even in the absence of government orders or reinforcing effects the orders themselves. This does not imply that lockdown orders have no effects on specific activities. Rather, it means that those orders have minor incremental effects on measures of aggregate social activity than the voluntary actions already taken. In other words, the government lockdowns are largely a matter of rearranging the deck chairs, or, that is to say, their distribution.
Many private individuals and institutions acted early in response to information about the virus, motivated by concerns about their own safety and the safety of family and friends. The public sector in the U.S. was not especially effective in providing information, with such politicos as President Donald Trump, Nancy Pelosi, Andrew Cuomo, Bill De Blasio, and the mayor of New Orleans minimizing the dangers into the month of March, and some among them encouraging people to get out and celebrate at public events. Even Anthony Fauci minimized the danger in late February (not to mention the World Health Organization). In fact, “the scientists” were as negligent in their guidance as anyone in the early stages of the pandemic.
When lockdown orders were issued, they were often arbitrary and nonsensical. Grocery stores, liquor stores, and Wal Mart were allowed to remain open, but department stores and gun shops were not. Beaches and parks were ordered closed, though there is little if any chance of infection outdoors. Lawn care services, another outdoor activity, were classified as non-essential in some jurisdictions and therefore prohibited. And certain personal services seem to be available to public officials, but not to private citizens. The lists of things one can and can’t buy truly defies logic.
“We’re talking about lockdown powers (at both the federal and state level): the ability to suspend the Constitution, indefinitely detain American citizens, bypass the courts, quarantine whole communities or segments of the population, override the First Amendment by outlawing religious gatherings and assemblies of more than a few people, shut down entire industries and manipulate the economy, muzzle dissidents, ‘stop and seize any plane, train or automobile to stymie the spread of contagious disease,’…”
That is fearsome indeed, and individuals can accomplish distancing without it. If you are extremely risk averse, you can distance yourself or take other precautions to remain protected. You can either take action to isolate yourself or you can decide to be in proximity to others. The more risk averse among us will internalize most of the cost of voluntary social distancing. The less risk averse will avoid that cost but face greater exposure to the virus. Of course, this raises questions of public support for vulnerable segments of the population for whom risk aversion will be quite rational. That would certainly be a more enlightened form of intervention than lockdowns, though support should be offered only to those highly at-risk individuals who can’t support themselves.
Christopher Phelan writes of three rationales for the lockdowns: buying time for development of a vaccine or treatments; reducing the number of infected individuals; and to avoid overwhelming the health care system. Phelan thinks all three are of questionable validity at this point. A vaccine might never arrive, and Phelan is pessimistic about treatments (I have more hope in that regard). Ultimately a large share of the population will be infected, lockdowns or not. And of course the health care system is not overwhelmed at this point. Yes, those caring for Covid patients are under a great stress, but the health care system as a whole, and patients with other maladies, are currently suffering from massive under-utilization.
If you wish to be socially distant, you are free to do so on your very own. Individuals are quite capable of voluntary risk mitigation without authoritarian fiat, as the charts above show. While private actors might not internalize all of the external costs of their activities, government is seldom capable of making the appropriate corrections. Coercion to enforce the kinds of crazy rules that have been imposed during this pandemic is the kind of abuse of power the nation’s founders intended to prevent. Reversing those orders can be difficult, and the precedent itself becomes a threat to future liberty. Nevertheless, we see mounting efforts to resist by those who are harmed by these orders, and by those who recognize the short-sighted nature of the orders. Private incentives for risk reduction, and private evaluation of the benefits of social and economic activity, offer superior governance to the draconian realities of lockdowns.
How much did state and local governments accomplish when they decided to issue stay-at-home orders? Perhaps not much. That’s the implication of data presented by the authors of “Internal and external effects of social distancing in a pandemic” (starts on page 22 in the linked PDF). Social distancing began in the U.S. in a series of voluntary, private actions. Government orders merely followed and, at best, reinforced those actions, but often in ham-handed ways.
The paper has a broader purpose than the finding that social distancing is often a matter of private initiative. I’ll say a bit more about it, but you can probably skip the rest of this paragraph without loss of continuity. The paper explores theoretical relationships between key parameters (including a social distancing construct) and the dynamics of a pandemic over time in a social welfare context. The authors study several alternatives: a baseline in which behavior doesn’t change in any way; a “laissez faire” path in which actions are all voluntary; and a “socially optimal” path imposed by a benevolent and all-knowing central authority (say what???). I’d offer more details, but I’ll await the coming extension promised by the authors to a world in which susceptible populations are heterogenous (e.g., like Covid-19, where children are virtually unaffected, healthy working age adults are roughly as at-risk as they are to the flu, and a population of the elderly and health-compromised individuals for which the virus is much more dangerous than the flu). In general, the paper seems to support a more liberalized approach to dealing with the pandemic, but that’s a matter of interpretation. Tyler Cowen, who deserves a hat-tip, believes that reading is correct “at the margin”.
