Tags
American Journal of Epidemiology, Andrew Cuomo, Anthony Fauci, Banality of Evil, CDC, City Journal, CMS, Donald Trump, Elective Surgery, Epidemiological Models, FDA, Gavin Newsom, Gretchen Whitmer, Harvey Risch, Hydroxychloraquin, Import Controls, Joel Zinberg, Lockdowns, Newsweek, NIH, Phil Murphy, Politico, PPE, Price Gouging, Prophylaxis, Quarantines, Steve Sisolak, The Lancet, Tom Wolf, Yale School of Public Health

Policymakers, public health experts, and the media responded to the coronavirus in ways that have often undermined public health and magnified the deadly consequences of the pandemic. Below I offer several examples of perverse politics and policy prescriptions, and a few really bad decisions by certain elected officials. Some of the collateral damage was intentional and motivated by an intent to inflict political damage on Donald Trump, and people of good faith should find that grotesque no matter their views on Trump’s presidency.
Politicized Treatment
The smug dismissal of hydroxychloraquine as Trumpian foolishness was a crime against humanity. We now know HCQ works as an early treatment and as a prophylactic against infection. It’s has been partly credited with stanching “hot spots” in India as well as contributing strongly to control of the contagion in Switzerland and in a number of other countries. According to epidemiologist Harvey Risch of the Yale School of Public Health, HCQ could save 75,000 to 100,000 lives if the drug is widely used. This is from Dr. Risch’s OpEd in Newsweek:
“On May 27, I published an article in the American Journal of Epidemiology (AJE) entitled, ‘Early Outpatient Treatment of Symptomatic, High-Risk COVID-19 Patients that Should be Ramped-Up Immediately as Key to the Pandemic Crisis.’ That article, published in the world’s leading epidemiology journal, analyzed five studies, demonstrating clear-cut and significant benefits to treated patients, plus other very large studies that showed the medication safety. …
Since [then], seven more studies have demonstrated similar benefit. In a lengthy follow-up letter, also published by AJE, I discuss these seven studies and renew my call for the immediate early use of hydroxychloroquine in high-risk patients.”
Risch is careful to couch his statements in forward-looking terms, but this also implies that tens of thousands of lives could have been saved, or patients might have recovered more readily and without lasting harm, had use of the drug not been restricted. The FDA revoked its Emergency Use Authorization for HCQ on June 15th, alleging that it is not safe and has little if any benefit. An important rationale cited in the FDA’s memo was an NIH study of late-stage C19 patients that found no benefit and potential risks to HCQ, but this is of questionable relevance because the benefit appears to be in early-stage treatment or prophylaxis. Poor research design also goes for this study and this study, while this study shared in some shortcomings (e.g., and no use of and/or controls for zinc) and a lack of statistical power. Left-wing outlets like Politico seemed almost gleeful, and blissfully ignorant, in calling those studies “nails in the coffin” for HCQ. Now, I ask: putting the outcomes of the research aside, was it really appropriate to root against a potential treatment for a serious disease, especially back in March and April when there were few treatment options, but even now?
Then we have the state governors who restricted the use of HCQ for treating C19, such as Gretchen Whitmer (MI) and Steve Sisolak (NV). Andrew Cuomo (NY) decided that HCQ could be dispensed only for hospital use, exactly the wrong approach for early stage treatment. And all of this resistance was a reaction to Donald Trump’s optimism about the promise of HCQ. Yes, there was alarm that lupus patients would be left without adequate supplies, but the medication is a very cheap, easy to produce drug, so that was never a real danger. Too much of the media and politicians have been complicit in denying a viable treatment to many thousands of C19 victims. If you were one of the snarky idiots putting it down on social media, you are either complicit or simply a poster child for banal evil.
