I see references to “long COVID” or “long-haul COVID” almost every day. No, it’s not an extended COVID infection or an extra scary version of COVID. It’s about lingering or new symptoms after recovery from the infection. Reportedly, these symptoms range from fatigue or anxiety to joint pain. Sometimes they are rather unusual afflictions such as “COVID toes”, described as rashes or red spots on toes. Sebastian Rushworth notes that there is “no hard evidence that long COVID is a distinct entity”. It was essentially invented on social media by groups of individuals who connected to discuss various post-COVID symptoms. Rushworth says:
“The most common symptoms in people with long covid (defined in the study as still having symptoms after four weeks) were fatigue (98%) and intermittent headache (91%). … symptoms of long covid are extremely unspecific, so it is probable that long covid is actually a whole bunch of different things, of which I would think post-viral syndrome is likely a significant part.”
Post-viral syndrome should not be a big surprise, since COVID is, well, a virus! PVS can last for months and commonly has the following symptoms:
Those sound familiar. PVS symptoms are thought to be a consequence of the body’s effort to fight off a virus, including the lingering effects of a strong immune response and the inflammation it can induce. Such an immune response can lead to even greater problems for those with a genetic predisposition for autoimmune diseases like diabetes. It happens. But none of this is new or unique to COVID.
While PVS and autoimmune diseases are very real, the unbridled panic over COVID has led to a few false claims. “COVID toes” is one of them. Moreover, the pandemic precipitated an avalanche of poor-quality academic research, rushed in an effort to produce useful findings. Some of that research is implicated in the COVID myths we’ve heard. An example discussed at the last link is the incidence of heart inflammation or myocarditis in COVID patients. This was all over the media in the months leading up to the college football season, as young athletes were said to be vulnerable. In fact, it’s incidence among COVID patients is fairly rare, and it’s not unique to COVID.
COVID can be a nasty infection, primarily for the aged and those with pre-existing conditions, including obesity. PVS is an unfortunate reality for many patients. But “long-COViD” is merely a varied collection of post-viral symptoms. Many of them are vague and usually self-diagnosed. Long COVID is, as Rushworth says, “basically whatever the person who thinks they have it says it is.” That the media has promoted long COVID and its varied manifestations as something wholly new, including a few probable “imagifestations” (to coin a term), is one more example of the “panic porn” to which we’ve been subjected during the pandemic.
Here’s one of the many entertaining videos made by people who want to convince you that hospitals are overrun with COVID patients (and here is another, and here, here, and here). That assertion has been made repeatedly since early in the pandemic, but as I’ve made clear on at least two occasions, the overall system has plenty of capacity. There are certainly a few hospitals at or very near capacity, but diverting patients is a long-standing practice, and other hospitals have spare capacity to handle those patients in every state. Those with short memories would do well to remember 2018 before claiming that this winter is unique in terms of available hospital beds.
An old friend with long experience as a hospital administrator claimed that I didn’t account for staffing shortfalls in my earlier posts on this topic, but in fact the statistics I presented were all based on staffed inpatient or ICU beds. Apparently, he didn’t read those posts too carefully. Moreover, it’s curious that a hospital administrator would complain so bitterly of staffing shortfalls in the wake of widespread hospital layoffs in the spring. And it’s curious that so many layoffs would accompany huge bailouts of hospital systems by the federal government, courtesy of the CARES Act.
In fairness, hospitals suffered huge declines in revenue in the spring of 2020 as elective procedures were cancelled and non-COVID patients stayed away in droves. Then hospitals faced the expense of covering their shortfalls in PPE. We know staffing was undercut when health care workers were diagnosed with COVID, but in an effort to stem the red ink, hospitals began laying-off staff anyway just as the the COVID crisis peaked in the spring. About 160,000 staffers were laid off in April and May, though more than half of those losses had been recovered as of December.
Did these layoffs lead to a noticeable shortfall in hospital capacity? It’s hard to say because bed capacity is a squishy metric. When patients are discharged, staffed beds can ratchet down because beds might be taken “off-line”. When patients are admitted, beds can be brought back on-line. ICU capacity is flexible as well, as parts of other units can be quickly modified for patients requiring intensive care. And patient ratios can be adjusted to accommodate layoffs or an influx of admissions. Since early in the fall, occupancy has been overstated for several reasons, including a new requirement that beds in use for observation of outpatients with COVID symptoms for 8 hours or more must be reported as beds occupied. However, there are hospitals claiming that COVID is stressing capacity limits, but nary a mention of the earlier layoffs.
So where are we now in terms of staffed hospital occupancy. The screen shot below is from the HHS website and represents staffed bed utilization nationwide. 29% of capacity is open, hardly a seasonal anomaly, and there are very few influenza admissions thus far this winter, which is rather unique. 37% of ICU beds are available, and COVID patients, those admitted either “for” or “with” COVID, account for less than 18% of inpatients, though again, that includes observational beds.
Next are the 25 states with the highest inpatient bed utilization as of January 7th. Rhode Island tops the list at just over 90%, and eight other states are over 80%. In terms of ICU utilization, Georgia and Alabama are very tight. California and Arizona are outliers with respect to proportions of COVID inpatients, 41% and 38%, respectively. Finally, CA, GA, AL and AZ are all near or above 50% of ICU beds occupied by COVID patients.
So some of the states reaching the peak of their fall waves are pretty tight, and there are states with large numbers of very serious cases. Nevertheless, in all states there is variation across local hospitals to serve in relief, and it is not unusual for hospitals to suffer wintertime strains on capacity.
Los Angeles County is receiving much attention for recent COViD stress placed on hospital capacity. But it is hard to square that narrative with certain statistics. For example, Don Wolt notes that the state of California reports available ICU capacity in Southern CA of zero, but LA County has reported 10% ~ 11% for weeks. And the following chart shows that LA County occupancy remains well below it’s July peak, especially after a recent downward revision from the higher level shown by the blue dashed line.
Interestingly, the friend I mentioned said I should talk with some health system CEOs about recent occupancies. He overlooked the fact that I quoted or linked to comments from some system CEOs in my earlier posts (linked above). It’s noteworthy that one of those CEOs, and this report from the KPI Institute, propose that an occupancy rate of 85% is optimal. This medical director prefers a 75% – 85% rate, depending on day of week. These authors write that there is no one “optimal” occupancy rate, but they seem to lean toward rates below 85%. This paper reports a literature search indicating ICU occupancy of 70% -75% is optimal, while noting a variety of conditions may dictate otherwise. Seasonal effects on occupancy are of course very important. In general, we can conclude that hospital utilization in most states is well within acceptable if not “optimal” levels, especially in the context of normal seasonal conditions. However, there are a few states in which some hospitals are facing tight capacity, both in total staffed beds and in their ICUs.
None of this is to minimize the challenges faced by administrators in managing hospital resources. No real crisis in hospital capacity exists currently, though hospital finances are certainly under stress. Yes, hospitals collect greater reimbursements on COVID patients via the CARES Act, but COVID patients carry high costs of care. Also, hospitals have faced steep declines in revenue from the fall-off in other care, high costs in terms of PPE, specialized equipment and medications, and probably high temporary staffing costs in light of earlier layoffs and short-term losses of staff to COVID infections. The obvious salve for many of these difficulties is cash, and the most promising source is public funding. So it’s unsurprising that executives are inclined to cry wolf about a capacity crisis. It’s a simple story and more appealing than pleading for cash, and it’s a scare story that media are eager to push.
Both the Pfizer and the Moderna COVID vaccines require two doses, with an effectiveness of about 95%. But a single dose may have an efficacy of about 80% that is likely to last over a number of weeks without a second dose. There are varying estimates of short-term efficacy, and but see here, here, and here. The chart above is for the Pfizer vaccine (red line) relative to a control group over days since the first dose, and the efficacy grows over time relative to the control before a presumed decay ever sets in.
Unfortunately, doses are in short supply, and getting doses administered has proven to be much more difficult than expected. “First Doses First” (FDF) is a name for a vaccination strategy focusing on delivering only first doses until a sufficient number of the highly vulnerable receive one. After that, second doses can be administered, perhaps within some maximum time internal such as 8 – 12 weeks. FDF doubles the number of individuals who can be vaccinated in the short-term with a given supply of vaccine. Today, Phil Kerpen posted this update on doses delivered and administered thus far:
Dosing has caught up a little, but it’s still lagging way behind deliveries.
As Alex Tabbarok points out, FDF is superior strategy because every two doses create an average of 1.6 immune individuals (2 x 0.8) instead of just 0.95 immune individuals. His example involves a population of 300 million, a required herd immunity level of two-thirds (higher than a herd immunity threshold), and an ability to administer 100 million doses per month. Under a FDF regime, you’ve reached Tabarrok’s “herd immunity” level in two months. (This is not to imply that vaccination is the only contributor to herd immunity… far from it!) Under the two-dose regime, you only get halfway there in that time. So FDF means fewer cases, fewer deaths, shorter suspensions of individual liberty, and a faster economic recovery.
An alternative that doubles the number of doses available is Moderna’s half-dose plan. Apparently, their tests indicate that half doses are just as effective as full doses, and they are said to be in discussions with the FDA and Operation Warp Speed to implement the half-dose plan. But the disadvantage of the half-dose plan relative to FDF is that the former does not help to overcome the slow speed with which doses are being administered.
Vaccine supplies are bound to increase dramatically in coming months, and the process of dosing will no doubt accelerate as well. However, for the next month or two, FDF is too sensible to ignore. While I am not a fan of all British COVID policies, their vaccination authorities have recommended an FDF approach as well as allowing different vaccines for first and second doses.
Anthony Fauci has repeatedly increased his estimate of how much of the population must be vaccinated to achieve what he calls herd immunity, and he did it again in late December. This series of changes, and other mixed messages he’s delivered in the past, reveal Fauci to be a “public servant” who feels no obligation to level with the public. Instead, he crafts messages based on what he believes the public will accept, or on his sense of how the public must be manipulated. For example, by his own admission, his estimates of herd immunity have been sensitive to polling data! He reasoned that if more people reported a willingness to take a vaccine, he’d have flexibility to increase his “public” estimate of the percentage that must be vaccinated for herd immunity. Even worse, Fauci appears to lack a solid understanding of the very concept of herd immunity.
Manipulation
There is so much wrong with his reasoning on this point that it’s hard to know where to start. In the first place, why in the world would anyone think that if more people willingly vaccinate it would imply that even more must vaccinate? And if he felt that way all along it demonstrates an earlier willingness to be dishonest with the public. Of course, there was nothing scientific about it: the series of estimates was purely manipulative. It’s almost painful to consider the sort of public servant who’d engage in such mental machinations.
Immunity Is Multi-Faceted
Second, Fauci seemingly wants to convince us that herd immunity is solely dependent on vaccination. Far from it, and I’m sure he knows that, so perhaps this too was manipulative. Fauci intimates that COVID herd immunity must look something like herd immunity to the measles, which is laughable. Measles is a viral infection primarily in children, among whom there is little if any pre-immunity. The measles vaccine (MMR) is administered to young children along with occasional boosters for some individuals. Believe it or not, Fauci claims that he rationalized a requirement of 85% vaccination for COVID by discounting a 90% requirement for the measles! Really???
In fact, there is substantial acquired pre-immunity to COVID. A meaningful share of the population has long-memory, cross-reactive T-cells from earlier exposure to coronaviruses such as the common cold. Estimates range from 10% to as much as 50%. So if we stick with Fauci’s 85% herd immunity “guesstimate”, 25% pre-immunity implies that vaccinating only 60% of the population would get us to Fauci’s herd immunity goal. (Two qualifications: 1) the vaccines aren’t 100% effective, so it would take more than 60% vaccinated to offset the failure rate; 2) the pre-immune might not be identifiable at low cost, so there might be significant overlap between the pre-immune and those vaccinated.)
