Tags
All-Cause Mortality, Andrew Bostom, Andrew Cuomo, Cause of Death, Centers for Disease Control, Clinical Events, Coronavirus, Death Certificate, False Positives, Florida House of Representatives, Hospice Deaths, Justin Hart, Lockdown Deaths, Non-COVID Deaths. Co-Morbidities, PCR Tests, Specificity, Testing

The CDC changed its guidelines on completion of death certificates on April 5th of this year, and only for COVID-19 (C19), just as infections and presumed C19 deaths were ramping up. The substance of the change was to broaden the definition under which death should be attributed to C19. This ran counter to CDC guidelines followed over the previous 17 years, and the change not only makes the C19 death counts suspect: it also makes comparisons of C19 deaths to other causes of death unreliable, since only C19 is subject to the new CDC guidance. That’s true for concurrent and historical comparisons. The distortions are especially bad relative to other respiratory diseases, but also relative to other conditions that are common in mortality data.
The change in the CDC guidelines was noted in a recent report prepared for the Florida House of Representatives. It was brought to my attention by a retweet by Justin Hart linked to this piece on Andrew Bostom’s site. Death certificates are divided into two parts: Part 1 provides four lines in which causes of death are listed in reverse clinical order of events leading to death. Thus, the first line is the final clinical condition precipitating death. Prior clinical events are to be listed below that. The example shown above indicates that an auto accident, listed on the fourth line, initiated the sequence of events. Part 2 of the certificate is available for physicians or examiners to list contributing factors that might have played a role in the death that were not part of the sequence of clinical events leading to death.
The CDC’s change in guidelines for C19, and C19 only, made the criteria for inclusion in Part 1 less specific, and it essentially eliminated the distinction between Parts 1 and 2. The following appears under “Vital Records Criteria”:
“A death certificate that lists COVID-19 disease or SARS-CoV-2 as a cause of death or a significant condition contributing to death.”
How much difference does this make? For one thing, it opens the door to C19-attributed deaths in cases of false-positive PCR tests. When large cohorts are subject to testing — for example, all patients admitted to hospitals — there will always be a significant number of false positives even when test specificity is as high as 98 – 99%.
The elimination of any distinction between Parts 1 and 2 causes other distortions. A review of the Florida report is illustrative. The House staff reviewed almost 14,000 certificates for C19-19 attributed deaths. Over 9% of those did not list C19 among the clinical conditions leading to death. Instead, in those cases, C19 was listed as a contributing factor. Under the CDC’s previous guidelines, those would not have been counted as C19 deaths. The Florida House report is conservative in concluding that the new CDC guidelines inflated C19 deaths by only those 9% of the records examined.
There are reasons to think that the exaggeration was much greater, however. First, the Florida House report noted that nearly 60% of the certificates contained information “recorded in a manner inconsistent with state and national guidance”. In addition, almost another 10% of the fatalities were among patients already in hospice! Do we really believe the deaths of all those patients whose diseases had reached such an advanced stage should be classified as C19 fatalities? And another 1-2% listed non-C19 conditions as the immediate and underlying causes.
Finally, more than 20% of the certificates listed C19 alone as a cause of death despite a range of other contributing conditions or co-morbidities. This in itself may have been prompted by the change in the CDC’s guidelines, as the normal standards often involve a “comorbidity” as the initial reason for hospitalization — in that case a clinical event ordinarily listed in Part 1. The high rate of errors and the fact that roughly two-thirds of the deaths reviewed occurred in the hospital, where patients are all tested and often multiple times, raises the specter that up to 20% more of the C19 deaths were either erroneous and/or misclassified due to false positives.
(An exception may have occurred in New York, where an order issued in March by Governor Andrew Cuomo to return C19-positive residents of nursing homes (including suspected C19 cases) back to those homes, The order was made before the change in CDC guidelines and wasn’t rescinded until later in April. There is reason to believe that some of the C19 deaths among nursing home residents in New York were undercounted.)