Seeding the Nursing Homes
The governors of several states issued executive orders to force nursing homes to accept C19 patients, which was against CMS guidance issued in mid-March. The governors were Andrew Cuomo (NY), Gretchen Whitmer (MI), Gavin Newsom (CA), Tom Wolf (PA), and Phil Murphy (PA). This was a case of stupidity more than anything else. These institutions are home to the segment of the population most vulnerable to the virus, and they have accounted for about 40% of all C19 deaths. Nursing homes were ill-prepared to handle these patients, and the governors foolishly and callously ordered them to house patients who required a greater level of care and who represented an extreme hazard to other residents and staff.
Party & Protest On
Then of course we had the mayor of New York City, Bill De Blasio, who urged New Yorkers to get out on the town in early March. That was matched in its stupidity by the array of politicians and health experts who decided, having spent months proselytizing the need to “stay home”, that it was in their best interests to endorse participation in street protests that were often too crowded to maintain effective social distance. That’s not a condemnation of those who sought to protest peacefully against police brutality, but it was not a good or consistent recommendation in the domain of public health. Thankfully, the protests were outside!
Testing, Our Way Or the Highway
The FDA and CDC were guilty of regulatory overreach in preventing early testing for C19, and were responsible for many lives lost early in the pandemic. By the time the approved CDC tests revealed that the virus was ramping up drastically in March, the country was already behind in getting a handle on the spread of the virus, quarantining the infected, and tracing their contacts. There is no question that this cost lives.
Masks… Maybe, But Our Way Or the Highway
U.S. public health authorities were guilty of confused messaging on the efficacy of masks early in the pandemic. As Joel Zinberg notes in City Journal, Anthony Fauci admitted that his own minimization of the effectiveness of masks was motivated by a desire to prevent a shortage of PPE for health care workers:
“In discouraging mask use, Fauci—for decades, the nation’s foremost expert on viral infectious diseases—was not acting as a neutral interpreter of settled science but as a policymaker, concerned with maximizing the utility of the limited supply of a critical item. An economist could have told him that there was no need to misinform the public. Letting market mechanisms work and relaxing counterproductive regulations would ease shortages. Masks for health-care workers would be available if we were willing to pay higher prices; those higher prices, in turn, would elicit more mask production.”
Indeed, regulators made acquisition of adequate supplies of PPE more difficult than necessary via compliance requirements, “price gouging” rules, and import controls.
Bans on Elective Surgery
Another series of unnecessary deaths was caused by various bans on elective surgeries across the U.S. (also see here), and we’re now in danger of repeating that mistake. These bans were thought to be helpful in preserving hospital capacity, but hospitals were significantly underutilized for much of the pandemic. Add to that the fright inspired by official reaction to C19, which keeps emergency rooms empty, and you have a universe of diverse public health problems to grapple with. As I said on this blog a couple of months ago:
“… months of undiagnosed cardiac and stroke symptoms; no cancer screenings, putting patients months behind on the survival curve; deferred procedures of all kinds; run-of-the-mill infections gone untreated; palsy and other neurological symptoms anxiously discounted by victims at home; a hold on treatments for all sorts of other progressive diseases; and patients ordinarily requiring hospitalization sent home. And to start back up, new health problems must compete with all that deferred care. Do you dare tally the death and other worsened outcomes? Both are no doubt significant.”
Lockdowns
The lockdowns were unnecessary and ineffectual in their ability to control the spread of the virus. A study of 50 countries published by The Lancet last week found the following:
“Increasing COVID-19 caseloads were associated with countries with higher obesity … median population age … and longer time to border closures from the first reported case…. Increased mortality per million was significantly associated with higher obesity prevalence … and per capita gross domestic product (GDP) …. Reduced income dispersion reduced mortality … and the number of critical cases …. Rapid border closures, full lockdowns, and wide-spread testing were not associated with COVID-19 mortality per million people.”