Conceptual Confusion
Vaccinations approaching 85% would be an extremely ambitious goal, especially if it is recommended annually or semi-annually. It would be virtually impossible without coercion. While more than 91% of children are vaccinated for measles in the U.S., it is not annual. Thus, measles does not offer an appropriate model for thinking about herd immunity to COVID. Less than half of adults get a flu shot each year, and somewhat more children.
Fauci’s reference to 85% – 90% total immunity is different from the concept of the herd immunity threshold (HIT) in standard epidemiological models. The HIT, often placed in the range of 60% – 70%, is the point at which new infections begin to decline. More infections occur above the HIT but at a diminishing rate. In the end, the total share of individuals who become immune due to exposure, pre-immunity or vaccination will be greater than the HIT. The point is, however, that reaching the HIT is a sufficient condition for cases to taper and an end to a contagion. If we use 65% as the HIT and pre-immunity of 25%, only 40% must be vaccinated to reach the HIT.
Heterogeneity
A recent innovation in epidemiological models is the recognition that there are tremendous differences between individuals in terms of transmissibility, pre-immunity, and other factors that influence the spread of a particular virus, including social and business arrangements. This kind of heterogeneity tends to reduce the effective HIT. We’ve already discussed the effect of pre-immunity. Suppose that certain individuals are much more likely to transmit the virus than others, like so-called super-spreaders. They spur the initial exponential growth of a contagion, but there are only so many of them. Once infected, no one else among the still-susceptible can spread the virus with the same force.
Researchers at the Max Planck Institute (and a number of others) have gauged the effect of introducing heterogeneity to standard epidemiological models. It is dramatic, as the following chart shows. The curves simulate a pandemic under different assumptions about the degree of heterogeneity. The peak of these curves correspond to the HIT under each assumption (R0 refers to the initial reproduction number from infected individuals to others).
Moderate heterogeneity implies a HIT of only 37%. Given pre-immunity of 25%, only an additional 12% of the population would have to be infected or vaccinated to prevent a contagion from gaining a foothold for the initial exponential stage of growth. Fauci’s herd immunity figure obviously fails to consider the effect of heterogeneity.
How Close To the HIT?
We’re not as far from HITs as Fauci might think, and a vaccination goal of 85% is absurd and unnecessary. The seasonal COVID waves we’ve experienced thus far have faded over a period of 10-12 weeks. Estimates of seroprevalence in many localities reached a range of 15% – 25% after those episodes, which probably includes some share of those with pre-immunity. To reach the likely range of a HIT, either some additional pre-immunity must have existed or the degree of heterogeneity must have been large in these populations.
But if that’s true, why did secondary waves occur in the fall? There are a few possibilities. Of course, some areas like the upper Midwest did not experience the springtime wave. But in areas that suffered a recurrance, perhaps the antibodies acquired from infections did not remain active for as long as six months. However, other immune cells have longer memories, and re-infections have been fairly rare. Another possibility is that those having some level of pre-immunity were still able to pass live virus along to new hosts. But this vector of transmission would probably have been quite limited. Pre-immunity almost surely varies from region to region, so some areas were not as firmly above their HITs as others. It’s also possible that infections from super-spreaders were concentrated within subsets of the population even within a given region, in certain neighborhoods or among some, but not all, social or business circles. Therefore, some subsets or “sub-herds” achieved a HIT in the first wave, but it was unnecessary for other groups. In other words, sub-herds spared in the first wave might have suffered a contagion in a subsequent wave. And again, reinfections seem to have been rare. Finally, there is the possibility of a reset in the HIT in the presence of a new, more transmissible variant of the virus, as has become prevalent in the UK, but that was not the case in the fall.
Fragility
Tyler Cowen has mentioned another possible explanation: so-called “fragile” herd immunity. The idea is that any particular HIT is dependent on the structure of social relations. When social distancing is widely practiced, for example, the HIT will be lower. But if, after a contagion recedes, social distancing is relaxed, it’s possible that the HIT will take a higher value at the onset of the next seasonal wave. Perhaps this played a role in the resurgence in infections in the fall, but the HIT can be reduced via voluntary distancing. Eventually, acquired immunity and vaccinations will achieve a HIT under which distancing should be unnecessary, and heterogeneity suggests that shouldn’t be far out of reach.
Conclusion
Anthony Fauci has too often changed his public pronouncements on critical issues related to management of the COVID pandemic. Last February he said cruises were fine for the healthy and that most people should live their lives normally. Oops! Then came his opinion on the limited effectiveness of masks, then a shift to their necessity. His first position on masks has been called a “noble lie” intended to preserve supplies for health care workers. However, Fauci was probably repeating the standing consensus at that point (and still the truth) that masks are of limited value in containing airborne pathogens.
This time, Fauci admitted to changing his estimate of “herd immunity” in response to public opinion, a pathetic approach to matters of public health. What he called herd immunity was really an opinion about adequate levels of vaccination. Furthermore, he neglected to consider other forms of immunity: pre-existing and already acquired. He did not distinguish between total immunity and the herd immunity threshold that should guide any discussion of pandemic management. He also neglected the significant advances in epidemiological modeling that recognize the reality of heterogeneity in reducing the herd immunity threshold. The upshot is that far fewer vaccinations are needed to contain future waves of the pandemic than Fauci suggests.
There are currently two vaccines in limited distribution across the U.S. from Pfizer and Moderna, but the number and variety of different vaccines will grow as we move through the winter. For now, the vaccine is in short supply, but that’s even more a matter of administering doses in a timely way as it is the quantity on hand. There are competing theories about how best to allocate the available doses, which is the subject of this post. I won’t debate the merits of refusing to take a vaccine except to say that I support anyone’s right to refuse it without coercion by public authorities. I also note that certain forms of discrimination on that basis are not necessarily unreasonable.
The vaccines in play all seem to be highly effective (> 90%, which is incredible by existing standards). There have been a few reports of side effects — certainly not in large numbers — but it remains to be seen whether the vaccines will have any long-term side effects. I’m optimistic, but I won’t dismiss the possibility.
Despite competing doctrines about how the available supplies of vaccine should be allocated, there is widespread acceptance that health care workers should go first. I have some reservations about this because, like Emma Woodhouse, I believe staff and residents at long-term care facilities should have at least equal priority. Yet they do not in the City of Chicago and probably in other areas. I have to wonder whether unionized health care workers there are the beneficiaries of political favoritism.
Beyond that question, we have the following competing priorities: 1) the vulnerable in care homes and other elderly individuals (75+, while younger individuals with co-morbidities come later); 2) “essential” workers of all ages (from police to grocery store clerks — decidedly arbitrary); and 3) basically the same as #2 with priority given to groups who have suffered historical inequities.
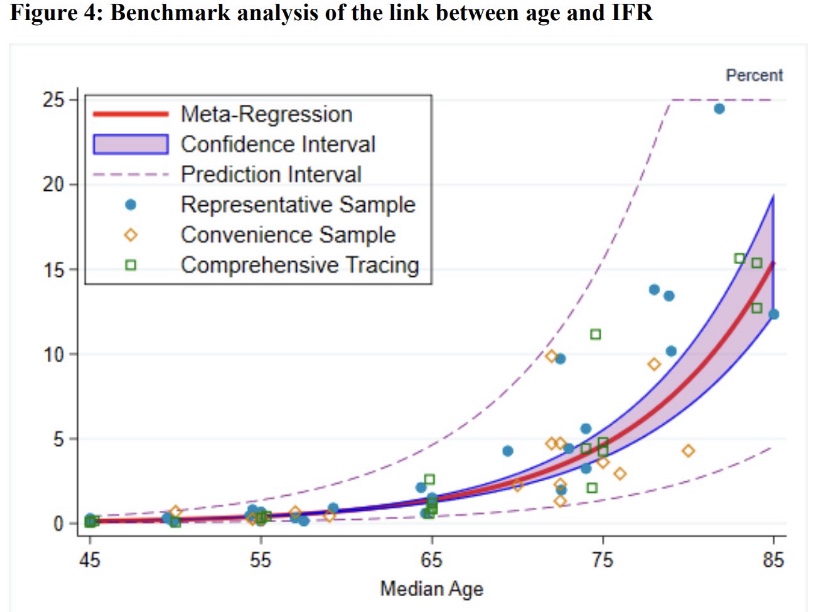
#1 is clearly the way to save the most lives, at least in the short-run. Over 40% of the deaths in the U.S. have been in elder-care settings, and COVID infection fatality ratesmount exponentially with age:
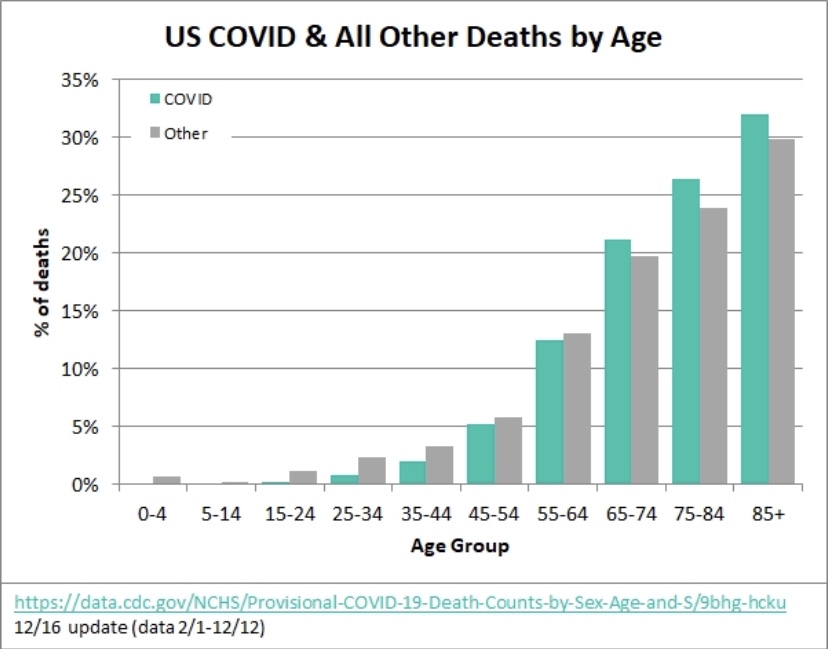
To derive the implications of #1 and #2, it’s more convenient to look at the share of deaths within each age cohort, since it incorporates the differences in infection rates and fatality rates across age groups (the number of “other” deaths is much larger than COVID deaths, of course, despite similar death shares):
The 75+ age group has accounted for about 58% of all COVID deaths in the U.S., and ages 25 – 64 accounted for about 20% (an approximate age range for essential workers). This implies that nearly three times as many lives can be saved by prioritizing the elderly, at least if deaths among so-called essential workers mimic deaths in the 25 – 64 age cohorts. However, the gap would be smaller and perhaps reversed in terms of life-years saved.
Furthermore, this is a short-run calculation. Over a longer time frame, if essential workers are responsible for more transmission across all ages than the elderly, then it might throw the advantage to prioritizing essential workers over the elderly, but it would take a number of transmission cycles for the differential to play out. Yes, essential workers are more likely to be “super-spreaders” than work-at-home, corporate employees, or even the unemployed, but identifying true super-spreaders would require considerable luck. Moreover, care homes generally house a substantial number of elderly individuals and staff in a confined environment, where spread is likely to be rampant. So the transmission argument for #2 over #1 is questionable.
