Tags
Antigenic Drift, CARES Act, Coronavirus, Covid-19, Death Laundering, Europe, False Positives, Hospital Reimbursement, IFR, Immunity, Infection Fatality Rate, Kyle Lamb, Medicare, Seasonality, Second Wave, Twitter, Vitamin D, WHO
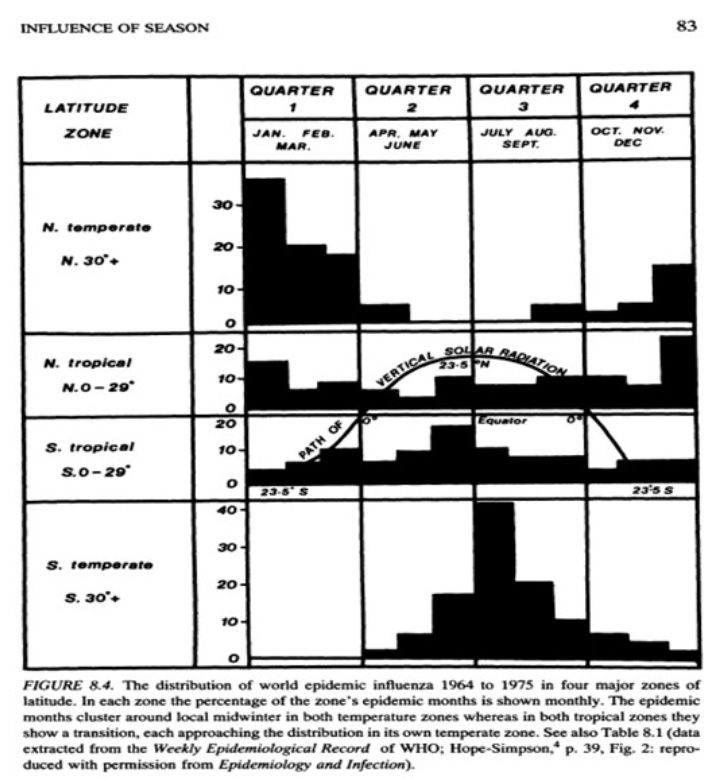
We’ve known for some times that COVID-19 (C19) follows seasonal patterns typical of the flu, though without the flu’s frequent antigenic drift. Now that we’re moving well into autumn, we’ve seen a surge in new C19 case counts in Europe and in a number of U.S. states, especially along the northern tier of the country.
The new case surge began in early to mid-September, depending on the state, and it’s been coincident with another surge in tests. From late July through early October, we had a near doubling in the number of tests per positive in the U.S. An increase in tests also accompanied the previous surge during the summer, which claimed far fewer lives than the initial wave in the early spring. In the summer, infections were much more prevalent among younger people than in the spring. Vitamin D levels were almost certainly higher during the summer months, our ability to treat the virus had also improved, and immunities imparted by prior infections left fewer susceptible individuals in the population. We have many of those advantages now, but D levels will fade as the fall progresses.
As for the new surge in cases, another qualification is that false positives are still a major testing problem; they inflate both case counts and C19-attributed deaths. In the absence of any improvement in test specificity, of which there is no evidence, the exaggeration caused by false positives grows larger as testing increases and positivity rates fall. So take all the numbers with that as a caveat.
How deadly will the virus be this fall? So far in Europe, the trends look very promising. Kyle Lamb provided the following charts from WHO on Twitter yesterday. (We should all be grateful that Twitter hasn’t censored Kyle yet, because he’s been a force in exposing alarmism in the mainstream media and among the public health establishment.) Take a look at these charts, and note particularly the lag between the first wave of infections and deaths, as well as the low counts of deaths now:
















If the lag between diagnosis and death is similar now to the spring, Europe should have seen a strong upward trend in deaths by now, yet it’s hardly discernible in most of those countries. The fatality rates are low as well:

As Lamb notes, the IFRs in the last column look about like the flu, though again, the reporting of deaths and their causes are often subject to lags.
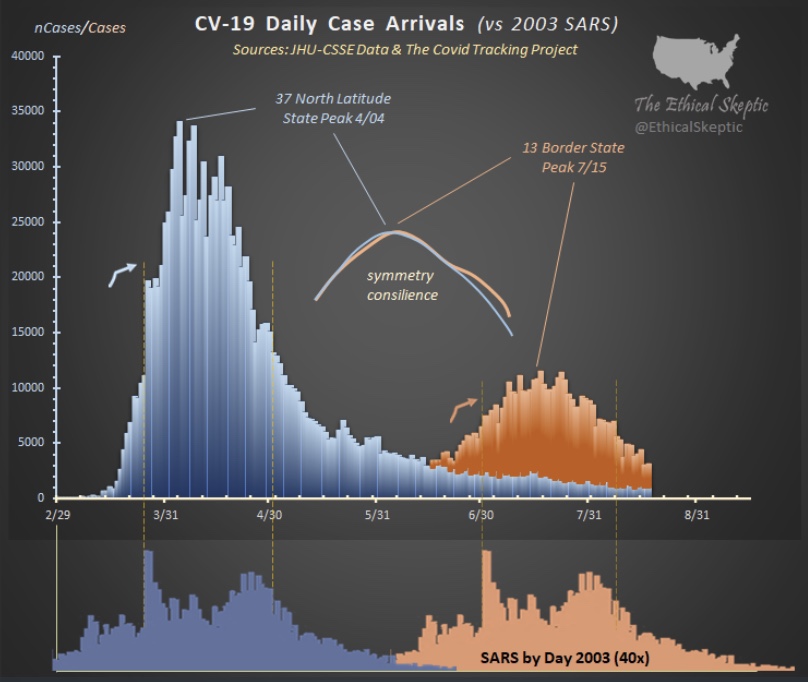
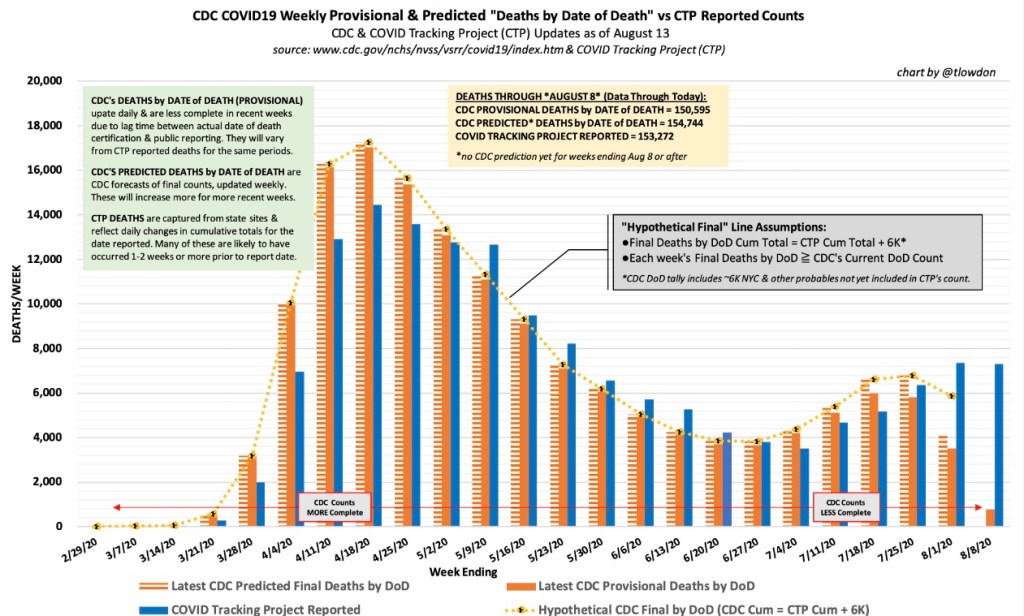
What about the U.S.? Nationwide, C19 cases and attributed death reports declined after July. See the chart below. More recently, reported deaths have stabilized at under 700 per day. Note again the relatively short lags between turns in cases and deaths in both the spring and summer waves.