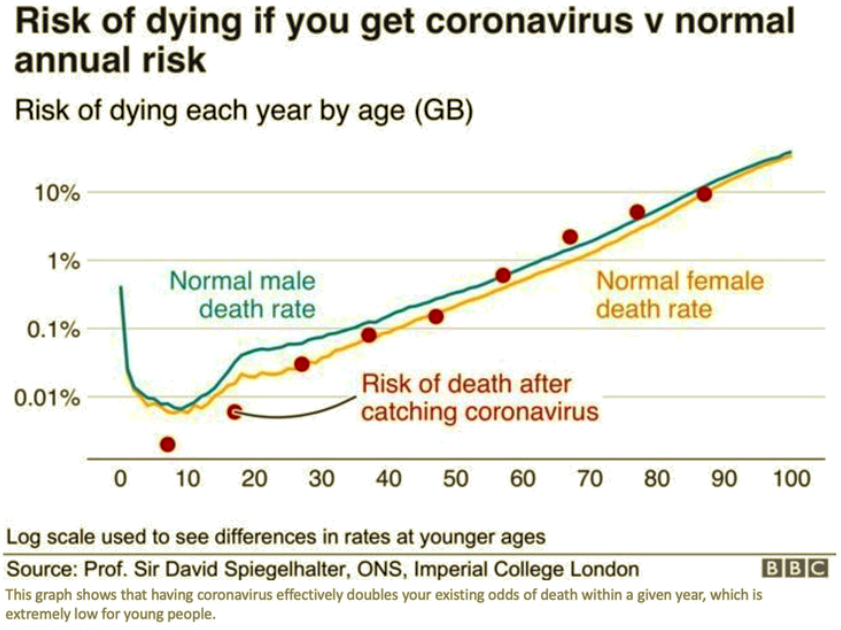
That should have been obvious for a virus that holds little danger for prime working-age cohorts who are most impacted by economic lockdowns.
Like the moratoria on elective surgeries, lockdowns did more harm than good. Livelihoods disappeared, business were ruined, savings