All told, in the Florida data we have potential misclassification of deaths of 9% + 9% + 2% + 20% = 40%, or inflation relative to actual C19 deaths of up to 40%/60% = 67%! I strongly doubt it’s that high, but I would not consider a range of 25% – 50% exaggeration to be unreasonable.
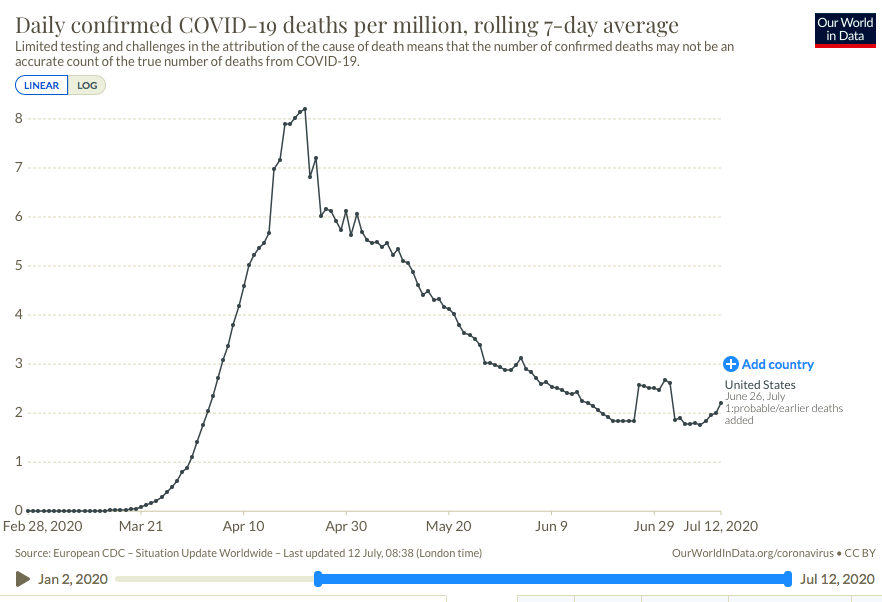
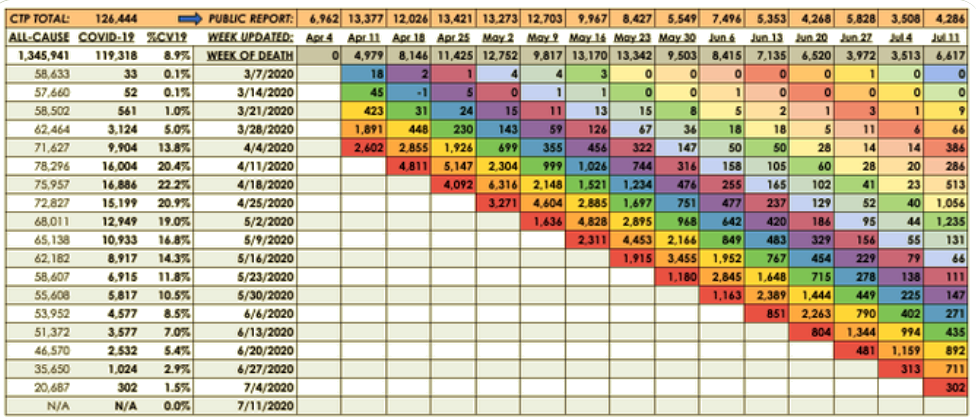
We know that reports of C19 deaths lag actual dates of death by anywhere from 1 to 8 weeks, sometimes even more. This is misleading when no effort is made to explain that difference, which I’ve never heard out of a single journalist. We also know that false positive tests inflate C19 deaths. The Florida report gives us a sense of how large that exaggeration might be. In addition, the Florida data show that the CDC guidelines inflate C19 deaths in other ways: as a mere contributing factor, it can now be listed as the cause of death, unlike the treatment of pneumonia as a contributing factor, for instance. The same kind of distortion occurs when patients contract C19 (or have a false positive test) while in hospice.