The over-riding problem is that of available supply. Suppose enough vaccine is available for all elderly individuals within a particular time frame. That’s about 6.6% of the total U.S. population. The same supply would cover only about 13% of the younger age group identified above. Essential workers are a subset of that group, but the same supply would fall far short of vaccinating all of them; lives saved under #2 would then fall far short of the lives saved under #1. Quantities of the vaccine are likely to increase over the course of a few months, but limited supplies at the outset force us to focus the allocation decision on the short-term, making #1 the clear winner.
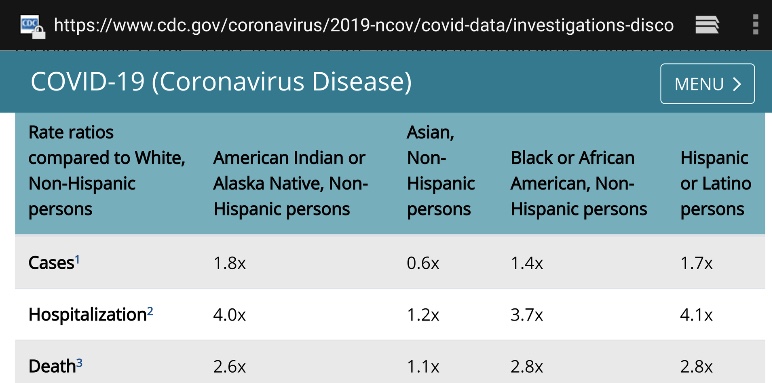
Now let’s talk about #3, minority populations, historical inequities, and the logic of allocating vaccine on that basis. Minority populations have suffered disproportionately from COVID, so this is really a matter of objective risk, not historical inequities… unless the idea is to treat vaccine allocations as a form of reparation. Don’t laugh — that might not be far from the intent, and it won’t count as a credit toward the next demand for “justice”.
For the sake of argument, let’s assume that minorities have 3x the fatality rate of whites from COVID (a little high). Roughly 40% of the U.S. population is non-white or Hispanic. That’s more than six times the size of the full 75+ population. If all of the available doses were delivered to essential workers in that group, it would cover less than half of them and save perhaps 30% of minority COVID deaths over a few months. In contrast, minorities might account for up to two-thirds of the deaths among the elderly. Therefore, vaccinating all of the elderly would save 58% of elderly COVID deaths and about 39% of minority deaths overall!
The COVID mortality risk to the average white individual in the elderly population is far greater than that faced by the average minority individual in the working age population. Therefore, no part of #3 is sensible from a purely mathematical perspective. Race/ethnicity overlaps significantly with various co-morbiditiesand the number of co-morbidities with which individuals are afflicted. Further analysis might reveal whether there is more to be gained by prioritizing by co-morbidities rather than race/ethnicity.
Megan McArdle has an interesting column on the CDC’s vaccination guidelines issued in November, which emphasized equity, like #3 above. But the CDC walked back that decision in December. The initial November decision was merely the latest of the the agency’s fumbles on COVID policy. In her column, McArdle notes that the public has understood that the priority was to save lives since the very start of the pandemic. Ideally, if objective measures show that identifiable characteristics are associated with greater vulnerability, then those should be considered in prioritizing individuals who desire vaccinations. This includes age, co-morbidities, race/ethnicity, and elements of occupational risk. But lesser associations with risk should not take precedence over greater associations with risk unless an advantage can be demonstrated in terms of lives saved, historical inequities or otherwise.
The priorities for the early rounds of vaccinationsmay differ by state or jurisdiction, but they are all heavily influenced by the CDC’s guidelines. Some states pay lip service to equity considerations (if they simply said race/ethnicity, they’d be forced to operationalize it), while others might actually prioritize doses by race/ethnicity to some degree. Once the initial phase of vaccinations is complete, there are likely to be more granular prioritizations based on different co-morbidities, for example, as well as race/ethnicity. Thankfully, the most severe risk gradient, advanced age, will have been addressed by then.
One last point: the Pfizer and Moderna vaccines both require two doses. Alex Tabarrok points out that first doses appear to be highly effective on their own. In his opinion, while supplies are short, the second dose should be delayed until all groups at substantially elevated risk can be vaccinated…. doubling the supply of initial doses! The idea has merit, but it is unlikely to receive much consideration in the U.S. except to the extent that supply chain problems make it unavoidable, and they might.
For clarity, start with this charming interpretive one-act on public health policy in 2020. You might find it a little sardonic, but that’s the point. It was one of the more entertaining tweets of the day, from @boriquagato.
A growing body of research shows that stringent non-pharmaceutical interventions (NPIs) — “lockdowns” is an often-used shorthand — are not effective in stemming the transmission and spread of COVID-19. A compendium of articles and preprints on the topic was just published by the American Institute for Economic Research (AEIR): “Lockdowns Do Not Control the Coronavirus: The Evidence”. The list was compiled originally by Ivor Cummins, and he has added a few more articles and other relevant materials to the list. The links span research on lockdowns across the globe. It covers transmission, mortality, and other health outcomes, as well as the economic effects of lockdowns. AIER states the following:
“Perhaps this is a shocking revelation, given that universal social and economic controls are becoming the new orthodoxy. In a saner world, the burden of proof really should belong to the lockdowners, since it is they who overthrew 100 years of public-health wisdom and replaced it with an untested, top-down imposition on freedom and human rights. They never accepted that burden. They took it as axiomatic that a virus could be intimidated and frightened by credentials, edicts, speeches, and masked gendarmes.
The pro-lockdown evidence is shockingly thin, and based largely on comparing real-world outcomes against dire computer-generated forecasts derived from empirically untested models, and then merely positing that stringencies and “nonpharmaceutical interventions” account for the difference between the fictionalized vs. the real outcome. The anti-lockdown studies, on the other hand, are evidence-based, robust, and thorough, grappling with the data we have (with all its flaws) and looking at the results in light of controls on the population.”
We are constantly told that public intervention constitutes “leadership”, as if our well being depends upon behavioral control by the state. Unfortunately, it’s all too typical of research on phenomena deemed ripe for intervention that computer models are employed to “prove” the case. A common practice is to calibrate such models so that the outputs mimic certain historical outcomes. Unfortunately, a wide range of model specifications can be compatible with an historical record. This practice is also a far cry from empirically testing well-defined hypotheses against alternatives. And it is a practice that usually does poorly when the model is tested outside the period to which it is calibrated. Yet that is the kind of evidence that proponents of intervention are fond of using to support their policy prescriptions.
In this case, it’s even worse, with some of the alleged positive effects of NPI’s wholly made-up, with no empirical support whatsoever! So-called public health experts have misled themselves, and the public, with this kind of fake evidence, when they aren’t too busy talking out of both sides of their mouths.
Now why would I say such a thing? Well, 1) the presidential election was rife with fraud, as many of us feared would be the case (and see here); 2) the supposed winner, Joe “The Plagiarist” Biden, is a figurehead, and he will remain in the White House only as long as he toes the line set down by the Left; and 3) the figurehead is badly compromised by Chinese and other foreign influence: Chairman Xi Jinping of the Chinese Communist Party (CCP) is undoubtedly pleased that such a pliant American president will be taking office.
Those who deny the fraud that took place in the election keep insisting “there’s no evidence!” In fact, there is ample evidence to convince any fair-minded person that massive fraud took place across a number of states (see here, here, here and here). We knew that massive adoption of mail-in ballots was an invitation to fraud. There are many hundreds of affidavits (yes, they constitute evidence) stating that Republican election officials and poll watchers were obstructed in their attempts to observe the counting process on and after Election Day, and worse. There is video evidence of activities coincident with late-night lockouts of Republican poll watchers and outrageous, instant jumps in Biden’s vote totals. There is definitive evidence of process “shortcuts” in several states that led to a large number of unverified ballots. These shortcuts were often taken in contravention of state law. There were failed chains of custody for thousands of ballots across several states. There were dead and out-of-state voters. There were irregularities associated with vote tabulations by Dominion machines. There are hand recounts in a few counties that demonstrate miscounting of ballots. And of course, there was a willful effort to suppress this information by the news media, and outright censorship of this information by social media platforms.
No matter what has or will happen in the courts, state legislatures, or Congress, a large share of the voting public believes there was fraud in this election. In fact, a significant share of democrats believe the election was stolen from President Trump! The fraud goes beyond the electoral process as well. Polls show a substantial number of Biden voters would not have voted for him had they known about the escapades of Hunter Biden and Joe’s role as the family cash cow. The mainstream media and social media platforms also deliberately suppressed the information about Hunter Biden’s pay-for-play scandal prior to the election. And that came after months of avoiding any real scrutiny of Biden’s policy agenda and his fitness as a candidate. Instead, the media asked Joe tough questions about his favorite ice cream.
Not your president? The Hunter Biden saga creates doubt about who Joe Biden is likely to serve as President. To whom is Joe beholden for “taking care” of “the big guy’s” family? How about Hunter’s deals in the Ukraine and Russia? How heavily was the CCP involved in Hunter’s business ventures? How much is Joe compromised by these unfortunate ties? What kind of compromises might it be worth to Joe to avoid further exposure? Should the Biden Administration overlook the plight of the Uhygers? Turn the cheek on Hong Kong? Sacrifice Taiwan? Allow Chinese technology to be embedded in U.S. communications hardware? Cede international rights in the South China Sea? Perhaps Joe will be Chairman Xi’s President. And perhaps others hold cards, such as the hostile Iranian regime. Not our president.
Finally, if you *think* you voted for Joe as president, be aware that he is, even now, a doddering figurehead, a puppet of the Left whose strings might well be clipped when he demonstrates even a hint of incapacity. It might not be long. Perhaps the Left will adopt Hunter’s imbroglio as an excuse to take Joe down. It seems more than a little suspicious that the media, post-election, has finally begun to talk about Hunter’s miscues and Joe’s “possible” involvement.
But even if Joe remains in the Oval Office through a first term, just who will be in charge? Joe? No, he is captive to the interests that helped put him there. We might just as well call him “Any-Way-the-Wind-Blows Joe”. Angela Davis, former VP of the Communist Party USA, said during the primaries that she supported Biden because he:
“… can be most effectively pressured into allowing more space for the evolving anti-racist movement.”
Well, Joe better not compromise with anyone or accept any policy that Angela Davis deems “racist”.
Let’s consider a few influences expected to be paramount in pulling Joe’s strings: Barack Obama, Alexandria Ocasio-Cortez, Julian Castro, and Black Lives Matter. Bernie Sanders will also loom large, and of course Kamala Harris will be there to push the leftist agenda, and she’ll be waiting in the wings when Joe loses his tentative grip on the reins of the progressive machine. Joe better not resist these forces: he can be manipulated, and if he strays from the path, he and his presidency can be cancelled.
If you are a member of the Marxist wing of the coalition, you might have him just where you want him. If you are a member of the CCP, then he might be your president. But he is not the president of the disenfranchised voters whose majority was outstripped by the mailed ballot fraud. And if you are a centrist Democrat, you should awaken to the reality of the hard-left movement with which you’ve joined forces. Do not accept it as a legitimate governing force. No, Joe Biden will not be your president.
As I’ve noted in the past, apologists willing to look past Joe Biden’s domestic and foreign controllers and the fraudulent election are not to be trusted. Indeed, they have been willing to look past Biden’s personal status as a fraud, from his many lies about his family to his admitted plagiarism, to his denial of sexual aggression toward female staffers. In summary, I can’t put it any better than Newt Gingrich does here:
“… I have no interest in legitimizing the father of a son who Chinese Communist Party members boast about buying. Nor do I have any interest in pretending that the current result is legitimate or honorable. It is simply the final stroke of a four-year establishment-media power grab. It has been perpetrated by people who have broken the law, cheated the country of information, and smeared those of us who believe in America over China, history over revisionism, and the liberal ideal of free expression over cancel culture.”