were destroyed, dreams were shattered, isolation set in, and it continues today. These kinds of problems are strongly associated with health troubles, family dysfunction, drug and alcohol abuse, and even suicide. It’s ironic that those charged with advising on matters pertaining to public health should focus exclusively on a single risk, recommending solutions that carry great risk themselves without a second thought. After all, the protocol in reviewing new treatments sets the first hurdle as patient safety, but apparently that didn’t apply in the case of shutdowns.
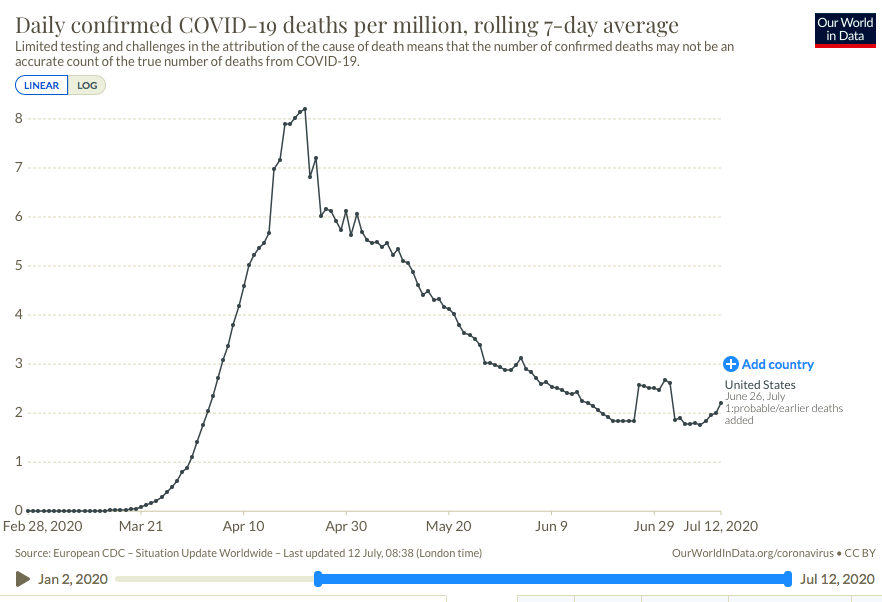
