Tags
Antibody, Antigen, Carl T. Bergstrom, Christopher Moore, Covid-19, Herd Immunity, Heterogeneity, Household Infection, Immunity, Infection Mortality Risk, Initial Viral Load, John Cochrane, Lockdowns, Marc Lipsitch, Muge Cevik, Natalie Dean, Natural Immunity, Philippe Lemoine, R0, Santa Fe Institute, SARS-CoV-2, Social Distancing, Super-Spreaders, Zvi Mowshowitz
Immunity doesn’t mean you won’t catch the virus. It means you aren’t terribly susceptible to its effects if you do catch it. There is great variation in the population with respect to susceptibility. This simple point may help to sweep away confusion over the meaning of “herd immunity” and what share of the population must be infected to achieve it.
Philippe Lemoine discusses this point in his call for an “honest debate about herd immunity“. He reproduces the following chart, which appeared in this NY Times piece by Carl T. Bergstrom and Natalie Dean:
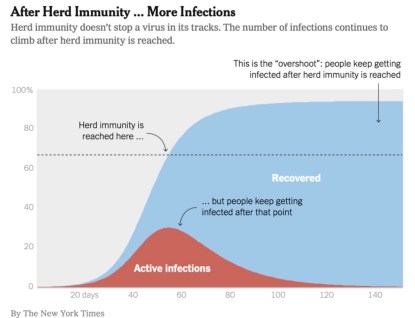
Herd immunity, as defined by Bergstrom and Dean, occurs when there are sufficiently few susceptible individuals remaining in the population to whom the actively-infected can pass the virus. The number of susceptible individuals shrinks over time as more individuals are infected. The chart indicates that new infections will continue after herd immunity is achieved, but the contagion recedes because fewer additional infections are possible.
We tend to think of the immune population as those having already been exposed to the virus, and who have recovered. Those individuals have antibodies specifically targeted at the antigens produced by the virus. But many others have a natural immunity. That is, their immune systems have a natural ability to adapt to the virus.
Heterogeneity
At any point in a pandemic, the uninfected population covers a spectrum of individuals ranging from the highly susceptible to the hardly and non-susceptible. Immunity, in that sense, is a matter of degree. The point is that the number of susceptible individuals doesn’t start at 100%, as most discussions of herd immunity imply, but something much smaller. If a relatively high share of the population has low susceptibility, the virus won’t have to infect such a large share of the population to achieve effective herd immunity.
The apparent differences in susceptibility across segments of the population may be the key to early herd immunity. We’ve known for a while that the elderly and those with pre-existing conditions are highly vulnerable. Otherwise, youth and good health are associated with low vulnerability.
Lemoine references a paper written by several epidemiologists showing that “variation in susceptibility” to Covid-19 “lowers the herd immunity threshold”:
“Although estimates vary, it is currently believed that herd immunity to SARS-CoV-2 requires 60-70% of the population to be immune. Here we show that variation in susceptibility or exposure to infection can reduce these estimates. Achieving accurate estimates of heterogeneity for SARS-CoV-2 is therefore of paramount importance in controlling the COVID-19 pandemic.”
The chart below is from that paper. It shows a measure of this variation on the horizontal axis. The colored, vertical lines show estimates of historical variation in susceptibility to historical viral episodes. The dashed line shows the required exposure for herd immunity as a function of this measure of heterogeneity.
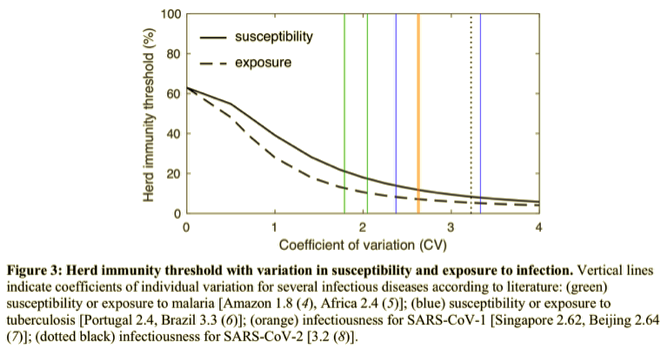
Their models show that under reasonable assumptions about heterogeneity, the reduction in the herd immunity threshold (in terms of the percent infected) may be dramatic, to perhaps less than 20%.