Here’s some incredible data on PCR tests demonstrating a radically excessive lab practice that generates false positives. I’m almost tempted to say we’d do just as well using a thermometer and the coffee ground test. Open a coffee tin and take a sniff. Can you smell the distinct aroma of the grounds? If not, and if you have other common symptoms, there’s a decent chance you have an active COVID infection. That test is actually in use in some parts of the globe!
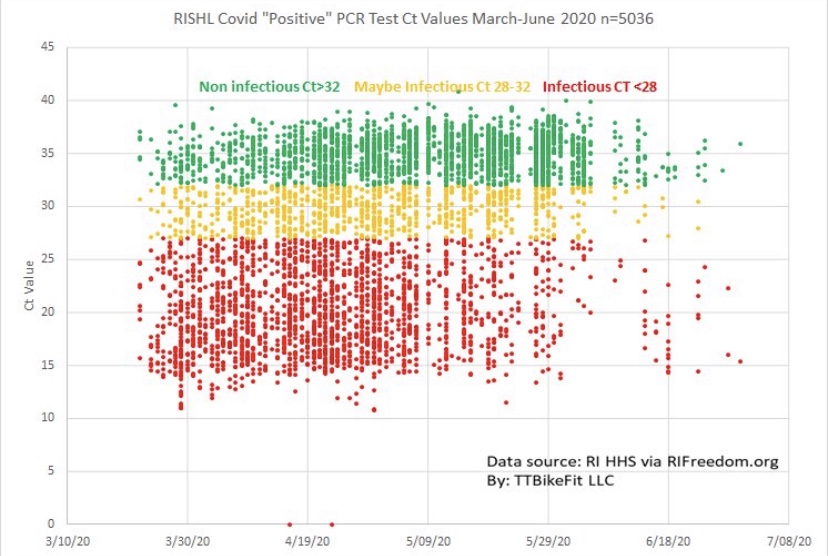
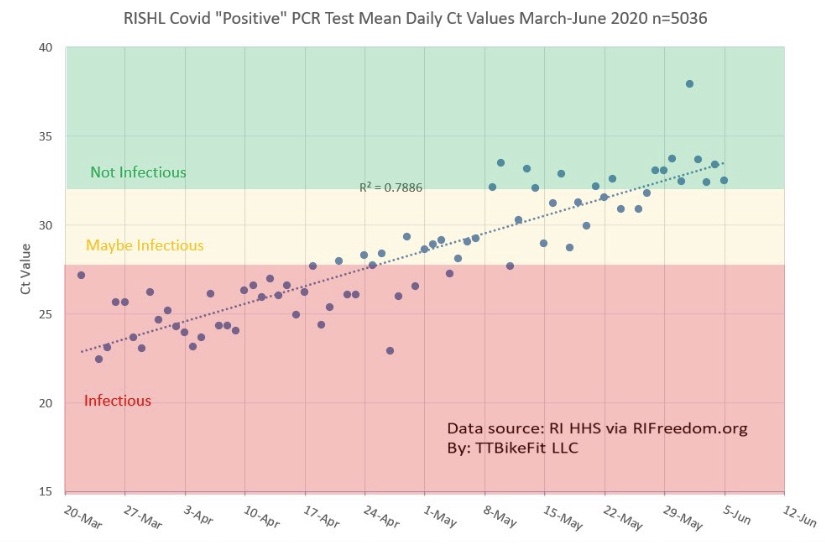
The data shown below on PCR tests are from the Rhode Island Department of a Health and the Rhode Island State Health Lab. They summarize over 5,000 positive COVID PCR tests (collected via deep nasal swabs) taken from late March through early July. The vertical axis in the chart measures the cycle threshold (Ct) value of each positive test. Ct is the number of times the RNA in a sample must be replicated before any COVID-19 (or COVID-like) RNA is detected. It might be from a live virus or perhaps a fragment of a dead virus. A positive test with a low Ct value indicates that the subject is likely infected with billions of live COVID-19 viruses, while a high Ct value indicates perhaps a handful or no live virus at all.
The range of red dots in the chart (< 28 Ct) indicates relatively low Ct values and active infections. The yellow range of dots, for which 28 < Ct <= 32, indicates possible infections, and the upper range of green dots, where Ct > 32, indicates that active infections were highly unlikely. It’s important to note that all of these tests were recorded as new COVID cases, so the range of Ct values suggest that testing in Rhode Island was unreasonably sensitive. That’s broadly true across the U.S. as well, which means that COVID cases are over-counted by perhaps 30% or more. And yet it is extremely difficult for subjects testing positive to learn their Ct values. You can ask, but you probably won’t get an answer, which is absurd and counterproductive.
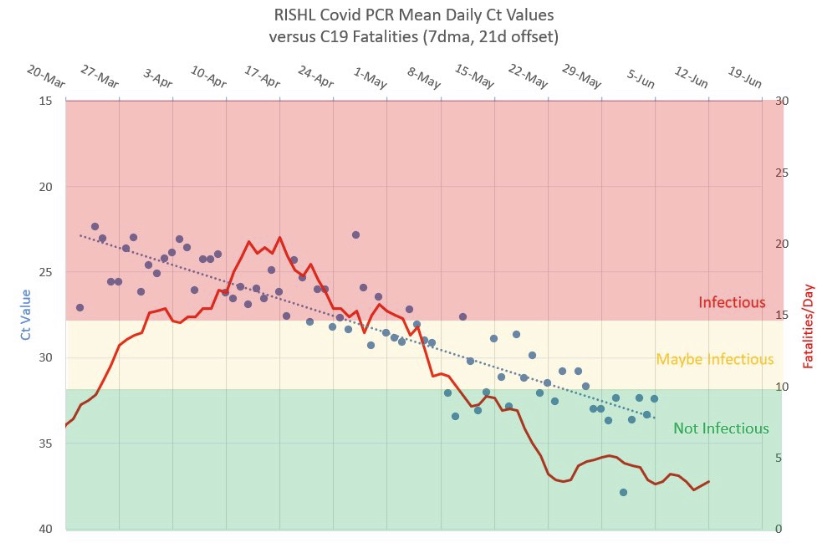
Notice that the concentration of red dots diminished over time, and we know that the spring wave of the virus in the Northeast was waning as the summer approached. The share of positives tests with high Ct values increased over that time frame, however. This is borne out by the next chart, which shows the daily mean Ct of these positive tests. The chart shows that active infections became increasingly rare over that time frame both because positive tests decreased and the average Ct value rose. What we don’t know is whether labs bumped up the number of cycles or replications to which samples were subjected. Still, the trend is rather disturbing because most of the positive cases in May and the first half of June were more likely to be virus remnants than live viruses.
It’s also worth noting that COVID deaths declined in concert with the upward trend in Ct values. This is shown in the chart below (where the Ct scale is inverted). This demonstrates the truly benign nature of positive tests having high Ct values.
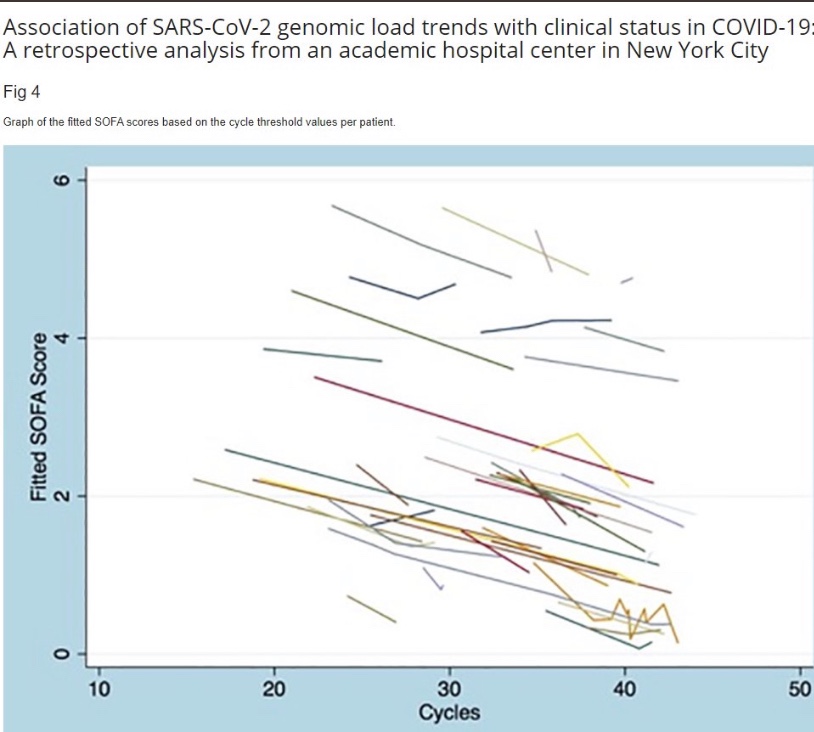
This is also demonstrated by the following data from a New York City academic hospital, which was posted by Andrew Bostom. It shows that a more favorable “clinical status” of COVID patients is associated with higher Ct values.
It’s astounding that the U.S. has relied so heavily on a diagnostic tool that gets so many subjects wrong. And it’s nearly impossible for subjects testing positive to obtain their Ct values. Instead, they are subject to self-quarantine for up to two weeks. Even worse, until recently there were delays in reporting the results of these tests of up to a week or more. That made them extremely unhelpful. On the other hand, thecoffee ground test is fast and cheap, and it might enhance the credibility of a subsequent positive PCR test, if one is necessary … and especially if the lab won’t report the Ct value.
The PCR test has identified far too many false infections, but it wouldn’t have been quite so damaging if 1) a reasonably low maximum cycle threshold had been established; 2) test results had not been subject to such long delays; and 3) rapid retests had been available for confirmation. The cycle threshold issue is starting to receive more attention, quite belatedly, and more rapid tests have become available. As I’ve emphasized in the past, cheap, rapid tests exist. But having dithered in February and March in approving even the PCR test, the FDA has remained extremely grudging in approving newer tests, and it persists in creating obstacles to their use. The FDA needs to wake up and smell the coffee!
My pre-Thanksgiving optimism about a crest in the fall wave of the coronavirus has been borne out for the Midwest and Mountain states in the U.S. These regions were the epicenter of the fall wave through October and most of November, but new cases in those states have continued to decline. Cases in a number of other states began to climb in November, however, contributing to a continuing rise in total new cases nationally. Some of these states are still in the throes of this wave, with the virus impacting subsets of the population that were relatively unscathed up till now.
My disclaimer: COVID is obviously a nasty virus. I don’t want to get it. However, on the whole, it is not a cataclysm on the order of many pandemics of the past. In fact, excess deaths this year will add just over 10% to projections of total deaths based on a five-year average. That level puts us in line with average annual deaths of about twenty years ago. And many of those excess deaths have been caused by our overreaction to the pandemic, not by the virus itself. As my endocrinologist has said, this is the greatest overreaction in all medical history. Unfortunately, a fading pandemic does not mean we can expect an end to the undue panic, or pretense for panic, on the part of interventionists.
This post will focus largely on trends in newly diagnosed COVID cases. I have been highly critical of our testing regime and COVID case counts because the most prominent diagnostic test (PCR) falsely identifies a large number of uninfected individuals as COVID-positive. However, case numbers are widely tracked and it’s fairly easy to find information across geographies for comparison. Deflate all the numbers by 30% if you want, or by any other factor, but please indulge me because I think the trends are meaningful, even if the absolute level of cases is inflated.