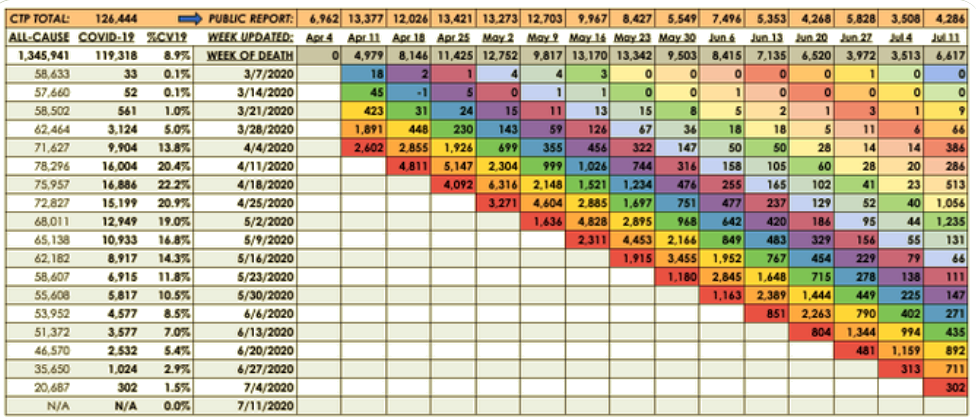
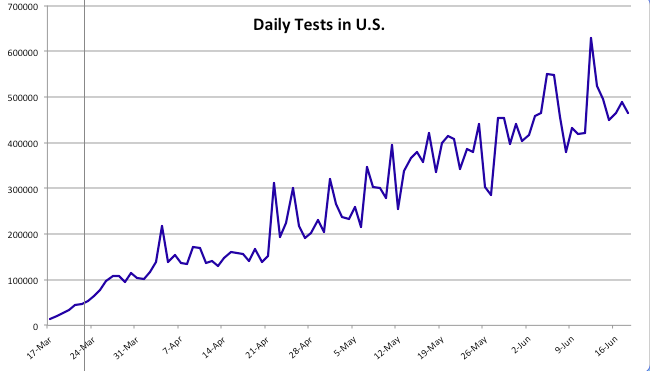
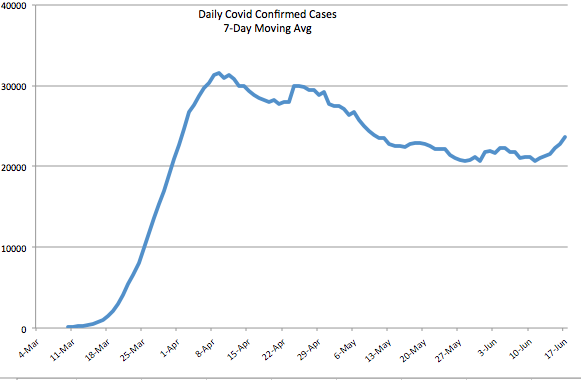
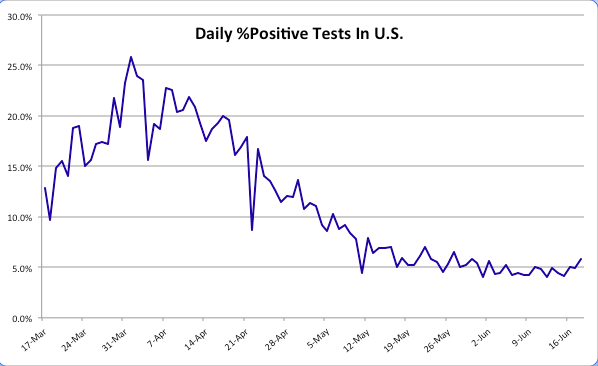
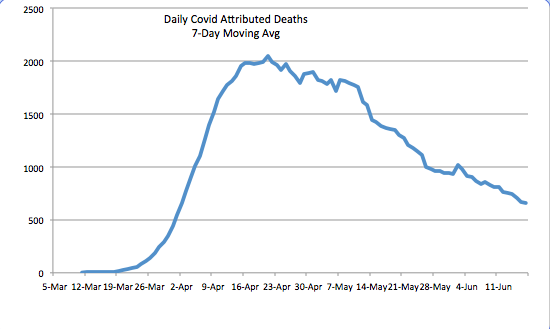
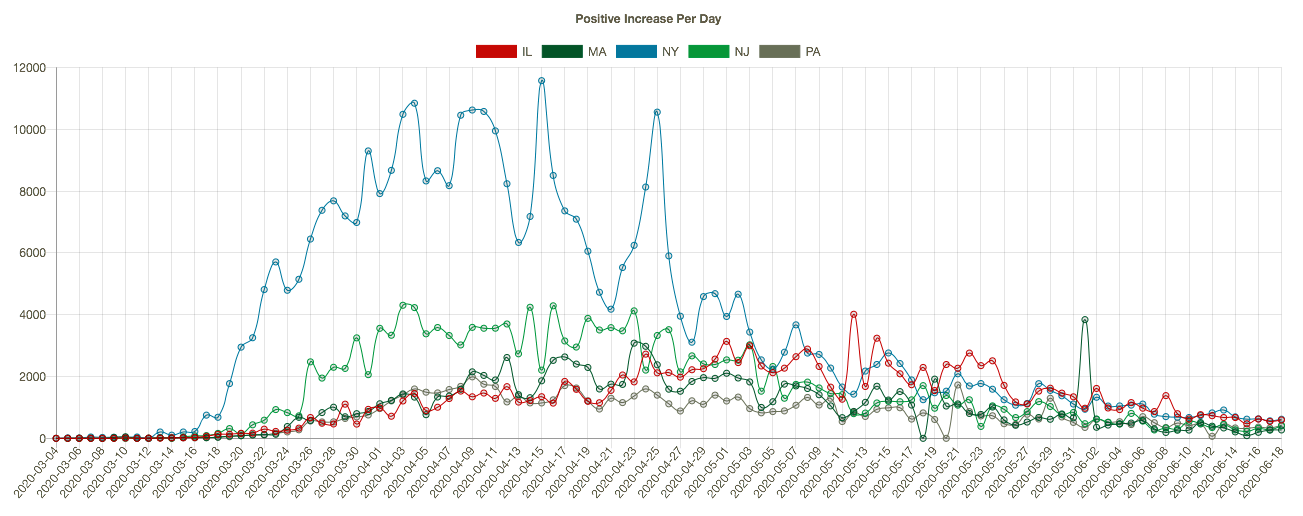
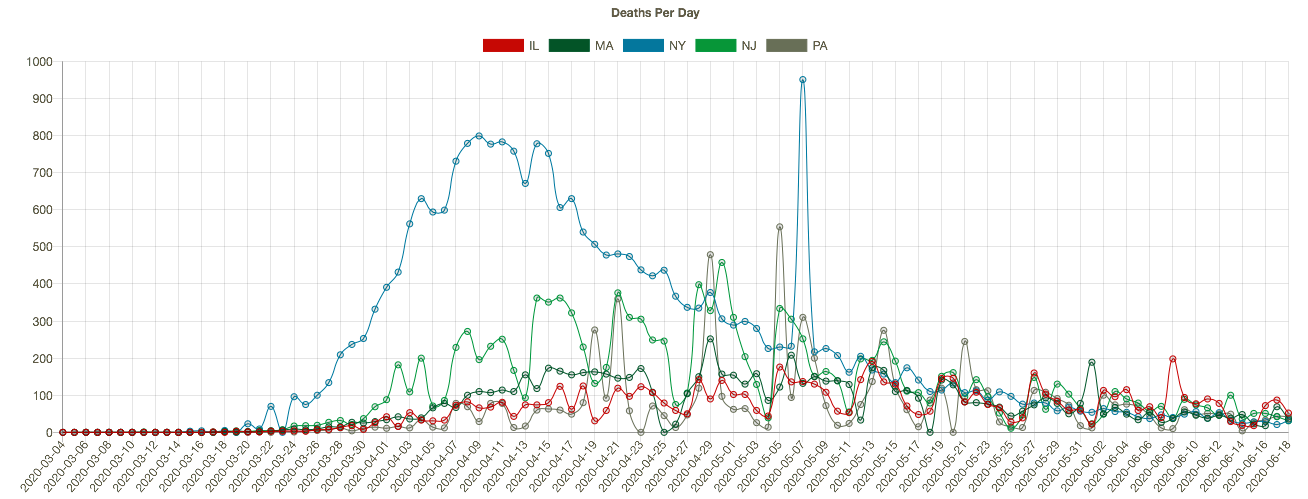
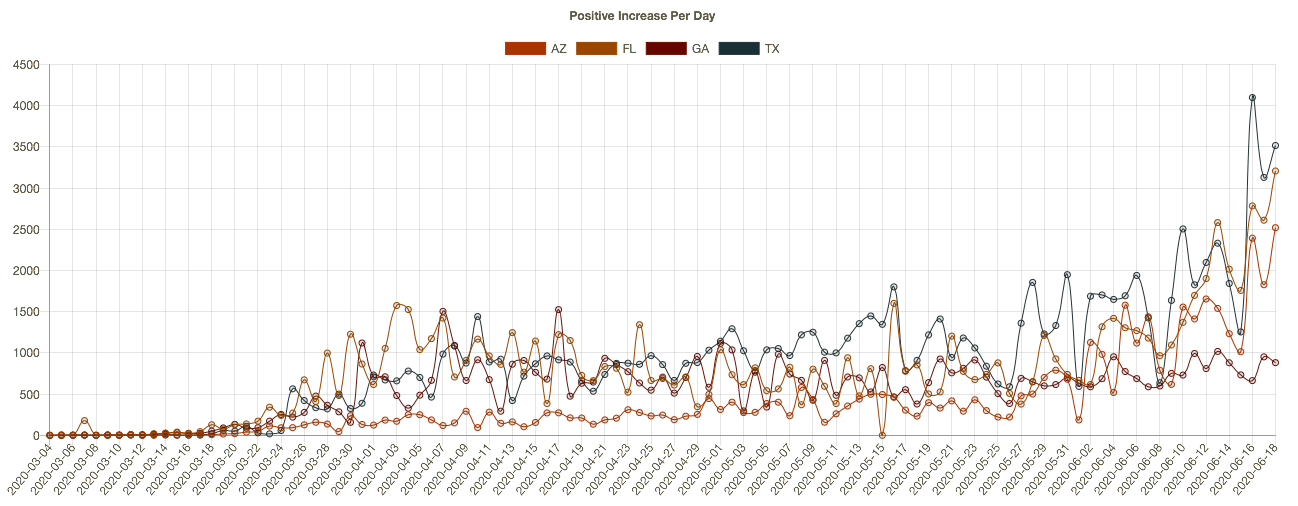
