Tags
Acquired Immunity, Anthony Fauci, Covid-19, Herd Immunity, Hererogeneity, HIT, Masks, Max Planck Institute, Measles, MMR Vaccine, R0, Reproduction Rate, T-Cells. Pre-Immunity, Tyler Cowen, Vaccinations. Fragile Immunity

Anthony Fauci has repeatedly increased his estimate of how much of the population must be vaccinated to achieve what he calls herd immunity, and he did it again in late December. This series of changes, and other mixed messages he’s delivered in the past, reveal Fauci to be a “public servant” who feels no obligation to level with the public. Instead, he crafts messages based on what he believes the public will accept, or on his sense of how the public must be manipulated. For example, by his own admission, his estimates of herd immunity have been sensitive to polling data! He reasoned that if more people reported a willingness to take a vaccine, he’d have flexibility to increase his “public” estimate of the percentage that must be vaccinated for herd immunity. Even worse, Fauci appears to lack a solid understanding of the very concept of herd immunity.
Manipulation
There is so much wrong with his reasoning on this point that it’s hard to know where to start. In the first place, why in the world would anyone think that if more people willingly vaccinate it would imply that even more must vaccinate? And if he felt that way all along it demonstrates an earlier willingness to be dishonest with the public. Of course, there was nothing scientific about it: the series of estimates was purely manipulative. It’s almost painful to consider the sort of public servant who’d engage in such mental machinations.
Immunity Is Multi-Faceted
Second, Fauci seemingly wants to convince us that herd immunity is solely dependent on vaccination. Far from it, and I’m sure he knows that, so perhaps this too was manipulative. Fauci intimates that COVID herd immunity must look something like herd immunity to the measles, which is laughable. Measles is a viral infection primarily in children, among whom there is little if any pre-immunity. The measles vaccine (MMR) is administered to young children along with occasional boosters for some individuals. Believe it or not, Fauci claims that he rationalized a requirement of 85% vaccination for COVID by discounting a 90% requirement for the measles! Really???
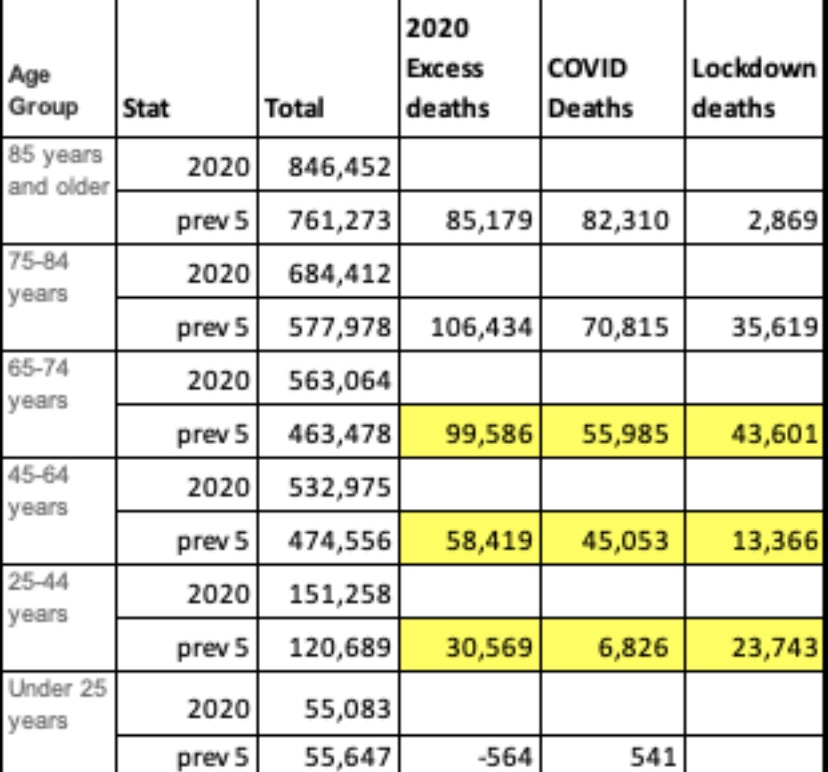
In fact, there is substantial acquired pre-immunity to COVID. A meaningful share of the population has long-memory, cross-reactive T-cells from earlier exposure to coronaviruses such as the common cold. Estimates range from 10% to as much as 50%. So if we stick with Fauci’s 85% herd immunity “guesstimate”, 25% pre-immunity implies that vaccinating only 60% of the population would get us to Fauci’s herd immunity goal. (Two qualifications: 1) the vaccines aren’t 100% effective, so it would take more than 60% vaccinated to offset the failure rate; 2) the pre-immune might not be identifiable at low cost, so there might be significant overlap between the pre-immune and those vaccinated.)
Conceptual Confusion
Vaccinations approaching 85% would be an extremely ambitious goal, especially if it is recommended annually or semi-annually. It would be virtually impossible without coercion. While more than 91% of children are vaccinated for measles in the U.S., it is not annual. Thus, measles does not offer an appropriate model for thinking about herd immunity to COVID. Less than half of adults get a flu shot each year, and somewhat more children.
Fauci’s reference to 85% – 90% total immunity is different from the concept of the herd immunity threshold (HIT) in standard epidemiological models. The HIT, often placed in the range of 60% – 70%, is the point at which new infections begin to decline. More infections occur above the HIT but at a diminishing rate. In the end, the total share of individuals who become immune due to exposure, pre-immunity or vaccination will be greater than the HIT. The point is, however, that reaching the HIT is a sufficient condition for cases to taper and an end to a contagion. If we use 65% as the HIT and pre-immunity of 25%, only 40% must be vaccinated to reach the HIT.