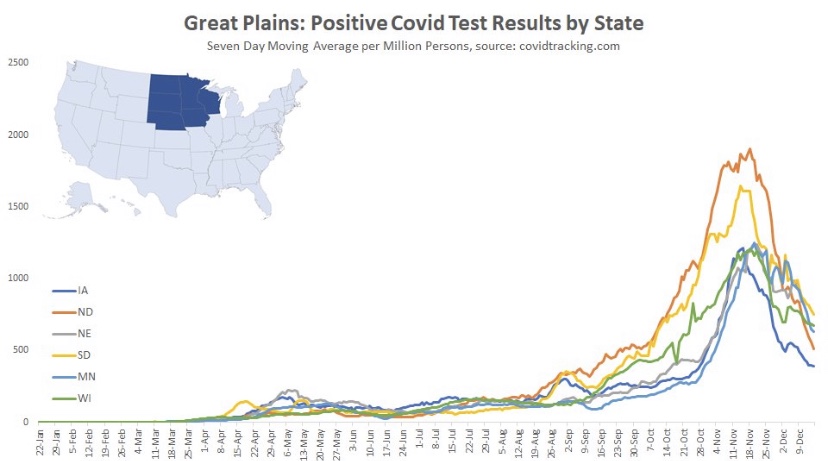
I’ll start with the good news and work my way down to states in which cases are still climbing (all of the following charts are from @Humble_Analysis (PLC)). The first chart is for the Great Plains, where cases peaked a little before Thanksgiving and have continued to fall since then. That peak came about six weeks after it began in earnest and cases have faded over the last four weeks.
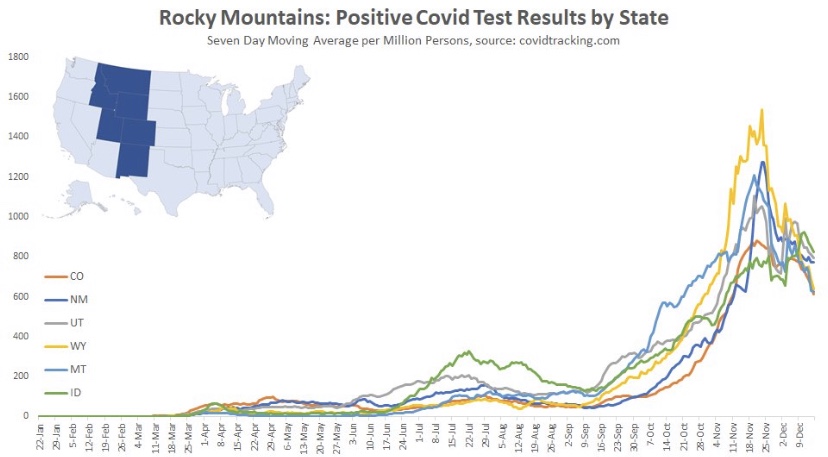
Next we have the Mountain states, where again, cases peaked around Thanksgiving, though Idaho saw a rebound after the holiday. You’ll see below that a number of states had a distinct drop in new cases during the week of Thanksgiving. There was somewhat of a pause in testing during that week, so the subsequent rebounds are largely due to a “catch-up” at testing sites, rather than some kind of Thanksgiving-induced spike in infections.
Back to the Mountain region, the peak came an average of about six or seven weeks into the wave, but the duration of the wave appears to have been longer in Montana and Wyoming.
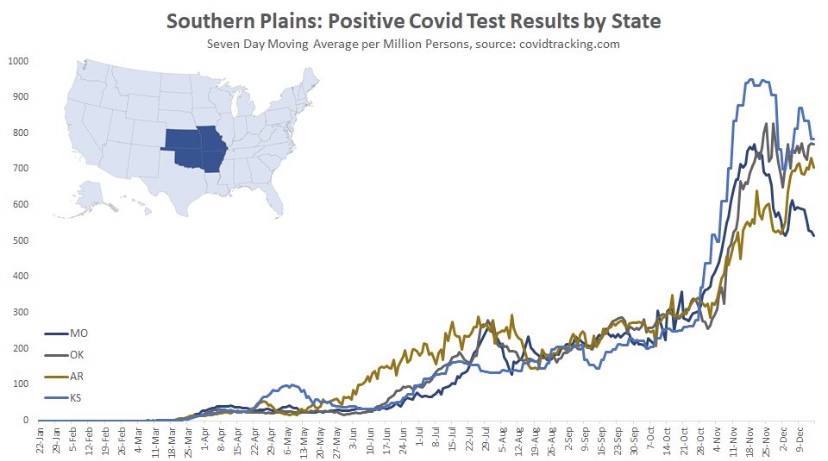
Here are the Southern Plain states, where cases plateaued around Thanksgiving (though cases in Missouri have clearly declined from their peak). In this region, case counts accelerated in October after a slow climb over the summer.
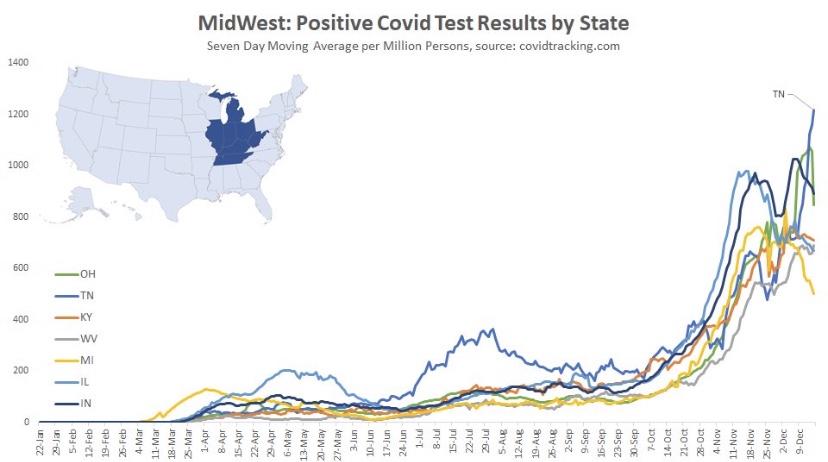
The situation is somewhat similar in the Midwest. where cases have generally plateaued. There were some post-Thanksgiving rebounds in several states, especially Tennessee. The wave began a little later in this region, in mid- to late October, and it is now seven to eight weeks into the wave, on average.
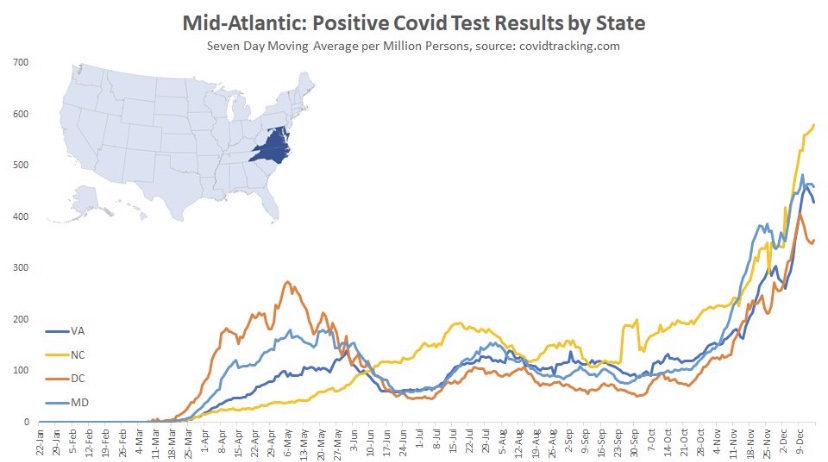
Here are the Mid-Atlantic states, which may be showing signs of a peak, though North Carolina has had the greatest caseload and is still climbing. These states are about seven weeks into the wave, on average.
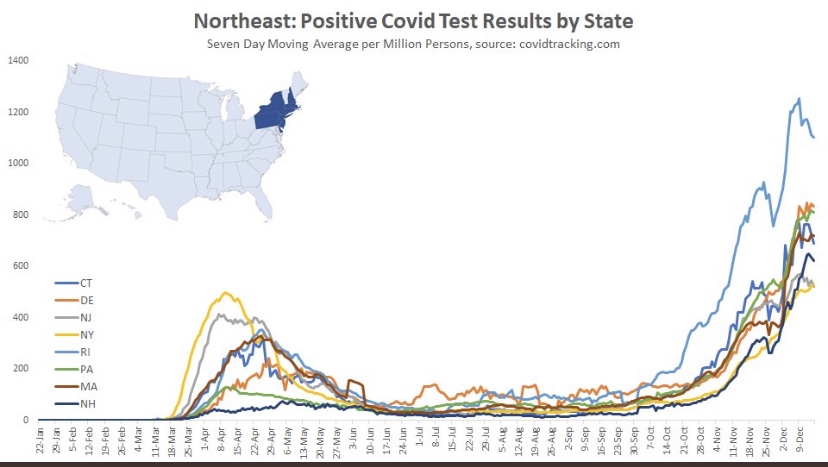
The Northeast also shows signs of a possible peak and is about seven weeks into the wave, except for Rhode Island, which saw an earlier onset and the most severe wave among these states.
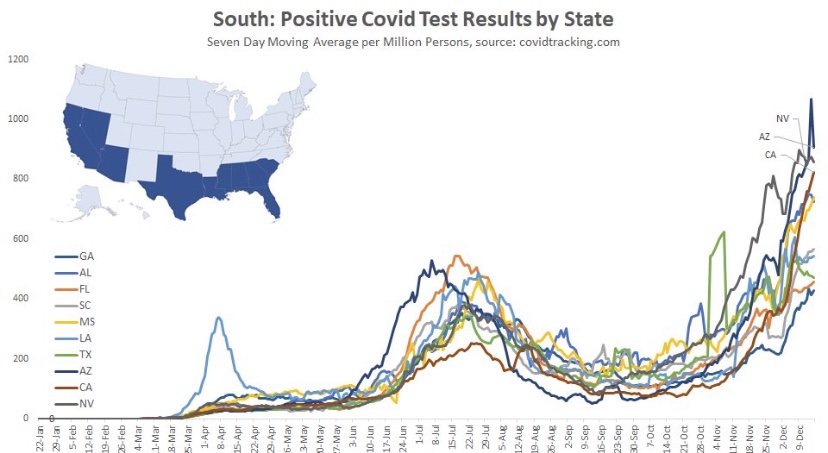
And finally we have the South, which is defined quite broadly in PLC’s construction. It’s a mixed bag, with a few states showing signs of a peak after about seven weeks. However, cases are still climbing in several states, notably California and Florida, among a few others.
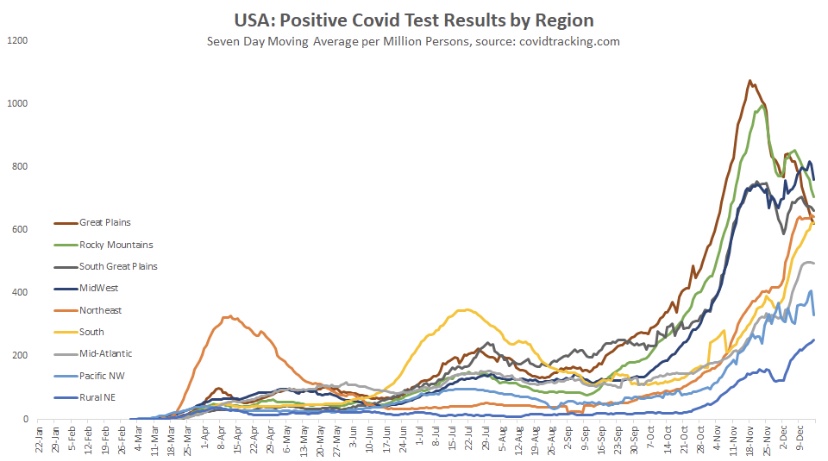
Oregon and Washington were skipped, but they appear as the Pacific NW in the following chart, along with aggregations for all the other regions. Maine is Part of the “Rural NE”, which was also skipped. The fall wave can be grouped roughly into two sets of regions: those in which waves began in late September or early October, and those where waves began in early to mid-November. The first group has moved beyond a peak or at least has plateaued. The latter group may be reaching peaks now or one hopes very soon. It seems to take about seven weeks to reach the peak of these regional waves, so a late December peak for the latter group would be consistent.