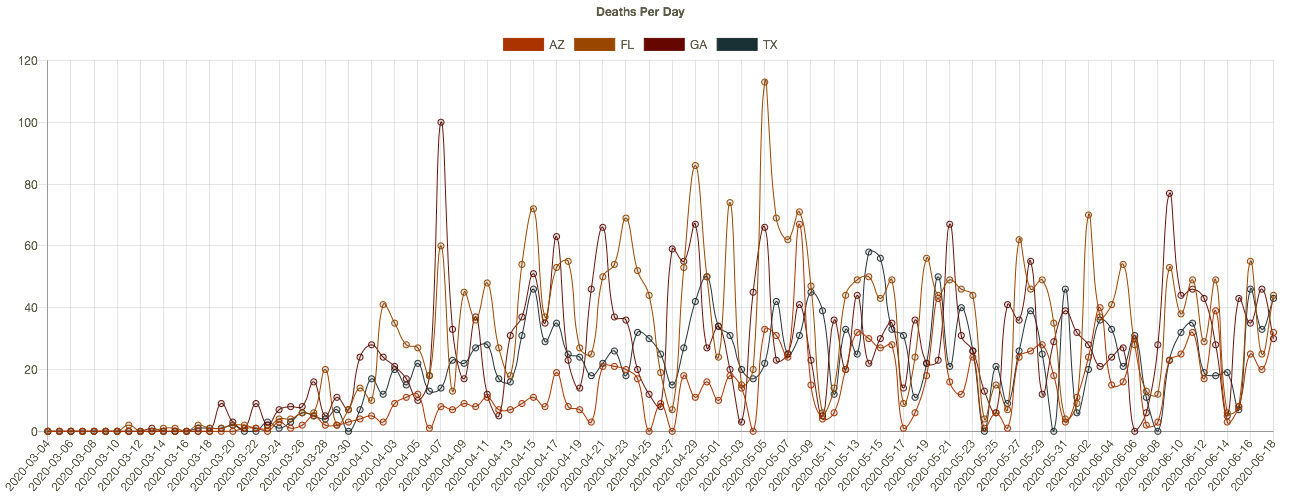
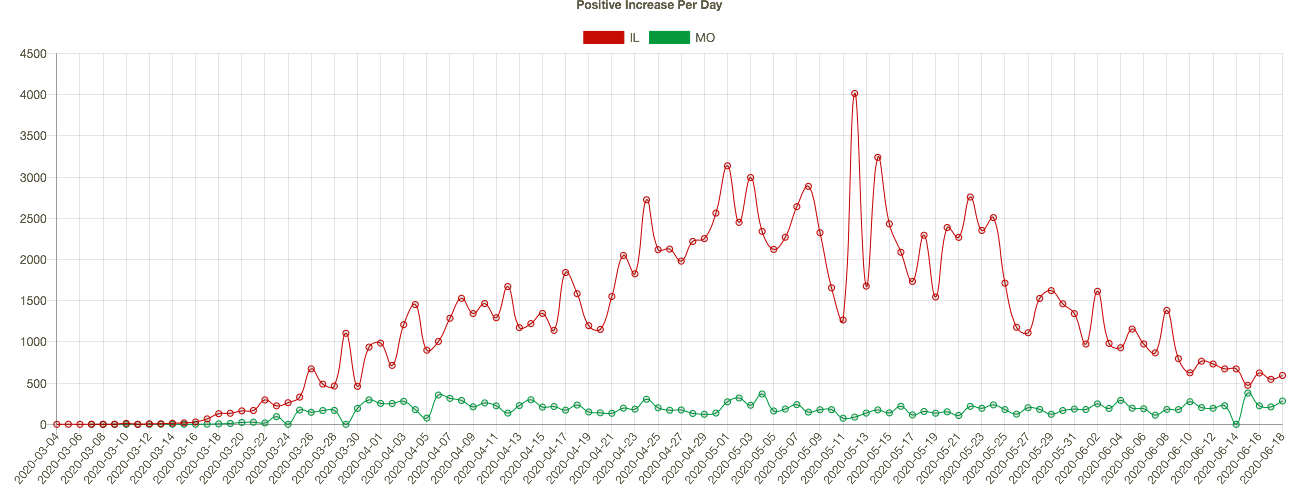
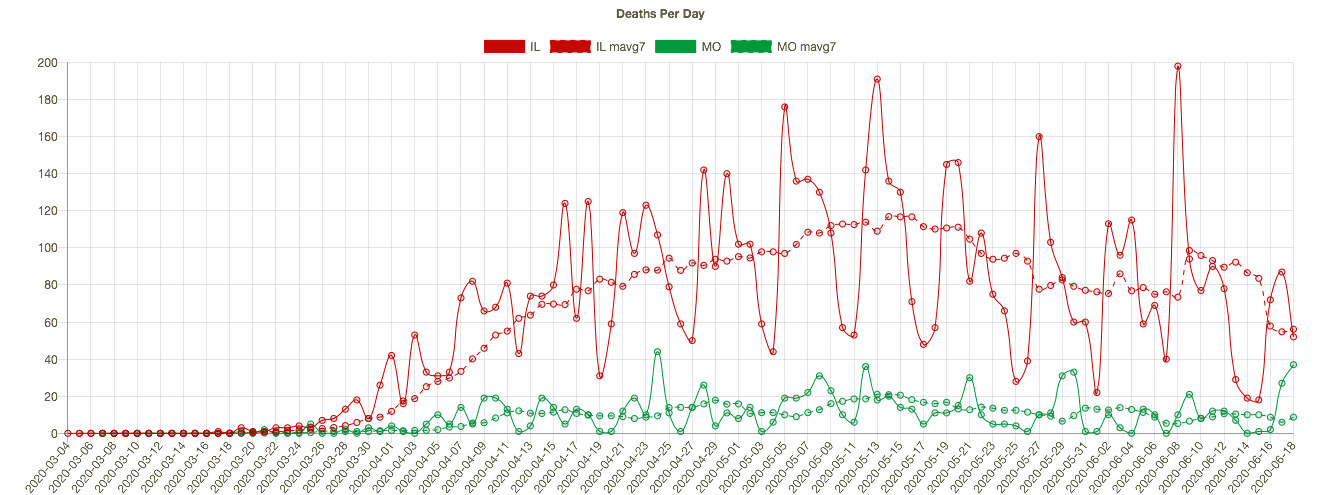
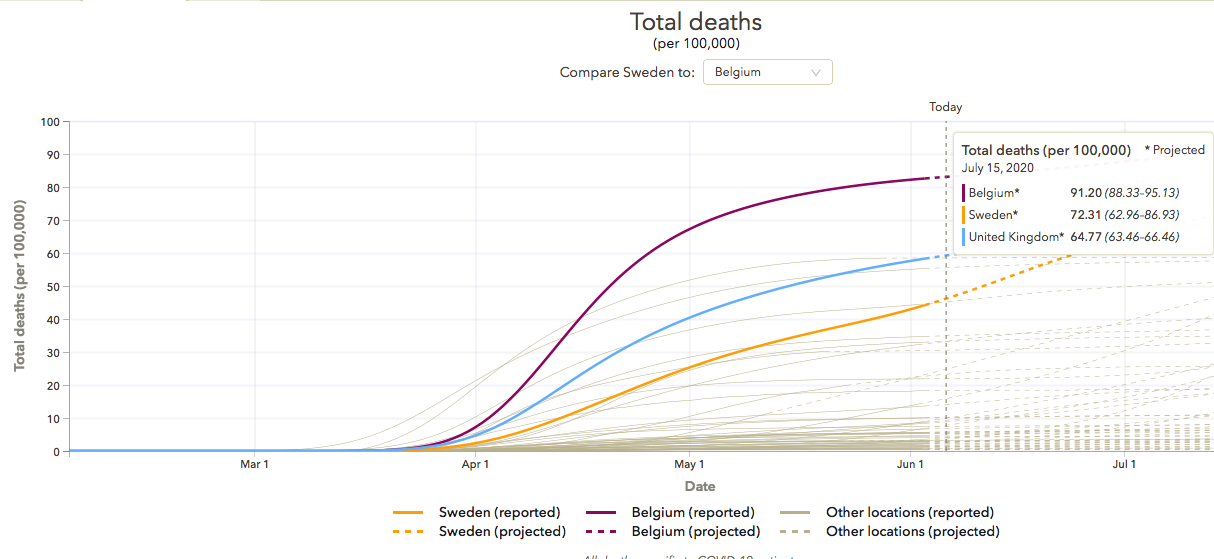
Even as efforts were made to reopen, faulty epidemiological models were used to predict calamitous outcomes. While case counts have risen in many states in the U.S. in June and July, deaths remain far below model predictions and far below deaths recorded during the spring in the northeast.
One last note: I almost titled this post “Attack of the Killer Morons”, but as a concession to what is surely a vain hope, I decided not to alienate certain readers right from the start.