Then there are these tweets from Marc Lipsitch, who links to this study:
“As an illustration we show that if R0=2.5 in an age-structured community with mixing rates fitted to social activity studies, and also categorizing individuals into three categories: low active, average active and high active, and where preventive measures affect all mixing rates proportionally, then the disease-induced herd immunity level is hD=43% rather than hC=1−1/2.5=60%.”
Even the celebrated Dr. Bergstrom now admits, somewhat grudgingly, that hereogeniety reduces the herd immunity threshold, though he doesn’t think the difference is large enough to change the policy conversation. Lipsitch also is cautious about the implications.
Augmented Heterogeneity
Theoretically, social distancing reduces the herd immunity threshold. That’s because infected but “distanced” people are less likely to come into close contact with the susceptible. However, that holds only so long as distancing lasts. John Cochrane discusses this at length here. Social distancing compounds the mitigating effect of heterogeneity, reducing the infected share of the population required for herd immunity.
Another compounding effect on heterogeneity arises from the variability of initial viral load on infection (IVL), basically the amount of the virus transmitted to a new host. Zvi Mowshowitz discusses its potential importance and what it might imply about distancing, lockdowns, and the course of the pandemic. In any particular case, a weak IVL can turn into a severe infection and vice versa. In large numbers, however, IVL is likely to bear a positive relationship to severity. Mowshowitz explains that a low IVL can give one’s immune system a head start on the virus. Nursing home infections, taking place in enclosed, relatively cold and dry environments, are likely to involve heavy IVLs. In fact, so-called household infections tend to involve heavier IVLs than infections contracted outside of households. And, of course, you are very unlikely to catch Covid outdoors at all.
Further Discussion
How close are we to herd immunity? Perhaps much closer than we thought, but maybe not close enough to let down our guard. Almost 80% of the population is less than 60 years of age. However, according to this analysis, about 45% of the adult population (excluding nursing home residents) have any of six conditions indicating elevated risk of susceptibility to Covid-19 relative to young individuals with no co-morbidities. The absolute level of risk might not be “high” in many of those cases, but it is elevated. Again, children have extremely low susceptibility based on what we’ve seen so far.
This is supported by the transmission dynamics discussed in this Twitter thread by Dr. Muge Cevik. She concludes:
“In summary: While the infectious inoculum required for infection is unknown, these studies indicate that close & prolonged contact is required for #COVID19 transmission. The risk is highest in enclosed environments; household, long-term care facilities and public transport. …
Although limited, these studies so far indicate that susceptibility to infection increases with age (highest >60y) and growing evidence suggests children are less susceptible, are infrequently responsible for household transmission, are not the main drivers of this epidemic.”
Targeted isolation of the highly susceptible in nursing homes, as well as various forms of public “distancing aid” to the independent elderly or those with co-morbidities, is likely to achieve large reductions in the effective herd immunity ratio at low cost relative to general lockdowns.
The existence of so-called super-spreaders is another source of heterogeneity, and one that lends itself to targeting with limitations or cancellations of public events and large gatherings. What’s amazing about this is how the super-spreader phenomenon can lead to the combustion of large “hot spots” in infections even when the average reproduction rate of the virus is low (R0 < 1). This is nicely illustrated by Christopher Moore of the Santa Fe Institute. Super-spreading also implies, however, that while herd immunity signals a reduction in new infections and declines in the actively infected population, “hot spots” may continue to flare up in a seemingly random fashion. The consequences will depend on how susceptible individuals are protected, or on how they choose to mitigate risks themselves.
Conclusion
I’ve heard too many casual references to herd immunity requiring something like 70% of the population to be infected. It’s not that high. Many individuals already have a sort of natural immunity. Recognition of this heterogeneity has driven a shift in the emphasis of policy discussions to the idea of targeted lockdowns, rather than the kind of indiscriminate “dumb” lockdowns we’ve seen. The economic consequences of shifting from broad to targeted lockdowns would be massive. And why not? The health care system has loads of excess capacity, and Covid infection fatality risk (IFR) is turning out to be much lower than the early, naive estimates we were told to expect, which were based on confirmed case fatality rates (CFRs).