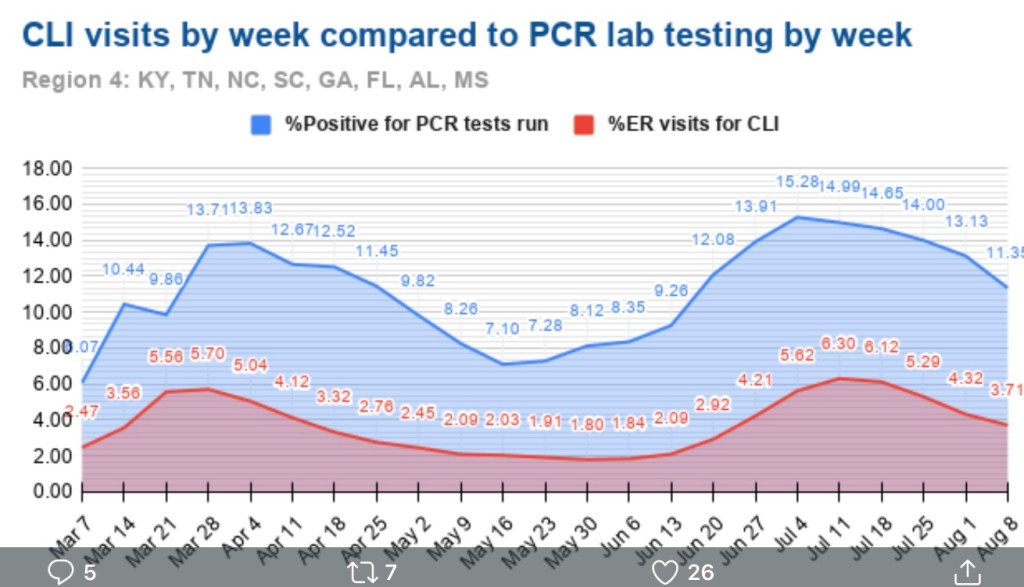
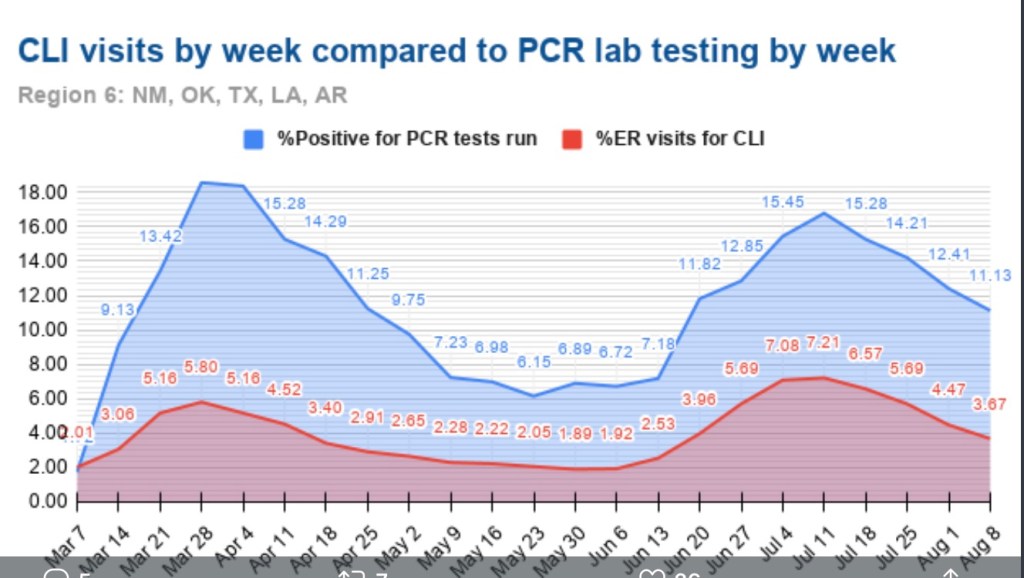
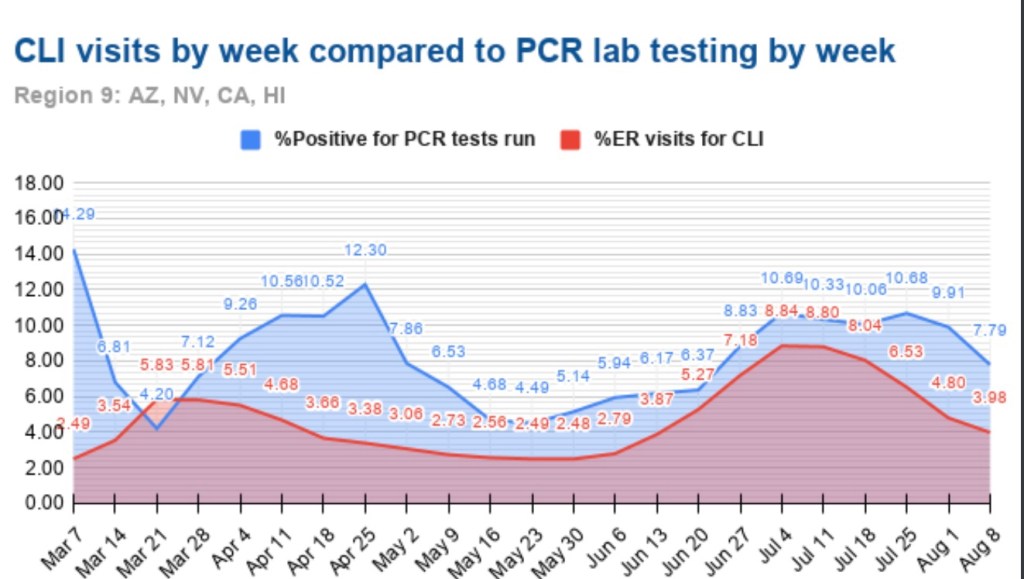
Clearly, there has been no acceleration in C19 deaths corresponding to the recent trend in new cases. Northeastern states that had elevated death rates in the spring saw no resurgence in the summer; southern states that experienced a surge in the summer have now enjoyed taperings of both cases and deaths. But with each season, the virus seems to roll to regions that have been relatively unscathed to that point. Now, cases are surging in the upper Midwest and upper mountain states, though some of these states are lightly populated and their data are thin.
A few state charts are shown below, but trends in deaths are very difficult to tease out in some cases. First, here are new cases and reported deaths in Michigan, Wisconsin, and Minnesota. There is a clear uptrend in cases in these states along with a very slight rise in deaths, but reported deaths are very low.