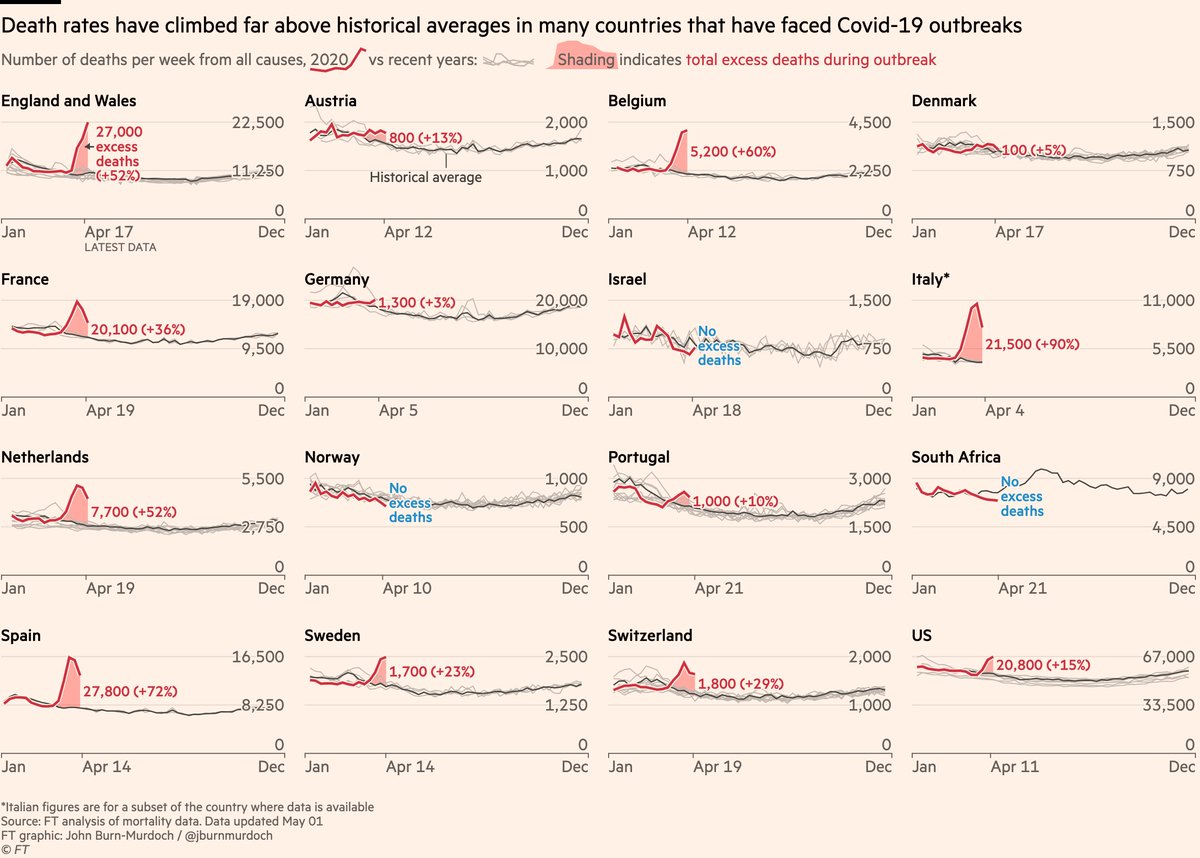
There is no doubt that C19 led to “excess deaths” relative to all-cause mortality. However, many of these fatalities are misclassified, and it’s likely that a large share were and are lockdown deaths as opposed to C19 deaths. That’s tragic. The CDC has done the country a massive disservice by creating “special rules” for attributing cause-of-death to C19. If reported C19 fatality rates reflected the same rules applied to other conditions, our approach to managing the pandemic surely would have inflicted far less damage to health and economic well being.