Heterogeneity
A recent innovation in epidemiological models is the recognition that there are tremendous differences between individuals in terms of transmissibility, pre-immunity, and other factors that influence the spread of a particular virus, including social and business arrangements. This kind of heterogeneity tends to reduce the effective HIT. We’ve already discussed the effect of pre-immunity. Suppose that certain individuals are much more likely to transmit the virus than others, like so-called super-spreaders. They spur the initial exponential growth of a contagion, but there are only so many of them. Once infected, no one else among the still-susceptible can spread the virus with the same force.
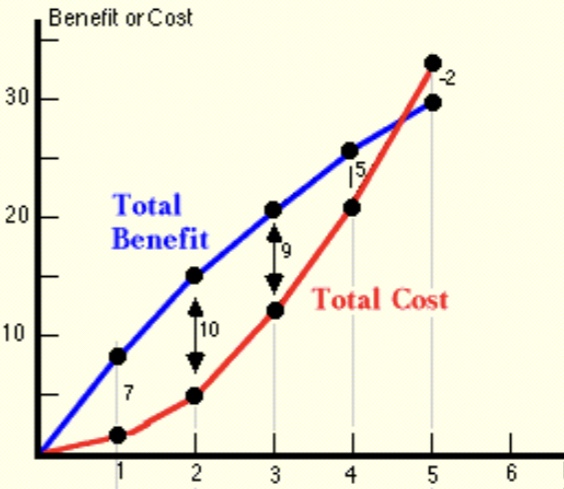
Researchers at the Max Planck Institute (and a number of others) have gauged the effect of introducing heterogeneity to standard epidemiological models. It is dramatic, as the following chart shows. The curves simulate a pandemic under different assumptions about the degree of heterogeneity. The peak of these curves correspond to the HIT under each assumption (R0 refers to the initial reproduction number from infected individuals to others).

Moderate heterogeneity implies a HIT of only 37%. Given pre-immunity of 25%, only an additional 12% of the population would have to be infected or vaccinated to prevent a contagion from gaining a foothold for the initial exponential stage of growth. Fauci’s herd immunity figure obviously fails to consider the effect of heterogeneity.
How Close To the HIT?
We’re not as far from HITs as Fauci might think, and a vaccination goal of 85% is absurd and unnecessary. The seasonal COVID waves we’ve experienced thus far have faded over a period of 10-12 weeks. Estimates of seroprevalence in many localities reached a range of 15% – 25% after those episodes, which probably includes some share of those with pre-immunity. To reach the likely range of a HIT, either some additional pre-immunity must have existed or the degree of heterogeneity must have been large in these populations.
But if that’s true, why did secondary waves occur in the fall? There are a few possibilities. Of course, some areas like the upper Midwest did not experience the springtime wave. But in areas that suffered a recurrance, perhaps the antibodies acquired from infections did not remain active for as long as six months. However, other immune cells have longer memories, and re-infections have been fairly rare. Another possibility is that those having some level of pre-immunity were still able to pass live virus along to new hosts. But this vector of transmission would probably have been quite limited. Pre-immunity almost surely varies from region to region, so some areas were not as firmly above their HITs as others. It’s also possible that infections from super-spreaders were concentrated within subsets of the population even within a given region, in certain neighborhoods or among some, but not all, social or business circles. Therefore, some subsets or “sub-herds” achieved a HIT in the first wave, but it was unnecessary for other groups. In other words, sub-herds spared in the first wave might have suffered a contagion in a subsequent wave. And again, reinfections seem to have been rare. Finally, there is the possibility of a reset in the HIT in the presence of a new, more transmissible variant of the virus, as has become prevalent in the UK, but that was not the case in the fall.
Fragility
Tyler Cowen has mentioned another possible explanation: so-called “fragile” herd immunity. The idea is that any particular HIT is dependent on the structure of social relations. When social distancing is widely practiced, for example, the HIT will be lower. But if, after a contagion recedes, social distancing is relaxed, it’s possible that the HIT will take a higher value at the onset of the next seasonal wave. Perhaps this played a role in the resurgence in infections in the fall, but the HIT can be reduced via voluntary distancing. Eventually, acquired immunity and vaccinations will achieve a HIT under which distancing should be unnecessary, and heterogeneity suggests that shouldn’t be far out of reach.
Conclusion
Anthony Fauci has too often changed his public pronouncements on critical issues related to management of the COVID pandemic. Last February he said cruises were fine for the healthy and that most people should live their lives normally. Oops! Then came his opinion on the limited effectiveness of masks, then a shift to their necessity. His first position on masks has been called a “noble lie” intended to preserve supplies for health care workers. However, Fauci was probably repeating the standing consensus at that point (and still the truth) that masks are of limited value in containing airborne pathogens.
This time, Fauci admitted to changing his estimate of “herd immunity” in response to public opinion, a pathetic approach to matters of public health. What he called herd immunity was really an opinion about adequate levels of vaccination. Furthermore, he neglected to consider other forms of immunity: pre-existing and already acquired. He did not distinguish between total immunity and the herd immunity threshold that should guide any discussion of pandemic management. He also neglected the significant advances in epidemiological modeling that recognize the reality of heterogeneity in reducing the herd immunity threshold. The upshot is that far fewer vaccinations are needed to contain future waves of the pandemic than Fauci suggests.