Let’s look at some of the charts the authors present early in the paper. The data on social distancing behavior comes from Safegraph, a vendor of mobility data taken from cell phone location information. This data can be used to construct various proxies for aggregate social activity. The first chart below shows traffic at “points of interest” (POI) in the U.S. from March 8 to April 12, 2020. That’s the blue line. The red line is the percentage of the U.S. population subject to lockdown orders on each date. The authors explain the details in the notes below the chart:
Clearly POI visits were declining sharply before any governments imposed their own orders. The next two charts show similar declines in the percent of mobile devices that leave “home” each day (“home” being the device’s dominant location during nighttime hours) and the duration over which devices were away from “home”, on average.
So all of these measures of social activity began declining well ahead of the government orders. The authors say private social distancing preceded government action in all 50 states. POI traffic was down almost 40% by the time 10% of the U.S. population was subject to government orders, and those early declines accounted for the bulk of the total decline through April 12. The early drops in the two away-from-home measures were 15-20%, again accounting for well over half of the total decline.
The additional declines beyond that time, to the extent they can be discerned, could be either trends that would have continued even in the absence of government orders or reinforcing effects the orders themselves. This does not imply that lockdown orders have no effects on specific activities. Rather, it means that those orders have minor incremental effects on measures of aggregate social activity than the voluntary actions already taken. In other words, the government lockdowns are largely a matter of rearranging the deck chairs, or, that is to say, their distribution.
Many private individuals and institutions acted early in response to information about the virus, motivated by concerns about their own safety and the safety of family and friends. The public sector in the U.S. was not especially effective in providing information, with such politicos as President Donald Trump, Nancy Pelosi, Andrew Cuomo, Bill De Blasio, and the mayor of New Orleans minimizing the dangers into the month of March, and some among them encouraging people to get out and celebrate at public events. Even Anthony Fauci minimized the danger in late February (not to mention the World Health Organization). In fact, “the scientists” were as negligent in their guidance as anyone in the early stages of the pandemic.
When lockdown orders were issued, they were often arbitrary and nonsensical. Grocery stores, liquor stores, and Wal Mart were allowed to remain open, but department stores and gun shops were not. Beaches and parks were ordered closed, though there is little if any chance of infection outdoors. Lawn care services, another outdoor activity, were classified as non-essential in some jurisdictions and therefore prohibited. And certain personal services seem to be available to public officials, but not to private citizens. The lists of things one can and can’t buy truly defies logic.
“We’re talking about lockdown powers (at both the federal and state level): the ability to suspend the Constitution, indefinitely detain American citizens, bypass the courts, quarantine whole communities or segments of the population, override the First Amendment by outlawing religious gatherings and assemblies of more than a few people, shut down entire industries and manipulate the economy, muzzle dissidents, ‘stop and seize any plane, train or automobile to stymie the spread of contagious disease,’…”
That is fearsome indeed, and individuals can accomplish distancing without it. If you are extremely risk averse, you can distance yourself or take other precautions to remain protected. You can either take action to isolate yourself or you can decide to be in proximity to others. The more risk averse among us will internalize most of the cost of voluntary social distancing. The less risk averse will avoid that cost but face greater exposure to the virus. Of course, this raises questions of public support for vulnerable segments of the population for whom risk aversion will be quite rational. That would certainly be a more enlightened form of intervention than lockdowns, though support should be offered only to those highly at-risk individuals who can’t support themselves.
Christopher Phelan writes of three rationales for the lockdowns: buying time for development of a vaccine or treatments; reducing the number of infected individuals; and to avoid overwhelming the health care system. Phelan thinks all three are of questionable validity at this point. A vaccine might never arrive, and Phelan is pessimistic about treatments (I have more hope in that regard). Ultimately a large share of the population will be infected, lockdowns or not. And of course the health care system is not overwhelmed at this point. Yes, those caring for Covid patients are under a great stress, but the health care system as a whole, and patients with other maladies, are currently suffering from massive under-utilization.
If you wish to be socially distant, you are free to do so on your very own. Individuals are quite capable of voluntary risk mitigation without authoritarian fiat, as the charts above show. While private actors might not internalize all of the external costs of their activities, government is seldom capable of making the appropriate corrections. Coercion to enforce the kinds of crazy rules that have been imposed during this pandemic is the kind of abuse of power the nation’s founders intended to prevent. Reversing those orders can be difficult, and the precedent itself becomes a threat to future liberty. Nevertheless, we see mounting efforts to resist by those who are harmed by these orders, and by those who recognize the short-sighted nature of the orders. Private incentives for risk reduction, and private evaluation of the benefits of social and economic activity, offer superior governance to the draconian realities of lockdowns.
In advanced civilizations the period loosely called Alexandrian is usually associated with flexible morals, perfunctory religion, populist standards and cosmopolitan tastes, feminism, exotic cults, and the rapid turnover of high and low fads---in short, a falling away (which is all that decadence means) from the strictness of traditional rules, embodied in character and inforced from within. -- Jacques Barzun