Next are Idaho, Montana, North Dakota, and South Dakota. A slight uptrend in cases began as early as August. Idaho and Montana have had few deaths, so they are not plotted in the second chart. The Dakotas have had days with higher reported deaths, and while the data are thin and volatile, the visual impression is definitely of an uptrend in deaths.


The following states are somewhat more central in latitude: Colorado, Illinois, and Ohio. There is a slight upward trend in new cases, but not deaths. Illinois is experiencing its own second wave in cases.


Out of curiosity, I also plotted Massachusetts, Pennsylvania, and New Jersey, all of which suffered in the first wave during the spring. They are now experiencing uptrends in cases, especially Massachusetts, but deaths have been restrained thus far.


The upshot is that states having little previous exposure to the virus are seeing an uptrend in deaths this fall. The same does not seem to be happening in states with significant prior exposure, at least not yet.
There are major questions about the reasons for the lingering death counts in the U.S.. But consider the following: first, the infection fatality rate (IFR) keeps falling, despite the stubborn level of daily reported deaths. Second, deaths reported have increasingly been pulled forward from deaths that actually occurred in the more distant past. This sort of “laundering” lends the appearance of greater persistence in deaths than is real. Third, again, false positives exaggerate not just cases, but also C19 deaths. Hospitals test everyone admitted, and patients who test positive for C19 are reimbursed at higher rates under the CARES Act; Medicare reimburses at a higher rates for C19 patients as well.
We’re definitely seeing a seasonal upswing in C19 infections in the US., now going on five weeks. In Europe, the surge in cases began slightly earlier. However, in both Europe and the U.S., these new cases have not yet been associated with a meaningful surge in deaths. The exceptions in the U.S. are the low-density upper mountain states, which have had little prior exposure to the virus. The lag between cases and deaths in the spring and summer was just two to three weeks, and while it’s too early to draw conclusions, the absence of a surge in deaths thus far bodes well for the IFR going forward. If we’re so fortunate, we can thank a combination of factors: a younger set of infecteds, earlier detection, better treatment and therapeutics, lower viral loads, and a subset of individuals who have already gained immunity.