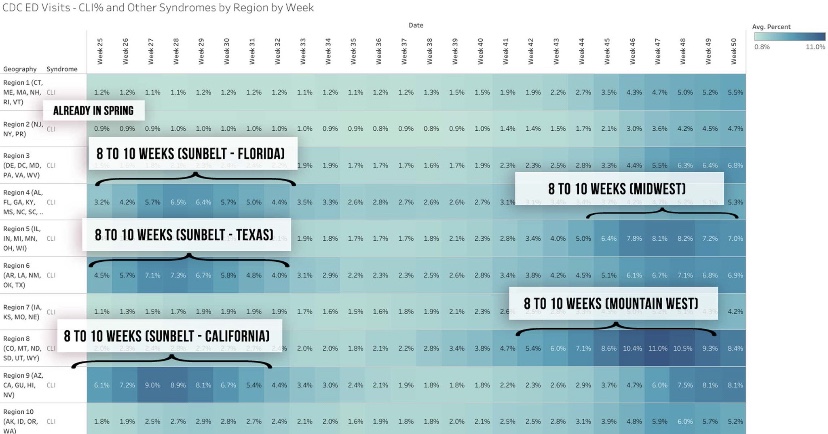
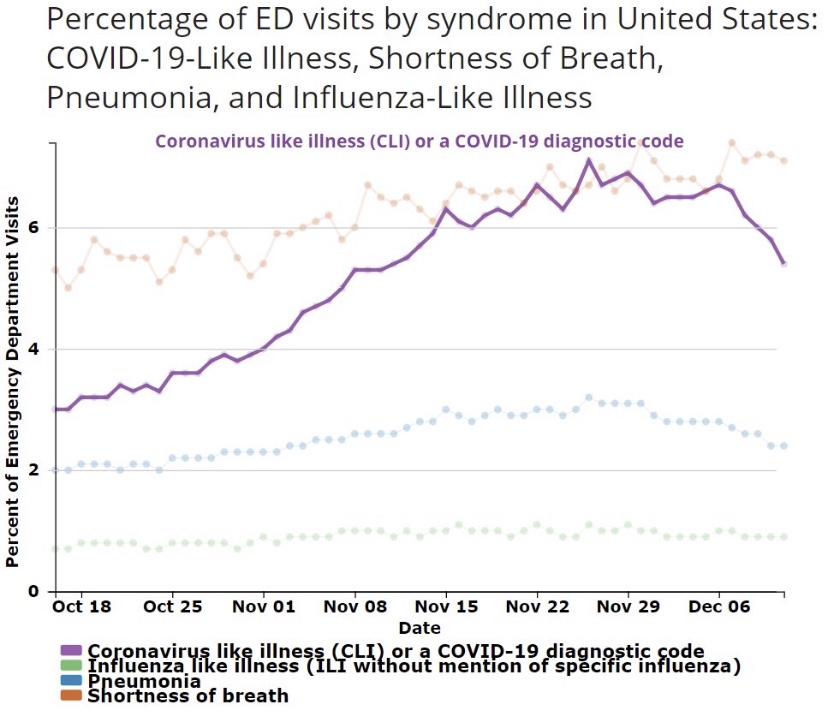
Justin Hart has a take on the duration of these waves, but he does so in terms of the share of emergency room (ER) visits in which symptoms of COVID-like illness (CLI) are presented. CLI tends to precede case counts slightly. Hart puts the duration of these waves at eight to ten weeks, but that’s a judgement call, and I might put it a bit longer using caseloads as a guide. Still, this color-coded chart from Hart is interesting.
If this sort of cyclical duration holds up, it’s consistent with the view that cases in many of the still “hot” states should be peaking this month.
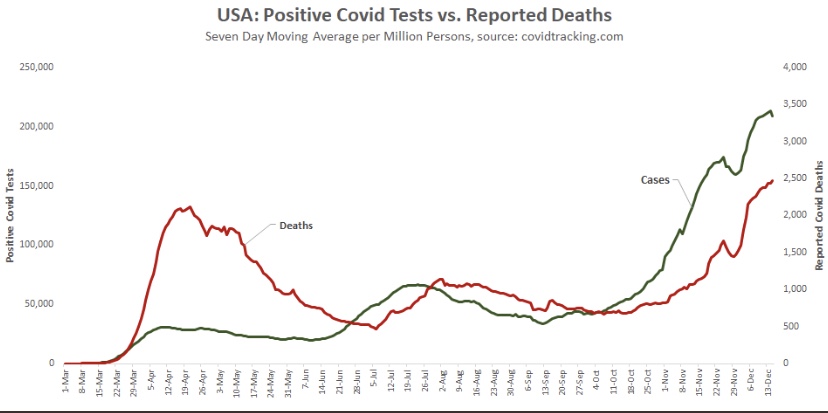
Aggregate cases for the U.S. appear below. The growth rate of new cases has slowed, and the peak is likely to occur soon. However, because it combines all of the regional waves, the duration of the wave nationwide will appear to be greater than for the individual regions. COVID-attributed deaths are also plotted, but they are reported deaths, not by date of death (DOD) or actual deaths, as I sometimes call them. Deaths by DOD are available only with a lag. As always, some of the reported deaths shown below occurred weeks before their reported date. Actual deaths were still rising as of late November, and are likely still rising. However, another indicator suggests they should be close to a peak.
A leading indicator of actual deaths I’ve discussed in the past now shows a more definitive improvement than it did just after Thanksgiving, as the next chart shows. This is the CLI share discussed above. An even better predictor of COVID deaths by actual DOD is the sum of CLI and the share of ER patients presenting symptoms of influenza-like illness (ILI), but ILI has been fairly low and stable, so it isn’t contributing much to changes in trend at the moment. There has been about a three-week lead between movements in CLI+ILI and COVID deaths by DOD.
(The reason the sum, CLI+ILI, has been a better predictor than CLI alone is because for some individuals, there are similarities in the symptoms of COVID and the flu.)
The chart shows that CLI peaked right around the Thanksgiving holiday (and so did CLI+ILI), but it remained on something of a plateau through the first week of December before declining. Some of the last few days on this chart are subject to revision, but the recent trend is encouraging. Allowing for a three-week lead, this indicates that peak deaths by DOD should occur around mid-December, but we won’t know exactly until early to mid-January. To be conservative, we might say the latter half of December will mark the peak in actual deaths.
The regional COVID waves this summer and fall seem to have run their course within 10 – 12 weeks. Several former hot spots have seen cases drop since Thanksgiving after surges of six to seven weeks. However, there are several other regions with populous states where the fall wave is still close to “mid-cycle”, as it were, showing signs of possible peaks after roughly seven weeks of rising cases. The national CLI share peaked around Thanksgiving, but it did not give up much ground until early December. That suggests that actual deaths (as opposed to reported deaths), at least in some regions, will peak around the time of the winter solstice. Let’s hope it’s sooner.
Successive waves within a region seem to reach particular subsets of the population with relatively few reinfections. The 10 – 12 week cycle discussed above is sufficient to achieve an effective herd immunity within these subsets. But once again, a large share of the vulnerable, and a large share of COVID deaths, are still concentrated in the elderly, high-risk population and in care homes. The vaccine(s) currently being administered to residents of those homes are likely to hasten the decline in COVID deaths beginning sometime in January, perhaps as early as mid-month. By then, however, we should already see a decline underway as this wave of the virus finally burns itself out. As vaccines reach a larger share of the population through the winter and spring, the likelihood of additional severe waves of the virus will diminish.
Lest there be any misunderstanding, the reasons for the contagion’s fade to come have mostly to do with reaching the effective herd immunity threshold within afflicted subsets of the population (sub-herds). Social distancing certainly plays a role as well. Nearly all of that is voluntary, though it has been encouraged by panicked pronouncement by certain public officials and the media. Direct interventions or lockdown measures are in general counter-productive, however, and they create a death toll of their own. Unfortunately, the fading pandemic might not rein-in the curtailment of basic liberties we’ve witnessed this year.
What does it take to shake people out of their statist stupor? Evidently, the sweet “logic” of universal confinement is very appealing to the prescriptive mindset of busybodies everywhere, who anxiously wag their fingers at those whom they view as insufficiently frightened. As difficult as it is for these shrieking, authoritarian curs to fathom, measures like lockdowns, restrictions on business activity, school closures, and mandates on behavior have at besta limited impact on the spread of the coronavirus, and they are enormously costly in terms of economic well-being and many dimensions of public health. Yet the storm of propaganda to the contrary continues. Media outlets routinely run scare stories, dwelling on rising case numbers but ignoring them when they fall; they emphasize inflated measures of pandemic severity; certain researchers and so-called health experts can’t learn the lessons that are plain in the data; and too many public officials feel compelled to assert presumed but unconstitutional powers. At least the World Health Organization has managed to see things clearly, but many don’t want to listen.
I’ll be the first to say I thought the federalist approach to COVID policy was commendable: allow states and local governments to craft policies appropriate to local conditions and political preferences, rather than have the federal government dictate a one-size-fits-all policy. I haven’t wavered in that assessment, but let’s just say I expected more variety. What I failed to appreciate was the extent to which state and local leaders are captive to provincial busybodies, mavens of precautionary excess, and fraudulent claims to scientific wisdom.
Of course, it should be obvious that the “knowledge problem” articulated by Friedrich Hayek is just as dangerous at low-levels of government as it is in a central Leviathan. And it’s not just a knowledge problem, but a political problem: officials become panicked because they fear bad outcomes will spell doom for their careers. Politicians are particularly prone to the hazards of “do-somethingism”, especially if they have willing, status-seeking “experts” to back them up. But as Scott Sumner says:
“When issues strongly impact society, the science no longer ‘speaks for itself’.
Well, the science is not quite as clear as the “follow-the-science” crowd would have you believe. And unfortunately, public officials have little interest in sober assessments of the unintended effects of lockdown policy.
In my last post, I presented a simple framework for thinking about the benefits and costs of lockdown measures, or non-pharmaceutical interventions (NPIs). I also emphasized the knowledge problem: even if there is some point at which NPI stringencies are “optimized”, government does not possess the knowledge to find that point. It lacks detailed information on both the costs and benefits of NPIs, but individual actors know their own tolerance for risk, and they surely have some sense of the risks they pose to others in their normal course of affairs. While voluntary precautions might be imperfect, they accomplish much of what interventionists hope will be gained via coercion. But, in an effort to “sell” NPIs to constituents and assert their authority, officials vastly over-estimate benefits of NPIs and under-estimate the costs.
NPI Stringency and COVID Outcomes
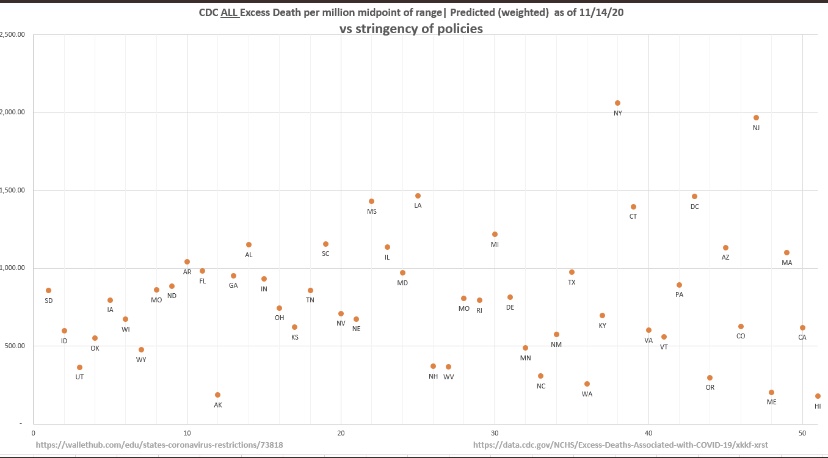
Let’s take a look at a measure of the strength of NPIs by state — the University of Oxford Stringency Index — and compare those to CDC all-cause excess deaths in each state. If it’s hard to read, try clicking on the image or turn your phone sideways. This plot covers outcomes through mid-November:
The chart doesn’t suggest any benefit to the imposition of greater restrictions, or more stringent NPIs. In fact, the truth is that people will do most of the work on their own based on perceptions of risk. That’s partly because government restrictions add little risk mitigation to what can be accomplished by voluntary social distancing and other precautions.
