Tags
Coronavirus, Covid-19, Delta Variant, Ethical Skeptic, Gauteng Province, Immune Escape, Mutations, Omicron Variant, South Africa, Spanish Flu, Viral Interference, Vitamin D, World Health Organization, Xi Jinping, Xi Variant
The political motives behind the naming of the Covid Omicron variant might prove to be a huge irony. The Greek letter Xi was skipped by the World Health Organization (WHO), undoubtedly to avoid any symbolic association between Covid and the Chinese dictator Xi Jinping. After all, he’s probably determined to bury discussion of the leak at the Wuhan lab that was the probable cause of this whole mess. The WHO was happy to provide cover. The irony is that the Omicron variant might well bring on a more gentle phase of the pandemic if early indications can be trusted. But in that case, my guess is Chairman Xi wouldn’t have appreciated the twist even if WHO had called it the Xi variant.
The Omicron variant was identified in the Gauteng Province of South Africa and announced by national health authorities on November 24th. The earliest known sample was taken on November 9th. The variant was subsequently diagnosed in a number of other countries, including the U.S. It has a large number of mutations, and initial reports indicated that the variant was spreading extremely fast, having suddenly outcompeted other variants to account for the majority of new cases in South Africa. It is apparently highly contagious. Moreover, Omicron has been diagnosed among the vaccinated as well as those having immunity from prior infections, which is usually more effective and durable than vaccination. Thus, it is said to have “immune escape” properties. Scary indeed!
However, Omicron seems to have been around much longer than suggested by its initial diagnosis in late November (and see this link for an extreme view). Cases in a number of countries show that it is already global; the lags involved in diagnosis as well as earlier contacts with spreaders suggest that Omicron’s origin could have been as early as late September. That means the spread has not been quite as fast as the first alarming reports suggested.
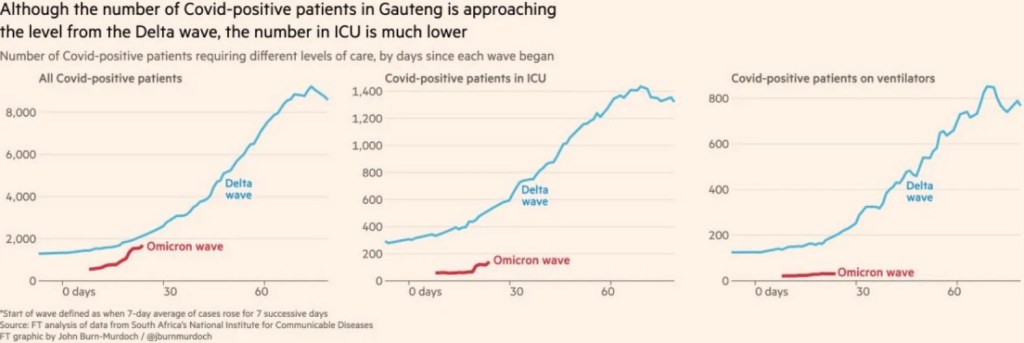
The reported symptoms of the Omicron variant have been quite mild, with fatigue being the most noteworthy. Omicron appears to have taken one mutation from the common cold, which, like Covid-19, is a type of coronavirus. And while there has been a surge in hospitalized cases in South Africa, most of these are said to be “incidental”. That is, these patients were admitted for other problems but happened to test positive for the Omicron variant. As we’ve seen throughout the pandemic, the data is not always reliable.