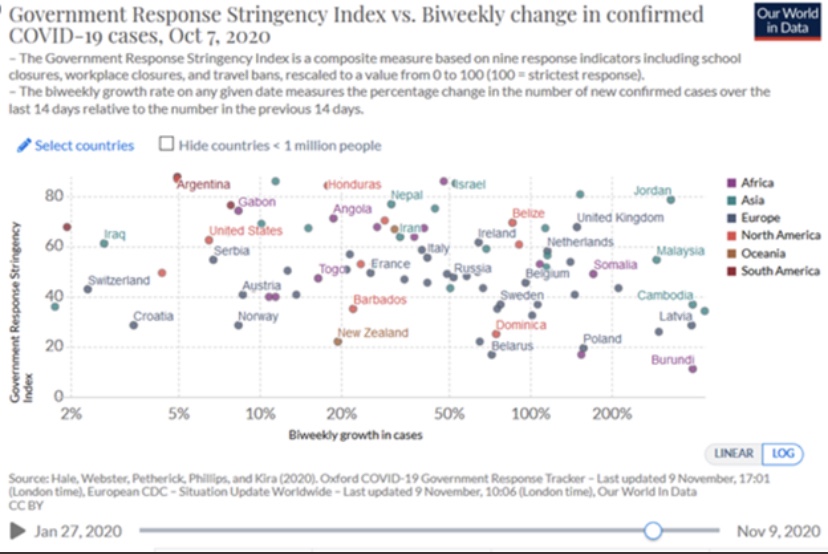
Here’s a similar chart with cross-country comparisons, though the data here ended in early October (I apologize for the fuzzy image):
But what about reverse causality? Maybe the imposition of stringency was a response to more severe contagions. Now that the virus has swept most of the U.S and Europe in three distinct waves, and given the variety and timing of NPIs that have been tried, it’s harder to make that argument. States like South Dakota have done fairly well with low stringency, while states like New Jersey with high stringency have fared poorly. The charts above provide multiple pair-wise examples and counter-examples of states or countries having faced hard waves with different results.
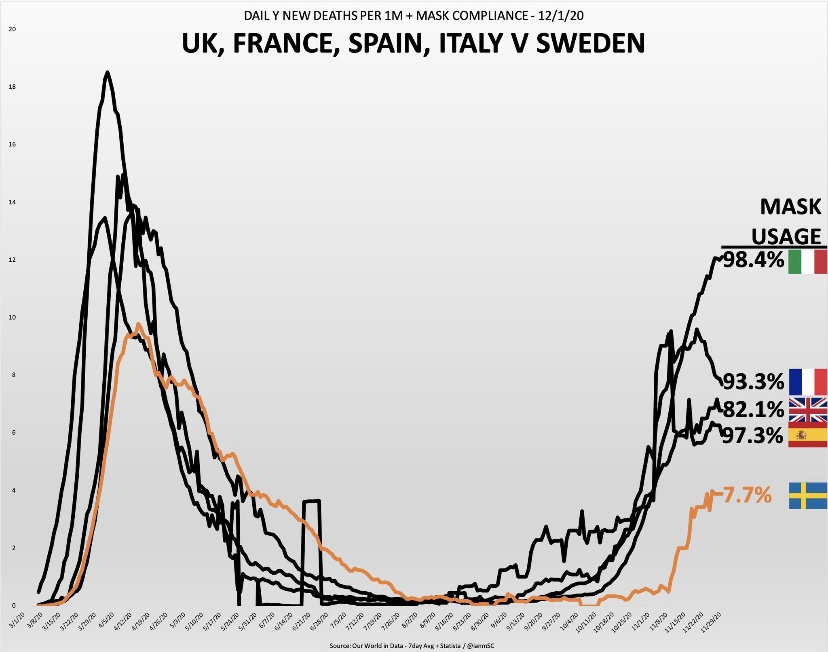
But let’s look at a few specific situations.
The countries shown above have converged somewhat over the past month: Sweden’s daily deaths have risen while the others have declined to greater or lesser degrees, but the implications for mask usage are unaltered.
And of course we have this gem, predicated on the mental gymnastics lockdown enthusiasts are fond of performing:
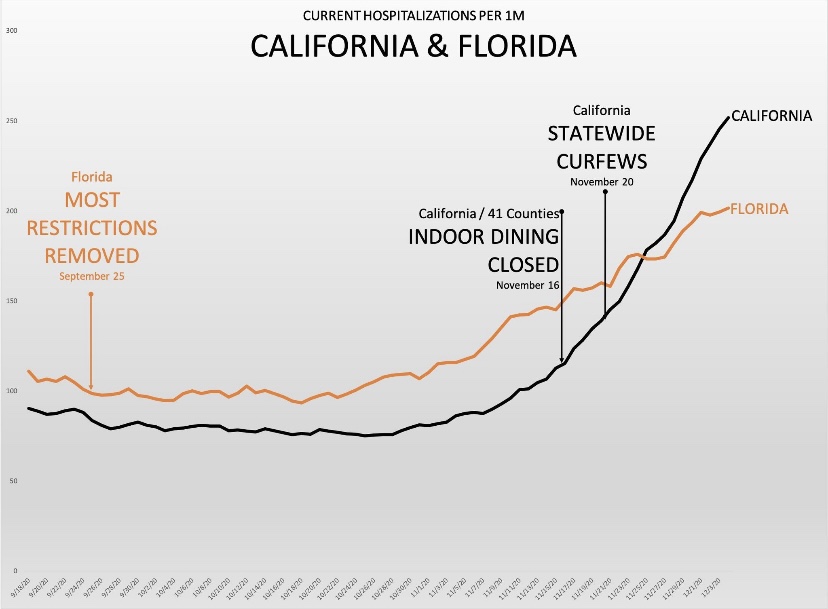
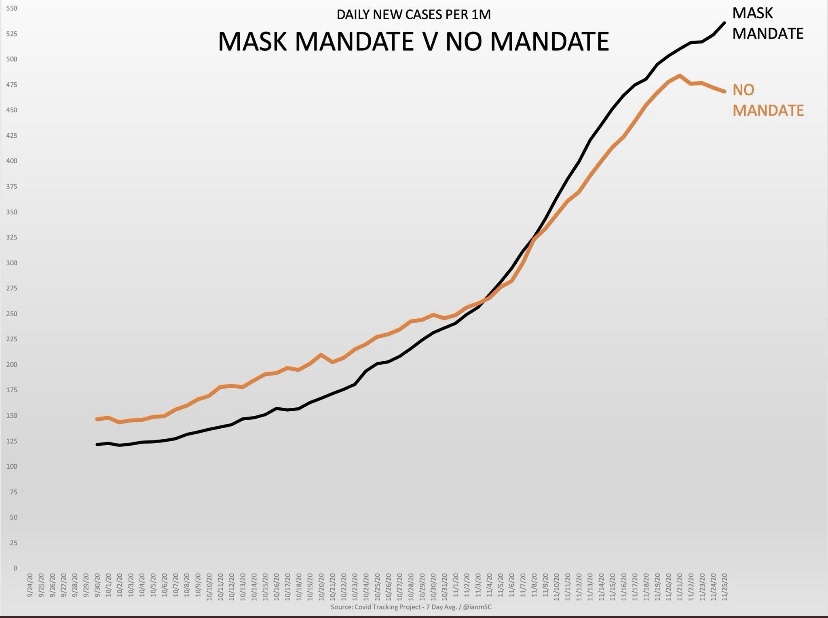
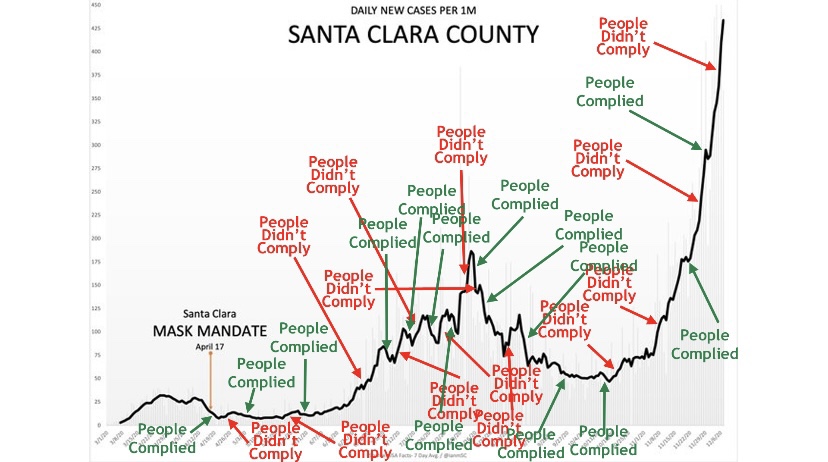
But seriously, it’s been a typical pattern: cases rise to a point at which officials muster the political will to impose restrictions, often well after the “exponential” phase of the wave or even the peak has passed. For the sake of argument, if we were to stipulate that lockdowns save lives, it would take time for these measures to mitigate new infections, time for some of the infected individuals to become symptomatic, and more time for diagnosis. For the lockdown arguments to be persuasive, the implementation of NPIs would have to precede the point at which the growth of cases begins to decline by a few weeks. That’s something we’ve seldom observed, but officials always seem to take credit for the inevitable decline in cases.
More informed lockdown proponents have been hanging their hats on this paper in Nature by Seth Flaxman, et al, published in July. As Philippe LeMoine has shown, however, Flaxman and his coauthors essentially assumed their result. After a fairly exhaustive analysis, Lemoine, a man who understands sophisticated mathematics, offers these damning comments:
“Their paper is a prime example of propaganda masquerading as science that weaponizes complicated mathematics to promote questionable policies. Complicated mathematics always impresses people because theydon’t understand it and it makes the analysis look scientific, but often it’s used to launder totally implausible assumptions, which anyone could recognize as such if they were stated in plain language. I think it’s exactly what happened with Flaxman et al.’s paper, which has been used as a cudgel to defend lockdowns, even though it has no practical relevance whatsoever.”
The Economic Costs of Stringency
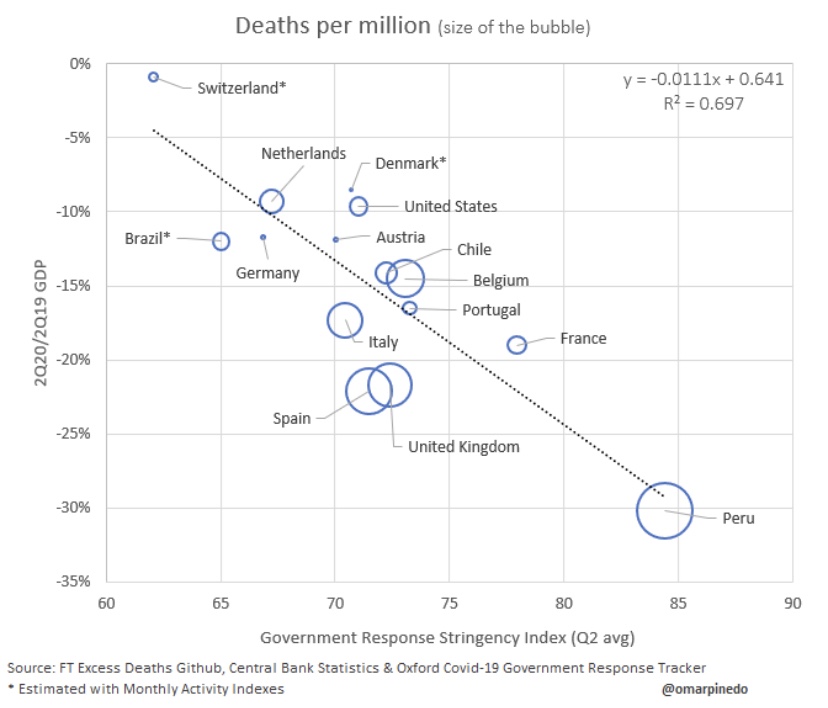
So the benefits of stringent lockdowns in terms of averting sickness and death from COVID are speculative at best. What about the costs of lockdowns? We can start with their negative impact on economic activity:
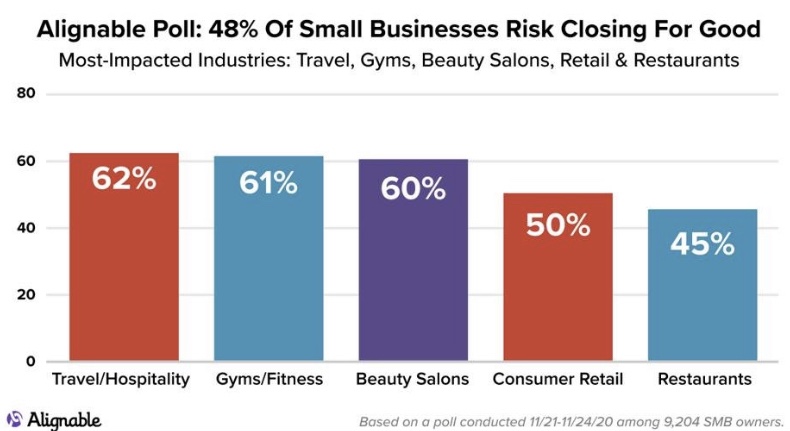
That’s a pretty bad reflection on NPI stringency. In the U.S, a 10% decline in GDP in 2020 amounts to about $2.1 trillion in lost goods and services. That’s just for starters. The many destroyed businesses and livelihoods carry an ongoing cost that could take years to fade, as this graphic on permanent business closures shows:
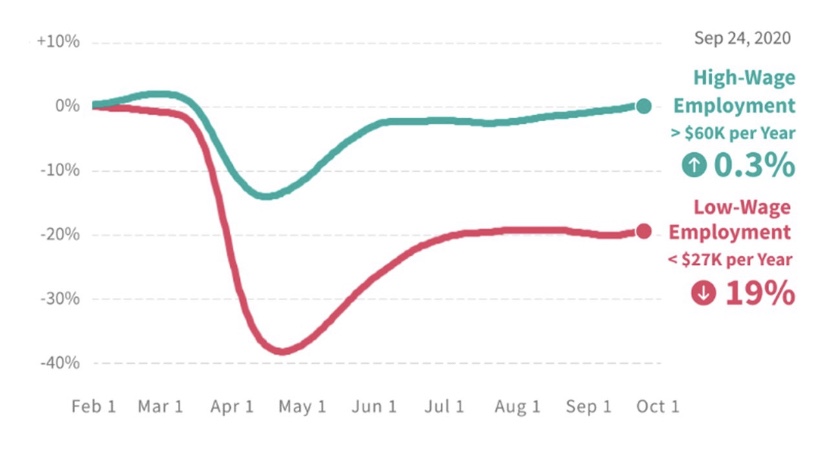
If you’re wondering about the distributional effects of lockdowns, here’s more bad news:
It’s possible to do many high-paying jobs from home. Not so for blue-collar workers. And distributional effects by size of enterprise are also heavily-skewed in favor of big companies. Within the retail industry, big-box stores are often designated as “essential”, while small shops and restaurants are not. The restaurant industry has been destroyed in many areas, inflicting a huge blow to owners and workers. This despite evidence from contact tracing showing that restaurants and bars account for a very small share of transmission. To add insult to injury, many restaurants invested heavily in safety measures and equipment to facilitate new, safer ways of doing business, only to be double-crossed by officials like Andrew Cuomo and Eric Garcetti, who later shut them down.
Public Health Costs of Stringency
Lives are lost due to lockdowns, but here’s a little exercise for the sake of argument: The life value implied by individual willingness-to-pay for risk reduction comes in at less than $4 million. Even if the supposed 300,000 COVID deaths had all been saved by lockdowns, that would have amounted to a value of $1.2 trillion, about half of the GDP loss indicated above. Of course, it would be outrageously generous to concede that lives saved by NPI’s have approached 300,000, so lockdowns fall far short at the very outset of any cost-benefit comparison, even if we value individual lives at far more than $4 million.
As AJ Kay says, the social and human costs go far beyond economic losses:
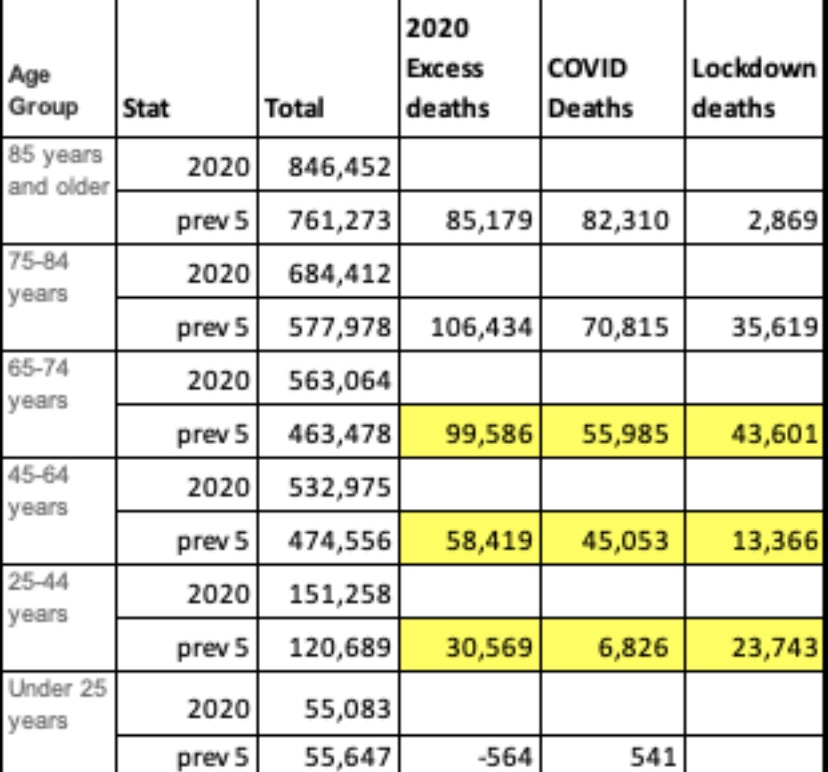
I cited specific examples of losses in many of these categories in an earlier post. But for the moment, instead of focusing on causes of death, take a look at this table provided by Justin Hart showing a measure of non-COVID excess deaths by age group in the far right-hand column:
The numbers here are derived by averaging deaths by age group over the previous five years and subtracting COVID deaths in each group. I believe Hart’s numbers go through November. Of greatest interest here is the fact that younger age groups, having far less risk of death from COVID than older age groups, have suffered large numbers of excess deaths NOT attributed to COVID. As Hart notes later in his thread:
These deaths are a tragic consequence of lockdowns.
Educational Costs of Stringency
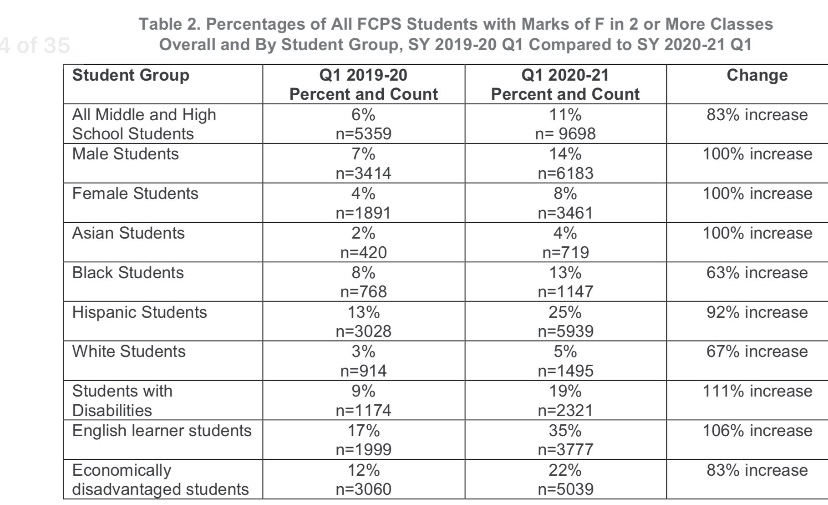
Many schools have been closed to in-person instruction during the pandemic, leading to severe disruptions to the education f children. This report from the Fairfax County, VA School District is indicative, and it is extremely disheartening. The report includes the following table:
Note the deterioration for disabled students, English learners, and the economically disadvantaged. The surfeit of failing grades is especially damaging to groups already struggling in school relative to their peers, such as blacks and Hispanics. Not only has the disruption to in-person instruction been disastrous to many students and their futures; it has also yielded little benefit in mitigating the contagion. A recent study in The Lancet confirms once again that transmission is low in educational settings. Also see here and here for more evidence on that point.
Conclusion
It’s clear that the “follow-the-science” mantra as a rationale for stringent NPIs was always a fraud, as was the knee-jerk response from those who conflated lockdowns with “leadership”. Such was the wrongheaded and ultimately deadly pressure to “do something”. We can be thankful that pressure was resisted at the federal level by President Trump. The extraordinary damage inflicted by ongoing NPIs was quite foreseeable, but there is one more very ominous implication. I’ll allow J.D. Tucille to sum that up with some of the pointed quotes he provides:
“‘The first global pandemic of the digital age has accelerated the international adoption of surveillance and public security technologies, normalising new forms of widespread, overt state surveillance,’ warned Kelsey Munro and Danielle Cave of the Australian Strategic Policy Institute’s Cyber Policy Centre last month.
‘Numerous governments have used the COVID-pandemic to repress expression in violation of their obligations under human rights law,’ United Nations Special Rapporteur on Freedom of Expression David Kaye noted in July.
‘For authoritarian-minded leaders, the coronavirus crisis is offering a convenient pretext to silence critics and consolidate power,’ Human Rights Watch warned back in April.
There’s widespread agreement, then, that government officials around the world are exploiting the pandemic to expand their power and to suppress opposition. That’s the case not only among the usual suspects where authorities don’t pretend to take elections and civil liberties seriously, but also in countries that are traditionally considered ‘free.’ … It’s wildly optimistic to expect that newly acquired surveillance tools and enforcement powers will simply evaporate once COVID-19 is sent on its way. The post-pandemic new normal is almost certain to be more authoritarian than what went before.”
In advanced civilizations the period loosely called Alexandrian is usually associated with flexible morals, perfunctory religion, populist standards and cosmopolitan tastes, feminism, exotic cults, and the rapid turnover of high and low fads---in short, a falling away (which is all that decadence means) from the strictness of traditional rules, embodied in character and inforced from within. -- Jacques Barzun