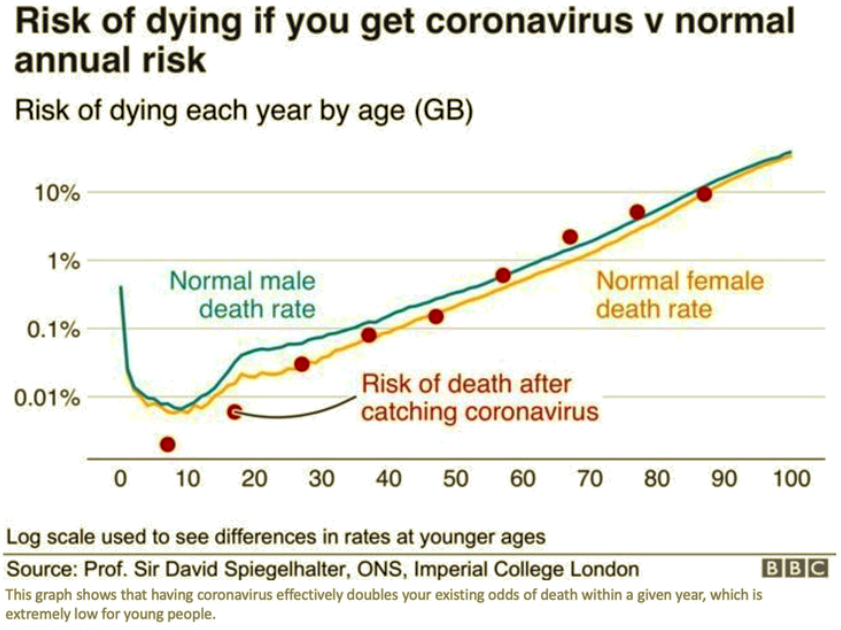
It’s too early to draw definite conclusions, and this variant might prove to be more dangerous with time. In fact, some say that South Africa’s experience might not be representative because of its young population and high natural immunity. It also happens to be early summer there, when higher vitamin D levels help to boost immunity. So, there is a great deal of uncertainty about Omicron (and see here). Nevertheless, I’ll risk a jinx by momentarily contemplating an outcome that’s not terribly far-fetched.
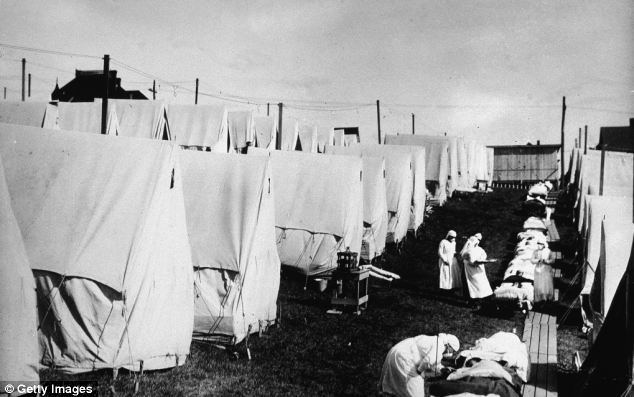
Viruses mutate in ways that help ensure their survival: they must not kill too many of their hosts, which means the usual progression is toward less lethal variants. They may become more contagious, and new variants must be contagious enough to outcompete their ancestors. Viral interference can sometimes prevent multiple viruses from having a broad coexistence. That’s the likely phenomenon we witnessed when the Covid pandemic coincided with the virtual disappearance of the flu and other respiratory viruses. More to the point, it’s the same phenomenon that occurred when the Spanish Flu was eventually outcompeted by less deadly variants.
So it’s possible that a mild Omicron will put the pandemic behind us. If it proves to be as contagious and as mild as it appears thus far, it would likely displace Delta and other variants as the first phase of a new, endemic malady. That might even cut into the severity of the current seasonal wave. The Ethical Skeptic tweets thusly:
“So was Omicron an ultra fast-mutating magic terminator variant? A gift from God, or aliens…? … Or natural virility/genetic profile derived from a previous variant conferring immunity …”
That would be a wonderful outcome, but Omicron’s arrival in the northern hemisphere just as winter gets underway contributes to the uncertainty. It’s severity during the northern winter could be far worse than what we’ve seen in South Africa. We can hope this variant isn’t one truly deserving of Chairman Xi’s name.